

Percutaneous Antegrade Retrieval of an Atrial Septal Occluder Dislodged Into the Left Ventricle
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
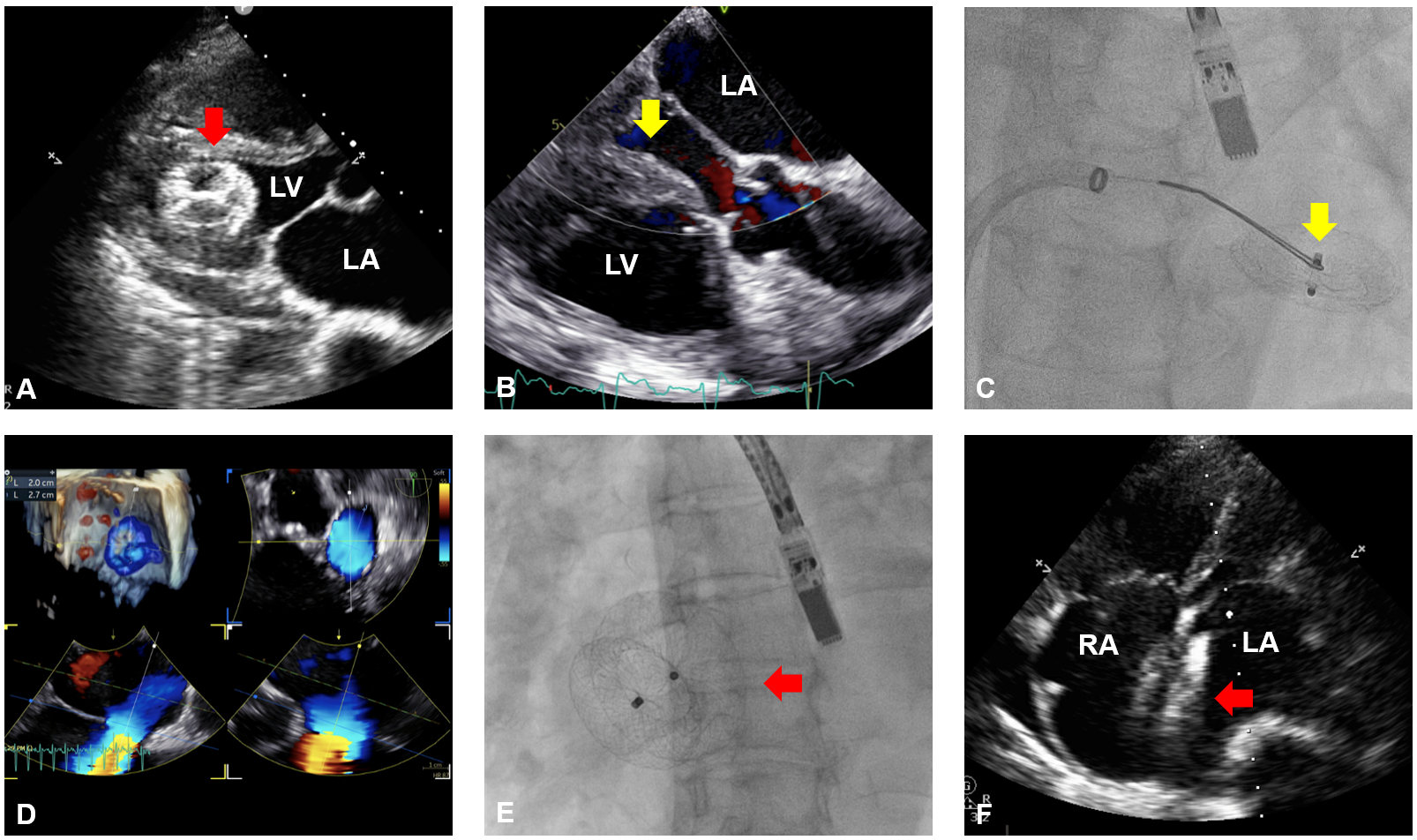
A 76-year-old woman with atrial septal defect (ASD) had previously undergone occluder implantation at another institution. At that time, preoperative transesophageal echocardiography (TEE) revealed an ASD measuring 2.0 x 2.5 cm with deficient retro-aortic rim. Transcatheter closure using a 24-mm Amplatzer Septal Occluder (Abbott) was performed. One month post-procedure, the device was found dislodged into the left ventricle (LV) (Figure A).
She was referred to our hospital for retrieval. The multidisciplinary heart team recommended percutaneous retrieval, reserving surgical treatment as a backup option. The procedure was performed under local anaesthesia with a 3-dimensional mini-TEE (9VT-D probe; GE Healthcare), which has a smaller tip for better tolerance under sedation. The connection hub of the occluder was found to face the mitral orifice, presenting a favorable orientation for antegrade retrieval (Figure B). A 14F Fustar steerable sheath (Lamed GmbH) was advanced into the left atrium through the ASD. Although a 9F sheath is minimally sufficient for a 24-mm occluder, a larger 14F sheath was chosen to ensure adequate oversizing. Subsequently, a 7F multipurpose angiographic catheter equipped with a 20-mm gooseneck snare was advanced into the LV (Video 1). The screw hub of the occluder was successfully snared (Figure C, Video 2), re-sheathed, and extracted.
Upon reassessment, the maximal ASD size was measured at 27 mm (Figure D). A 32-mm Amplatzer Septal Occluder was successfully implanted (Figure E). Echocardiography at 3 months demonstrated stable device positioning, absence of residual shunt, and trivial mitral regurgitation (Figure F).
Conventionally, LV-displaced occluders necessitate open surgical retrieval because of risks of LV outflow-tract obstruction and mitral valve damage during percutaneous approaches. This case demonstrates the feasibility of a primary antegrade approach.
Affiliations and Disclosures
Yee-Tat Lee, MBBS1,2; Tsun-Ho Lam, MBBS1,2; Lap-Tin Lam, MBBS1,3; Kwong-Yue Eric Chan, MBBS1,2,3; Yui-Ming Lam, MBBS1,2; Simon Cheung-Chi Lam, MBBS1,2; Chun-Ka Wong, MBBS1,2,4; Ka-Chun Un, MBBS MRes(Med)1,2
From the 1Cardiology Division, Department of Medicine, Li Ka Shing Faculty of Medicine, The University of Hong Kong, Hong Kong SAR, China; 2Cardiology Division, Department of Medicine, Queen Mary Hospital, Hong Kong SAR, China; 3Cardiac Medical Unit, Grantham Hospital, Hong Kong SAR, China; 4Cambridge Stem Cell Institute, University of Cambridge, United Kingdom.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention(s) described in the manuscript and for the publication thereof, including any and all images.
Address for correspondence: Ka-Chun Un, MBBS, MRes(Med), FRCP (London), FACC, Cardiology Division, Department of Medicine, Queen Mary Hospital, The University of Hong Kong, Hong Kong SAR, Chian. Email: drtimothyun@gmail.com; X: @timothy_un










