


Contemporary Contrast Media Dosing During Percutaneous Coronary Intervention in Patients With Pre-existing Renal Impairment
© 2025 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Editor's 2025 Top 10 Interview
Abstract
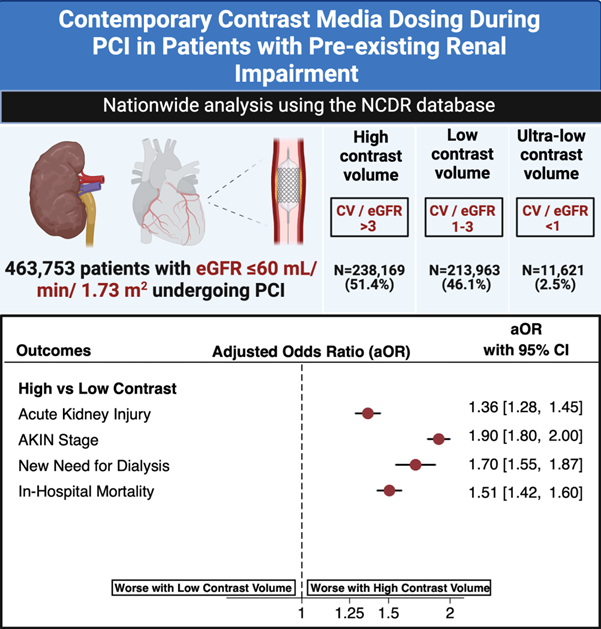
Objectives. Contrast volume minimization can mitigate acute kidney injury (AKI) risk following percutaneous coronary intervention (PCI), but national data regarding contemporary contrast volume dosing patterns are lacking. The authors analyzed data from the National Cardiovascular Data Registry (NCDR) CathPCI registry to assess the prevalence and outcomes of renal function-based contrast dosing during PCI in patients with pre-existing renal impairment.
Methods. The authors analyzed data from 463 753 patients with an eGFR ≤ 60 mL/min/1.73 m2, and categorized patients based on contrast volume/eGFR: high (> 3), low (1-3), and ultra-low (< 1). eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration creatinine equation. The primary outcome was the occurrence of AKI. Outcomes were adjusted based on covariates derived from a validated AKI prediction model.
Results. The majority (51.4%) of patients received high contrast volume. Compared with patients who received low contrast volume, patients with high contrast volume use had a significantly higher incidence of AKI (adjusted OR 1.36 [1.28 to 1.45]) and a higher stage of AKI (adjusted OR 1.90 [1.80 to 2.00]). The incidence of AKI was similar between low and ultra-low contrast volume use. The development of new need for dialysis was higher in patients who received high contrast volume (2.8%) compared with those who received low contrast volume (0.8%) and ultra-low contrast volume (0.8%) (P < .001).
Conclusions. High contrast volume during PCI is associated with worse outcomes including AKI and new need for dialysis. Our study provides further support for the use of contrast volume less than 3 times the eGFR as a target to guide contrast dosing during PCI.
Introduction
Acute kidney injury (AKI) is a common complication of percutaneous coronary intervention (PCI) and is associated with increased mortality, prolonged hospitalization, and higher costs.1,2 The identification of high-risk patients, contrast minimization, and peri-procedural hydration are the 3 key strategies recommended to prevent contrast-related AKI.3-6 Prior regional studies have shown that limiting the administered contrast volume to less than 3 times the calculated creatinine clearance is associated with a lower risk of developing AKI.7-10 In addition, some clinicians have demonstrated both the efficacy and superior outcomes associated with the administration of ultra-low contrast volume (contrast volume use ≤ creatinine clearance).11-13
Observational studies have also demonstrated a reduction in AKI rates following a reduction in total contrast volume.7-10 However, national data regarding contemporary contrast dosing practice in PCI are lacking. Therefore, we analyzed data from the National Cardiovascular Data Registry (NCDR) to assess the prevalence, predictors, and outcomes of renal function-based contrast dosing during PCI in patients with pre-existing renal impairment.
Methods
Study population and design
The study population consisted of patients undergoing index PCI at hospitals participating in the National Cardiovascular Data Registry (NCDR) CathPCI Registry between April 1, 2018 and June 30, 2022. The CathPCI Registry, a quality improvement initiative of the American College of Cardiology in partnership with the Society of Cardiovascular Angiography and Interventions, captures data from patients undergoing cardiac catheterization and/or PCI. Baseline demographic, clinical, and procedural characteristics as well as in-hospital outcomes are collected from more than 1600 hospitals across the country. Details regarding the registry’s organization, data collection, and monitoring process have been published previously.14,15
The study was designed by the authors and approved and funded by the NCDR. The need for informed consent was waived, as the CathPCI Registry collects data without individual patient identifiers. The analyses were performed by the Duke Clinical Research Institute. The authors R.Y. and D.M.W. reviewed the analyses and vouched for the accuracy and completeness of the study.
For this study, we included adult patients with pre-existing moderate to severe renal impairment (defined as estimated glomerular filtration rate [eGFR] ≤ 60 mL/min/1.73 m2) undergoing elective or emergent PCI. The eGFR was calculated using the updated Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) creatinine equation, a race-neutral equation now recommended by various professional societies.16 We excluded patients (1) whose pre or post-procedure creatinine values were missing, (2) who died in the catheterization lab, (3) who were undergoing coronary artery bypass grafting during the same admission, (4) whose baseline risk of AKI could not be predicted due to missing variables, (5) who were already on dialysis at the time of presentation, and (6) who were missing contrast volume or whose contrast volume was listed as 0.
Study variables
The study population was divided into 3 cohorts: high contrast volume use (contrast volume/eGFR > 3), low contrast volume use (contrast volume/eGFR 1-3), and ultra-low contrast volume use (contrast volume/eGFR < 1). Patient demographics and clinical, procedural, and operator characteristics were described. The primary outcome of interest was the occurrence of AKI, defined as greater than or equal to 0.3 mg/dL absolute or greater than or equal to a 1.5-fold relative increase in post-PCI creatinine.17,18 Peak value within 7 days of the procedure was considered the post-PCI creatinine. Secondary outcomes studied included the stage of AKI based on the Acute Kidney Injury Network (AKIN) definition and the new requirement of dialysis during the admission.
Statistical analysis
All analyses were performed using SAS version 9.4 (SAS Institute). Given the large sample size, the baseline characteristics were compared using absolute standardized difference percentages. A 10% or greater absolute standardized difference percentage was considered a potentially meaningful difference. The low-contrast-volume cohort was identified as the reference group for comparison with the ultra-low-volume and high-contrast-volume cohorts.
For each binary outcome, a logistic regression model was used for reporting the odds ratio (OR) and 95% CI. The AKIN stage was treated as an ordinal outcome. Therefore, the association between contrast group and AKIN stage was assessed using ordinal logistic regression. The proportional odds assumption was tested using the Score Test, and the criteria for proportional odds were satisfied. The OR was presented for having a 1-unit worse (higher) AKIN stage. Predicted probabilities are also shown. Contrast level was a 3-category variable: ultra-low, low, and high contrast volume as defined above. The comparison groups were ultra-low vs low contrast volume and high vs low contrast volume. Tukey’s adjustment method was employed to account for multiple comparisons between the groups. We also reported the adjusted OR with the adjustment covariates derived from a prior AKI prediction model developed using the NCDR CathPCI database.19 These covariates included age, prior cerebrovascular disease, prior heart failure, diabetes, chronic kidney disease severity, anemia, indication for PCI (non-ST-segment elevation myocardial infarction [NSTEMI] vs ST-segment elevation myocardial infarction [STEMI] vs non-acute coronary syndrome), cardiac arrest on presentation, heart failure on presentation, presence of cardiogenic shock, and the use of an intra-aortic balloon pump prior to the procedure.
Results
Patient characteristics
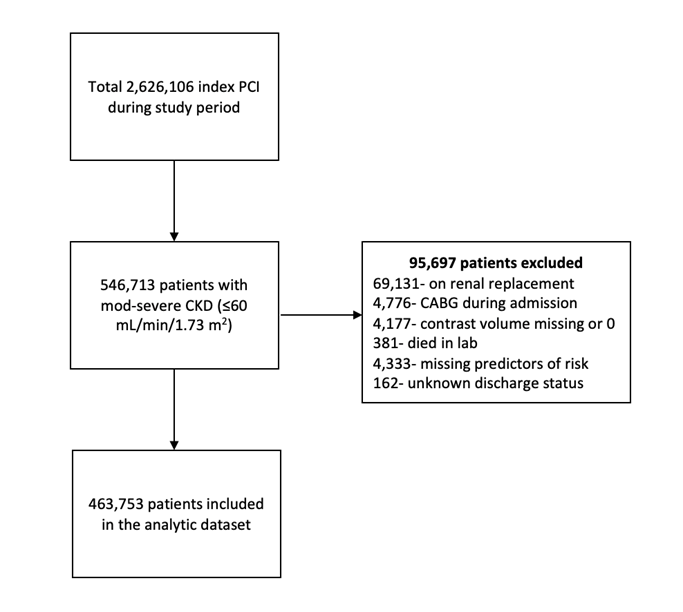
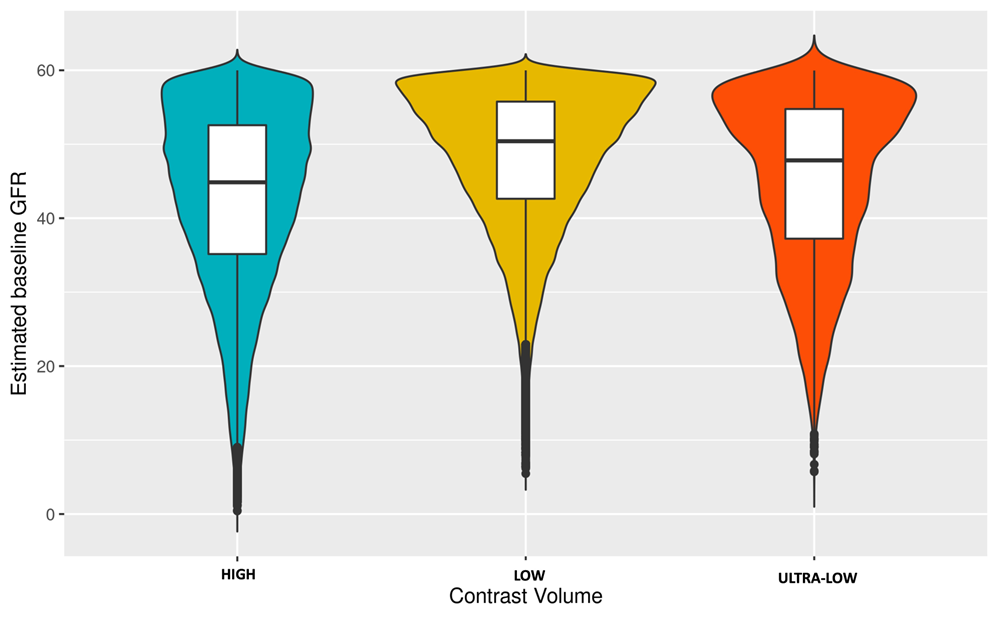
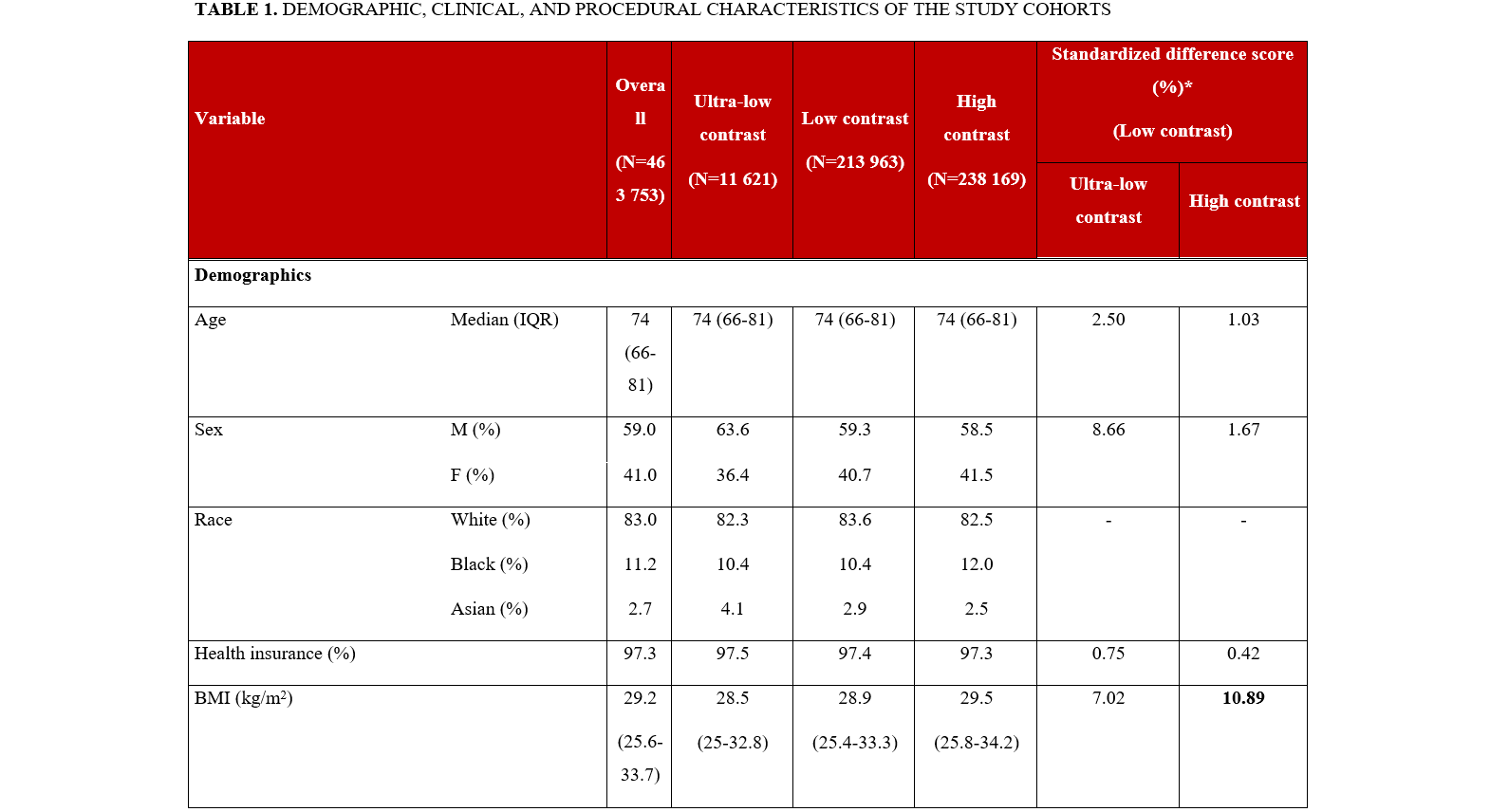
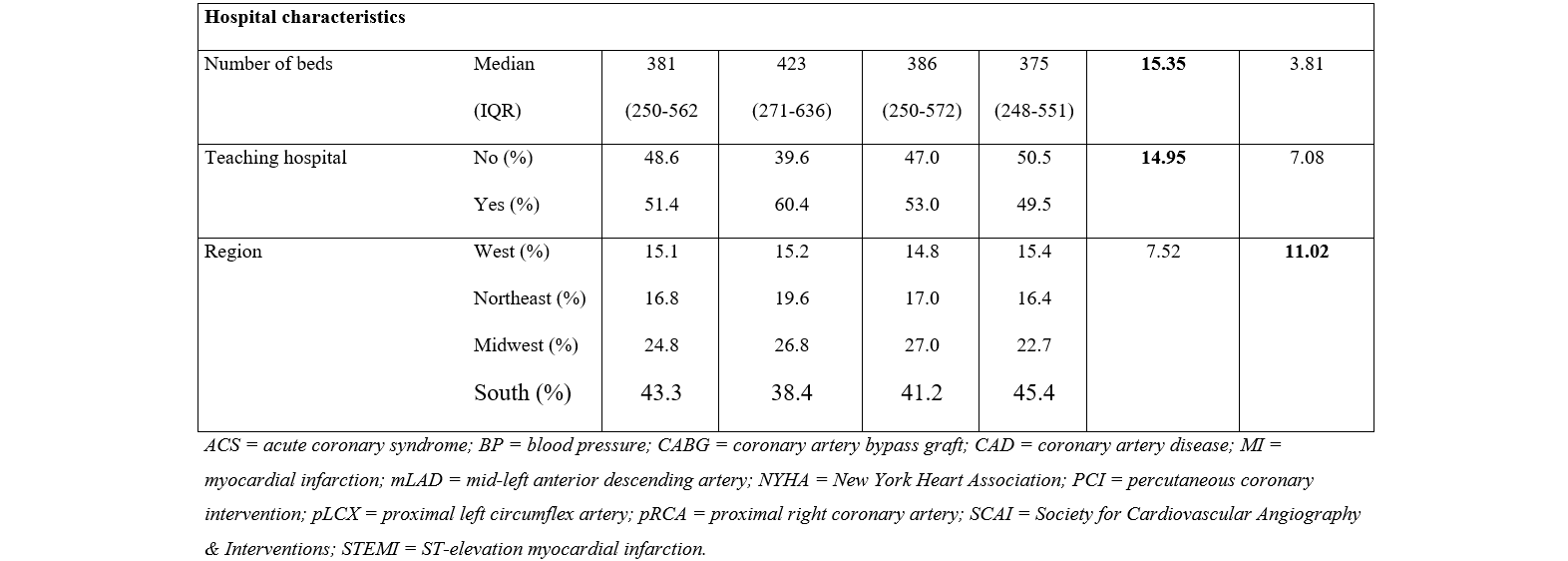
A total of 2 626 106 patients underwent a PCI during the study period, of which 619 981 did not have a pre-procedure creatinine. Of the remaining 2 006 877 patients, 546 713 (27.2%) had moderate to severe chronic kidney disease (CKD). Additionally, 95 697 patients were excluded due to the presence of 1 or more of the exclusion criteria, leaving a total of 463 753 patients in the analytic dataset (Figure 1). A slight majority (238 169, 51.4%) of patients received high contrast volume (contrast volume/eGFR > 3). Low contrast volume (contrast volume/eGFR 1-3) was used in 213 963 (46.1%) patients and ultra-low contrast volume (contrast volume/eGFR < 1) was used in 11 621 (2.5%) patients. The median age of the study population was 74 years and 190 010 (41%) were female. Minimal clinically meaningful differences were noted in the baseline demographic or clinical characteristics of the cohorts (Table 1). Baseline eGFR was comparable between all 3 groups (Figure 2). Compared with patients who received low contrast volume, patients who received ultra-low contrast volume were more likely to have had a prior PCI, undergone elective PCI, and undergone PCI for stable coronary artery disease. They were also more likely to have had PCI performed at a teaching hospital.
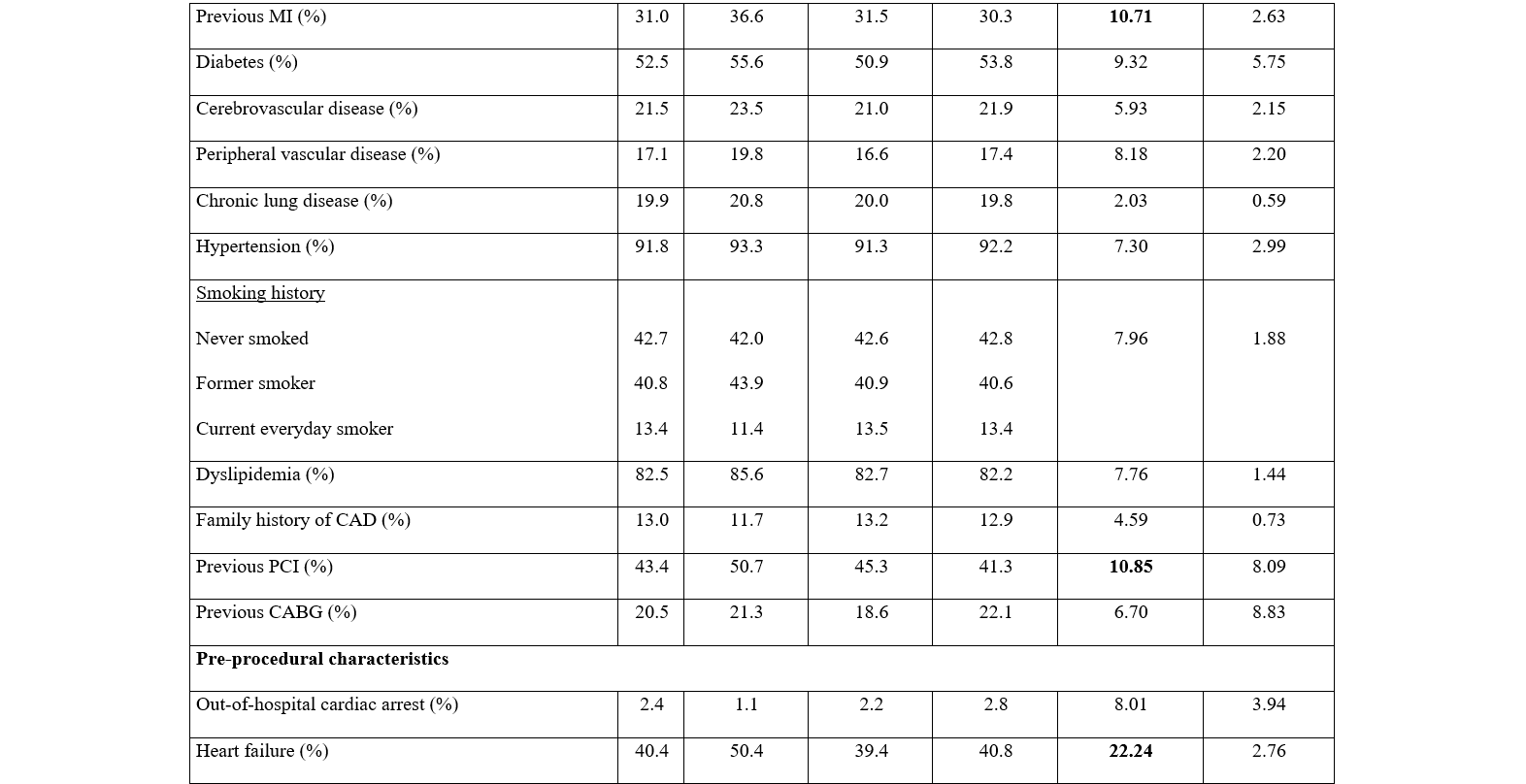
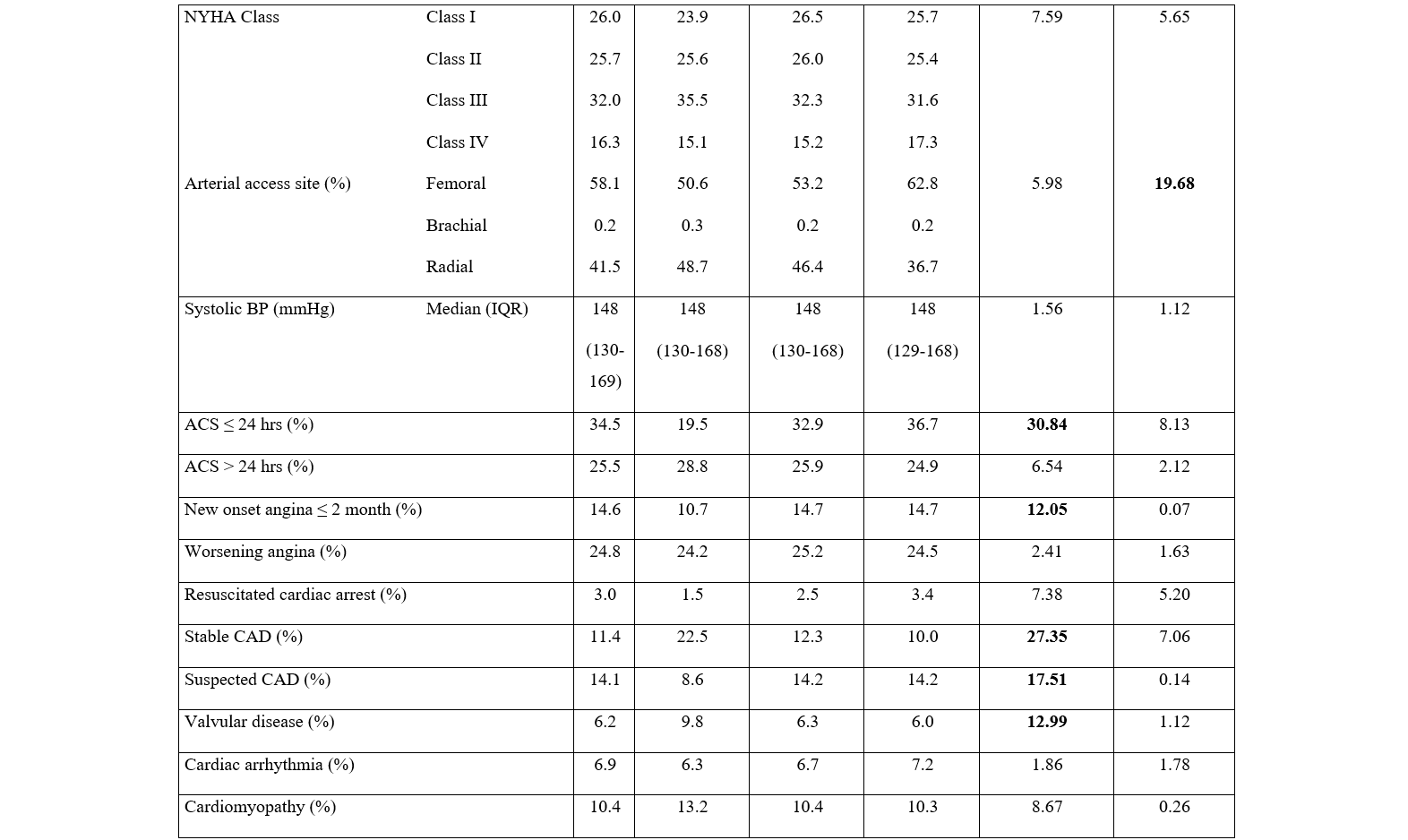
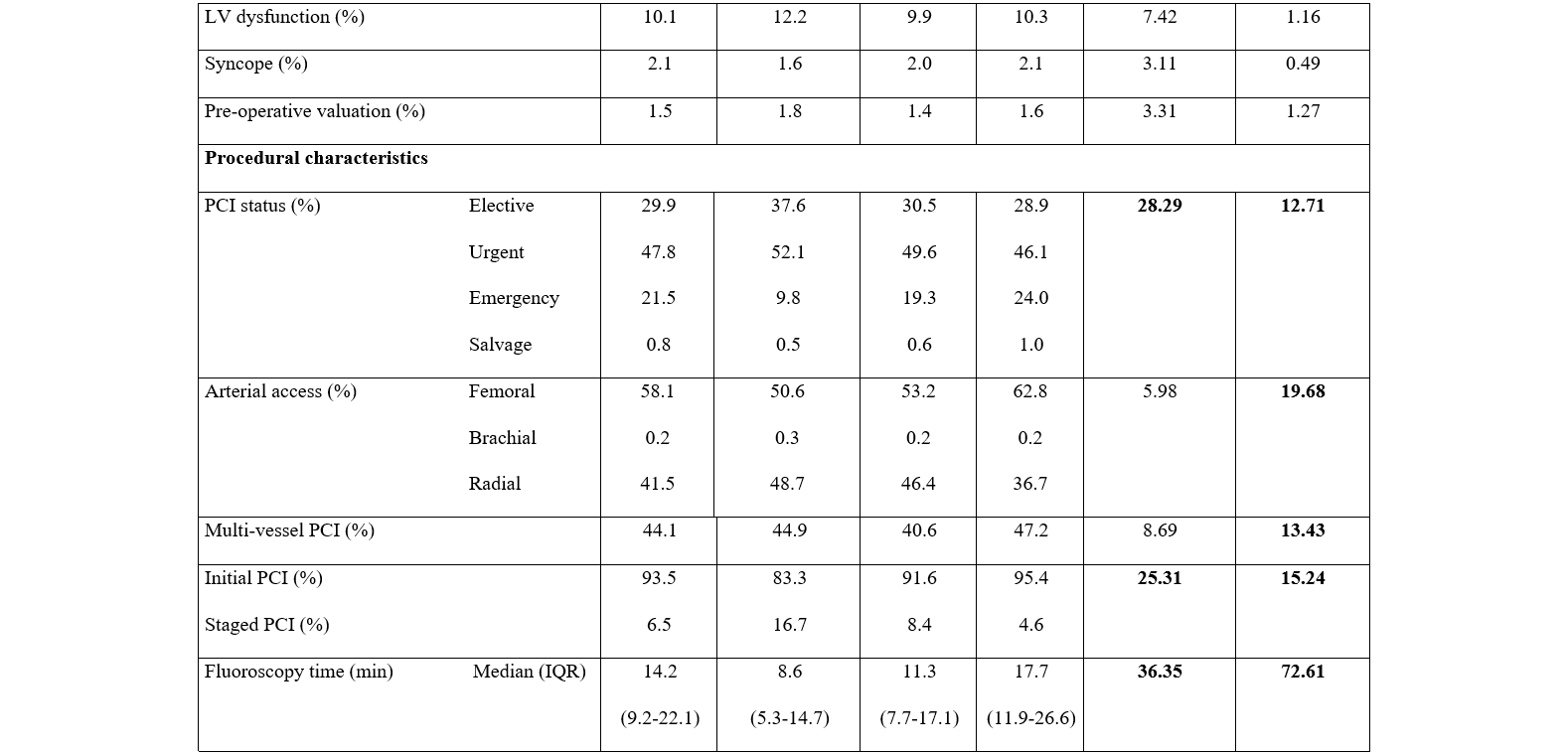
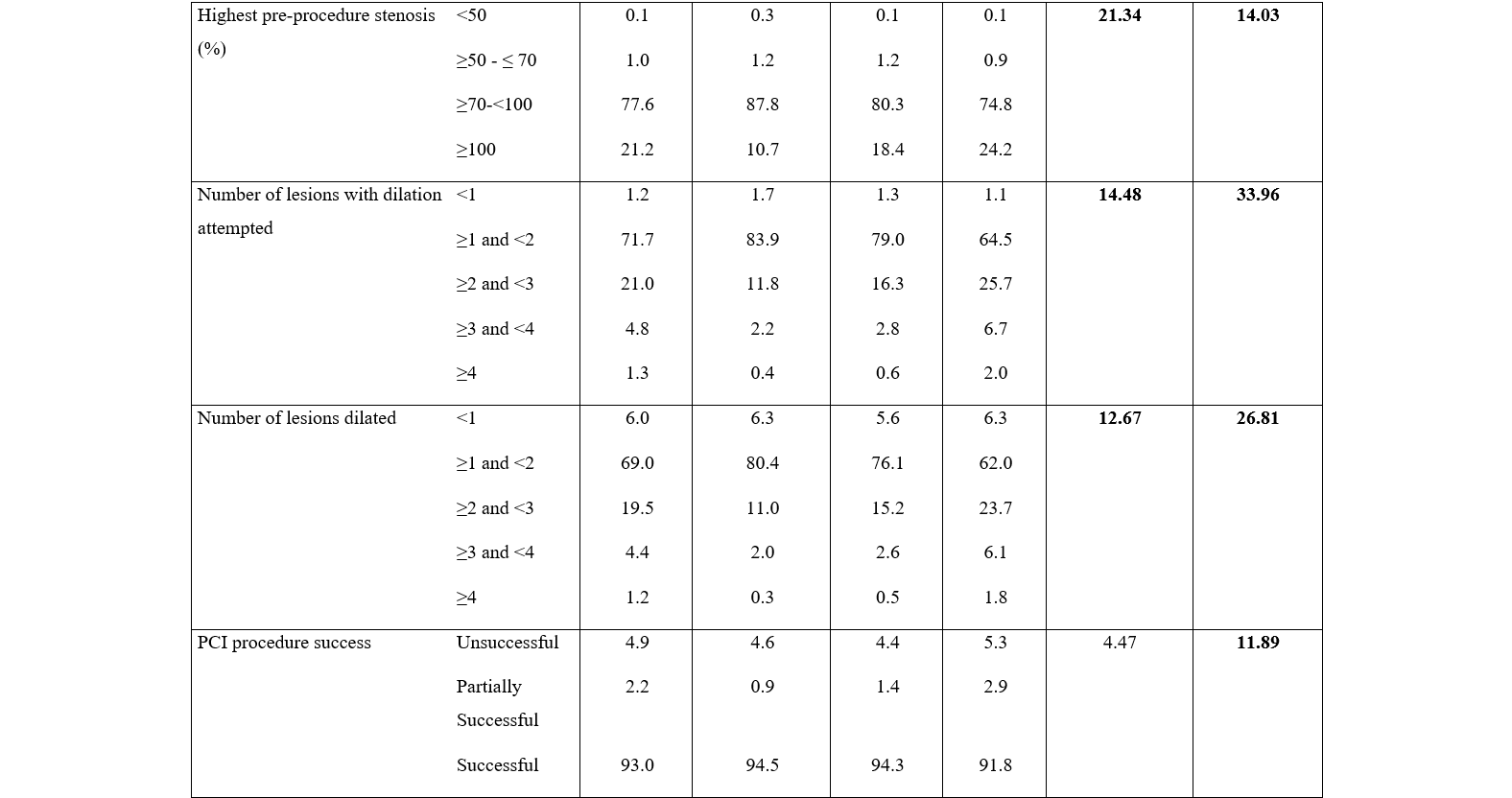
Compared with patients who received low contrast volume, patients who received high contrast volume were more likely to have emergent PCI, PCI for STEMI, and PCI for multi-vessel disease. Patients who received high contrast volume had higher complexity and severity of lesions, and a greater number of lesions dilated but a lower rate of successful PCI. They were also more likely to receive femoral arterial access, concomitant venous access, and have longer fluoroscopy times.
Primary outcome
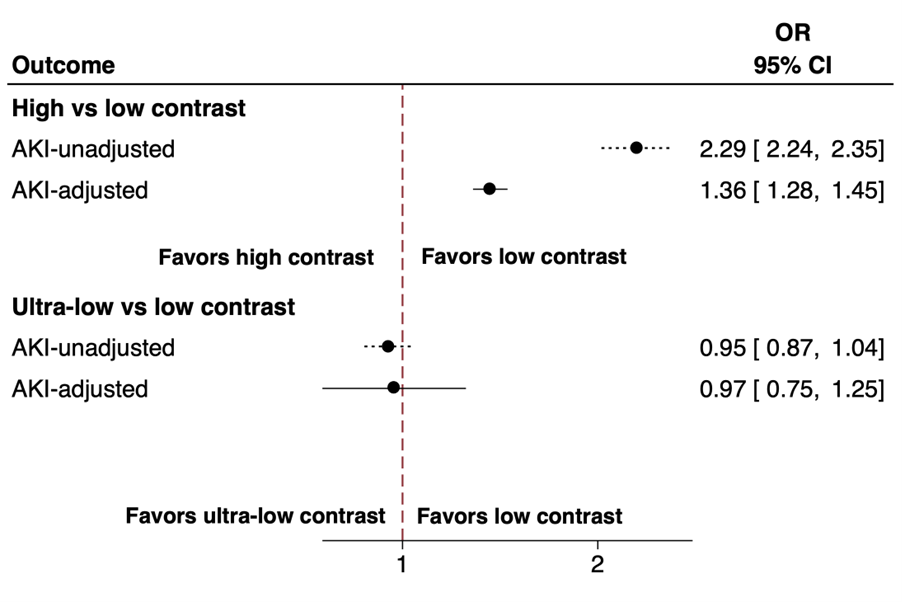
The unadjusted and adjusted incidences of AKI of the 3 cohorts are shown in Figure 3. There was no significant difference in the incidence of AKI between ultra-low vs low contrast volume use: 13.9% vs 11.1% (unadjusted OR, 0.95; 95% CI, 0.87-1.04; adjusted OR, 0.97 [0.75-1.25]). The incidence of AKI was significantly higher in patients with high contrast volume use compared with patients with low contrast volume use: 21.5% vs 11.1% (unadjusted OR, 2.29 [2.24-2.35]). The significance of this finding persisted after adjusting for important covariates (adjusted OR, 1.36 [1.28-1.45]).
Secondary outcomes
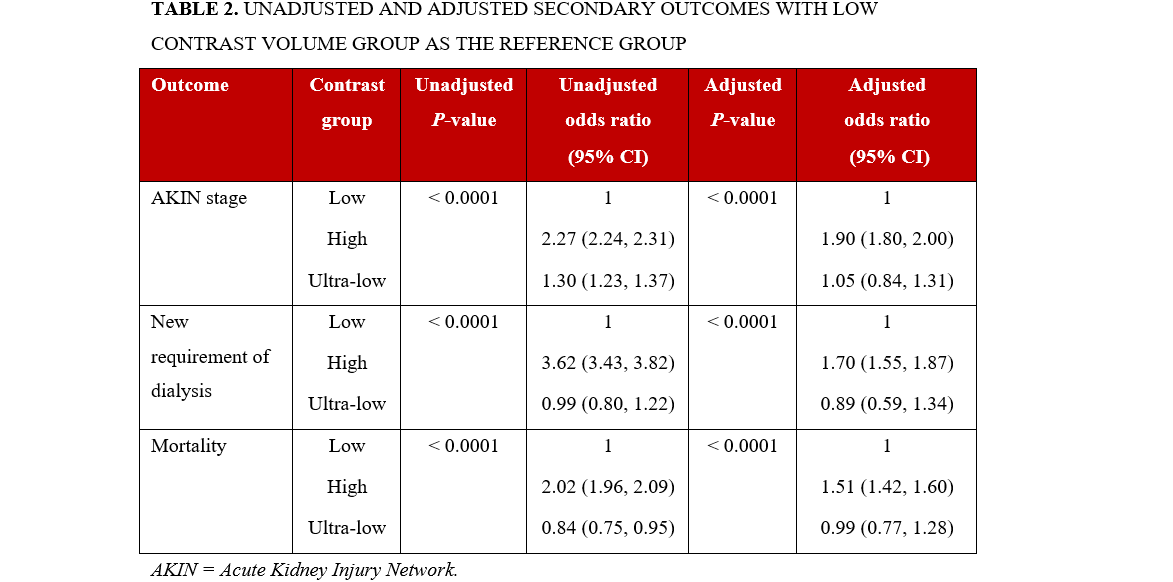
The incidence and odds ratio of secondary outcomes are displayed in Table 2. The severity of AKI defined by AKIN staging was similar between patients receiving ultra-low and low contrast volume after adjusting for covariates (adjusted OR 1.05 [0.84-1.31]). However, compared with low contrast volume use, high contrast volume use was associated with a higher AKIN stage of AKI (adjusted OR 1.90 [1.80-2.00]). Of all the patients, only 1.8% developed a new need for dialysis after undergoing PCI. This was highest in patients who received high contrast volume (2.8%) compared with low contrast volume (0.8%) and ultra-low contrast volume (0.8%) (P < .001). Similarly, although the total incidence of in-hospital mortality was low at 4.2%, the incidence of death was significantly greater in the high contrast volume group (5.5%) compared with the low contrast volume group (2.8%) and the ultra-low contrast volume group (2.4%) (P < .001).
Discussion
This study analyzed the use of renal function-based contrast dosing in almost half a million patients with moderate to severe CKD (defined as eGFR ≤ 60 mL/min/1.73 m2) undergoing PCI. The first key finding of this study was the continued use of high contrast volume in the majority of patients. Secondly, in line with prior studies, patients receiving a high dose of contrast had worse renal outcomes compared with those receiving low dose contrast. Finally, in contrast to prior work, we did not find a difference in the outcomes of those who received ultra-low compared with low dose contrast.12
There appears to be a non-linear association between renally-adjusted contrast volume administration and renal outcomes, and there is general agreement that a strategy of ‘as low as reasonably safe’ is an effective clinical approach to minimize the risk of contrast-associated AKI.7,20 Laskey et al first studied the use of the contrast volume/creatinine clearance ratio as a predictor of early post-PCI rise in creatinine and proposed a ratio greater than 3.7 as the optimal cutoff for predicting the risk of AKI.21 Subsequent studies suggested that the safer threshold for renal dosing is lower and closer to 3 times the creatinine clearance. Based on a study of 58 957 patients undergoing PCI in Michigan, our group had proposed that a planned contrast volume restricted to less than 3 times and preferably 2 times the creatinine clearance might be valuable in reducing the risk of AKI. Subsequently, this practice has been widely adopted in Michigan and by many institutions elsewhere, and is associated with reduced contrast volume use and a corresponding decrease in AKI incidence.
Similar to the PCI population, there appears to be a similar relationship between high contrast dose (defined similarly) and outcomes in patients undergoing endovascular procedures as well as those undergoing structural cardiac interventions.22,23 The argument for minimizing contrast volume, especially in high-risk patients, has been further supported by efforts to use exceedingly low volumes of contrast. Kane et al demonstrated the feasibility and lower rates of AKI associated with the use of ultra-low contrast volume in 185 patients with non-dialysis-dependent stage 3 to 5 CKD.11 This practice has also seen wider use in select hospitals and, in prior work, was demonstrated to be associated with a lower incidence of AKI compared with low-dose contrast dosing.13
Our study builds upon prior work by reporting contemporary data across the United States using updated definitions and limiting the inclusion criteria to patients with the highest risk of developing contrast-associated AKI (ie, patients with pre-existing moderate to severe renal impairment). Our data support using the contrast volume/eGFR ratio as a guide for contrast dosing and limiting the contrast volume to less than 3 times the eGFR. The observed high proportion of patients still receiving high contrast volume was surprising. Further studies should investigate the factors that explain persistent use of high contrast volume use during PCI.
Limitations
The results of this study should be interpreted in the context of certain limitations. First, it is an observational study limiting causal inference. Despite reporting adjusted ORs accounting for these differences, unmeasured confounders could still bias the results of the study. It is possible that physicians and institutions who follow low contrast dosing also follow other renal protective approaches, and the observed differences may be exaggerated in observation studies. However, in the absence of randomized trials, which are neither feasible nor ethical in this case, large observational studies such as this are the best option to study different levels of contrast dosing. Second, 23.6% of the patients undergoing PCI during the study period were excluded because of the lack of a pre-procedural creatinine and, hence, unknown baseline renal function. It is hard to speculate whether this has influenced the study results in a significant way. Third, the study population was limited to patients undergoing PCI, in which the contrast dosing would be higher than in non-invasive imaging or for patients undergoing diagnostic coronary angiography only, and thus cannot be generalized to those populations. Finally, outcome reporting is limited to in-hospital data. With increasingly early discharge after PCI, it is plausible that a significant number of patients were discharged prior to the peaking of creatinine, hence underestimating the occurrence of AKI.
Conclusions
This study shows the high prevalence of high contrast volume use during PCI for patients with moderate to severe renal impairment and provides additional support for the need and benefit of limiting the contrast volume to 3 times the eGFR during PCI.
Affiliations and Disclosures
Devika Aggarwal, MBBS1; Rebecca Young, MS2; Milan Seth, MS3; Daniel M. Wojdyla, MS2; Devraj Sukul, MD3; Tracy Y. Wang, MD4; Simon R. Dixon, MB, ChB5; Michael R. Rudnick, MD6; Shweta Bansal, MBBS7; Carlo Briguori, MD8; Hitinder S. Gurm, MBBS3
From 1Mount Sinai Fuster Heart, Mount Sinai Morningside Hospital, New York, New York; 2Duke Clinical Research Institute, Durham, North Carolina; 3University of Michigan, Ann Arbor, Michigan; 4Duke University Medical Center, Durham, North Carolina; 5William Beaumont University Hospital, Royal Oak, Michigan; 6Perelman School of Medicine of the University of Pennsylvania, Philadelphia, Pennsylvania; 7University of Texas Health Science Center at San Antonio, San Antonio, Texas; 8Mediterranea Cardiocentro, Naples, Italy.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Funding: The National Cardiovascular Data Registry (NCDR)-Cath PCI Registry (RPA-ID 683).
Address for correspondence: Hitinder S. Gurm, MBBS, 2A 192F, Frankel Cardiovascular Center, University of Michigan Health System, 1500 East Medical Center Dr., Ann Arbor, MI 48109, USA. Email: hgurm@med.umich.edu; X: @devikagg
References
1. Tsai TT, Patel UD, Chang TI, et al. Contemporary incidence, predictors, and outcomes of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the NCDR Cath-PCI registry. JACC Cardiovasc Interv. 2014;7(1):1-9. doi:10.1016/j.jcin.2013.06.016
2. Amin AP, McNeely C, Spertus JA, et al. Incremental cost of acute kidney injury after percutaneous coronary intervention in the United States. Am J Cardiol. 2020;125(1):29-33. doi:10.1016/j.amjcard.2019.09.042
3. Mehran R, Dangas GD, Weisbord SD. Contrast-associated acute kidney injury. N Engl J Med. 2019;380(22):2146-2155. doi:10.1056/NEJMra1805256
4. McCullough PA. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2008;51(15):1419-1428. doi:10.1016/j.jacc.2007.12.035
5. Almendarez M, Gurm HS, Mariani J Jr, et al. Procedural strategies to reduce the incidence of contrast-induced acute kidney injury during percutaneous coronary intervention. JACC Cardiovasc Interv. 2019;12(19):1877-1888. doi:10.1016/j.jcin.2019.04.055
6. Seeliger E, Sendeski M, Rihal CS, Persson PB. Contrast-induced kidney injury: mechanisms, risk factors, and prevention. Eur Heart J. 2012;33(16):2007-2015. doi:10.1093/eurheartj/ehr494
7. Gurm HS, Dixon SR, Smith DE, et al; BMC2 (Blue Cross Blue Shield of Michigan Cardiovascular Consortium) Registry. Renal function-based contrast dosing to define safe limits of radiographic contrast media in patients undergoing percutaneous coronary interventions. J Am Coll Cardiol. 2011;58(9):907-914. doi:10.1016/j.jacc.2011.05.023
8. Gurm HS, Seth M, Dixon S, Kraft P, Jensen A. Trends in contrast volume use and incidence of acute kidney injury in patients undergoing percutaneous coronary intervention: insights from Blue Cross Blue Shield of Michigan Cardiovascular Collaborative (BMC2). JACC Cardiovasc Interv. 2018;11(5):509-511. doi:10.1016/j.jcin.2017.10.018
9. Kooiman J, Seth M, Share D, Dixon S, Gurm HS. The association between contrast dose and renal complications post PCI across the continuum of procedural estimated risk. PLoS One. 2014;9(3):e90233. doi:10.1371/journal.pone.0090233
10. Brown JR, Solomon R, Stabler ME, et al. Team-based coaching intervention to improve contrast-associated acute kidney injury: a cluster-randomized trial. Clin J Am Soc Nephrol. 2023;18(3):315-326. doi:10.2215/CJN.0000000000000067
11. Kane GC, Doyle BJ, Lerman A, Barsness GW, Best PJ, Rihal CS. Ultra-low contrast volumes reduce rates of contrast-induced nephropathy in patients with chronic kidney disease undergoing coronary angiography. J Am Coll Cardiol. 2008;51(1):89-90. doi:10.1016/j.jacc.2007.09.019
12. Gurm HS, Seth M, Dixon SR, et al. Contemporary use of and outcomes associated with ultra-low contrast volume in patients undergoing percutaneous coronary interventions. Catheter Cardiovasc Interv. 2019;93(2):222-230. doi:10.1002/ccd.27819
13. Oliveira MD, Caixeta A. Ultra-low contrast strategy for routine coronary procedures via distal transradial access: real-world experience with consecutive all-comers patients from the DISTRACTION registry. J Invasive Cardiol. 2025;37(4). doi:10.25270/jic/24.00276
14. Moussa I, Hermann A, Messenger JC, et al. The NCDR CathPCI registry: a US national perspective on care and outcomes for percutaneous coronary intervention. Heart. 2013;99(5):297-303. doi:10.1136/heartjnl-2012-303379
15. Messenger JC, Ho KKL, Young CH, et al; NCDR Science and Quality Oversight Committee Data Quality Workgroup. The National Cardiovascular Data Registry (NCDR) Data Quality Brief: the NCDR Data Quality Program in 2012. J Am Coll Cardiol. 2012;60(16):1484-1488. doi:10.1016/j.jacc.2012.07.020
16. Delgado C, Baweja M, Crews DC, et al. A unifying approach for GFR estimation: recommendations of the NKF-ASN task force on reassessing the inclusion of race in diagnosing kidney disease. Am J Kidney Dis. 2022;79(2):268-288.e1. doi:10.1053/j.ajkd.2021.08.003
17. Mehta RL, Kellum JA, Shah SV, et al; Acute Kidney Injury Network. Acute Kidney Injury Network: report of an initiative to improve outcomes in acute kidney injury. Crit Care. 2007;11(2):R31. doi:10.1186/cc5713
18. Khwaja A. KDIGO clinical practice guidelines for acute kidney injury. Nephron Clin Pract. 2012;120(4):c179-c184. doi:10.1159/000339789
19. Tsai TT, Patel UD, Chang TI, et al. Validated contemporary risk model of acute kidney injury in patients undergoing percutaneous coronary interventions: insights from the National Cardiovascular Data Registry Cath-PCI registry. J Am Heart Assoc. 2014;3(6):e001380. doi:10.1161/JAHA.114.001380
20. Azzalini L, Vilca LM, Lombardo F, et al. Incidence of contrast-induced acute kidney injury in a large cohort of all-comers undergoing percutaneous coronary intervention: comparison of five contrast media. Int J Cardiol. 2018;273:69-73. doi:10.1016/j.ijcard.2018.08.097
21. Laskey WK, Jenkins C, Selzer F, et al. Volume-to-creatinine clearance ratio: a pharmacokinetically based risk factor for prediction of early creatinine increase after percutaneous coronary intervention. J Am Coll Cardiol. 2007;50(7):584-590. doi:10.1016/j.jacc.2007.03.058
22. Woltemath AA, Gonzalez G, Tecson KM, Vasquez J. Contrast-associated acute kidney injury following peripheral angiography. Proc (Bayl Univ Med Cent). 2021;34(6):678-680. doi:10.1080/08998280.2021.1941701
23. Gualano SK, Seth M, Gurm HS, et al. Renal function-based contrast threshold predicts kidney injury in transcatheter aortic valve replacement. J Soc Cardiovasc Angiogr Interv. 2022;1(3):100038. doi:10.1016/j.jscai.2022.100038











