The patient was a 71-year-old female nursing home resident with a past medical history remarkable for end-stage renal disease on hemodialysis, hypertension, diabetes mellitus and coronary artery disease. She also had a remote history of breast carcinoma and anemia, the latter resulting in a few bone marrow biopsies without any conclusive evidence regarding an underlying hematologic dyscrasia.
Case Presentation
From January 22, 2013, to February 13, 2013, the patient was hospitalized for respiratory insufficiency requiring intubation and pressor support. Approximately 1 month later on March 17, 2013, the patient developed difficulty swallowing and breathing although the shortness of breath was more due to upper airway abnormalities, according to the patient. She found it difficult to swallow solids with the symptoms of odynophagia becoming progressively worse over the ensuing days. She also complained of generalized weakness, fatigue and lightheadedness when standing. Over the past 2 days prior to admission to the hospital, she had a decreased appetite. Almost concurrent with the sore throat was the onset of a very distinctive skin rash that she described as otherwise asymptomatic.
At the time of admission, the patient was evaluated by an ear, nose and throat specialist in the emergency room; a flexible laryngoscopy demonstrated ulcerations involving the epiglottis, aryepiglottic folds and arytenoids. She also had a skin biopsy. Endoscopy of the esophagus and stomach showed intraoral ulcerations along with a small ulcerative nodule involving the gastroesophageal junction. The patient was placed in the intensive care unit and intubated due to difficulty breathing associated with laryngeal edema and ulcerations. The patient had been on various long-term medications including hydralazine (3/100 mg tablets per day) for treatment of hypertension.
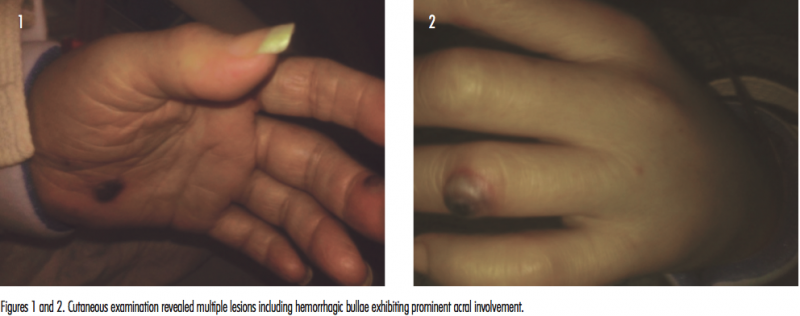
On physical examination, the patient showed left eyelid swelling with conjunctival injection in the lateral aspect. There were ulcerations of the lips and mucous membranes; the rest of the oral mucosa could not be visualized. Cutaneous examination revealed multiple lesions including hemorrhagic bullae scattered on the upper and lower extremities as well as palms and plantar surfaces of the foot and forehead (Figures 1 and 2).
Laboratory studies revealed a white blood cell count of 6.3, hemoglobin of 9.7, hematocrit of 28.6 and platelet count of 218. Blood cultures were negative. Viral serologies were also negative. A repeat bone marrow biopsy showed an increase in erythropoiesis and decreased granulopoiesis, whereby a low-grade myelodysplastic syndrome could not be excluded. The patient had a positive antineutrophilic cytoplasmic antibody (ANCA) assay showing a characteristic perinuclear staining pattern, while enzyme-linked immunosorbent assay studies demonstrated markedly elevated antibodies to myeloperoxidase (MPO). The patient was suspected of having a primary ANCA positive vasculitic syndrome such as microscopic polyarteritis. Skin and esophageal biopsies were performed to better elucidate the nature of the vasculitic process.
Pathology
Skin
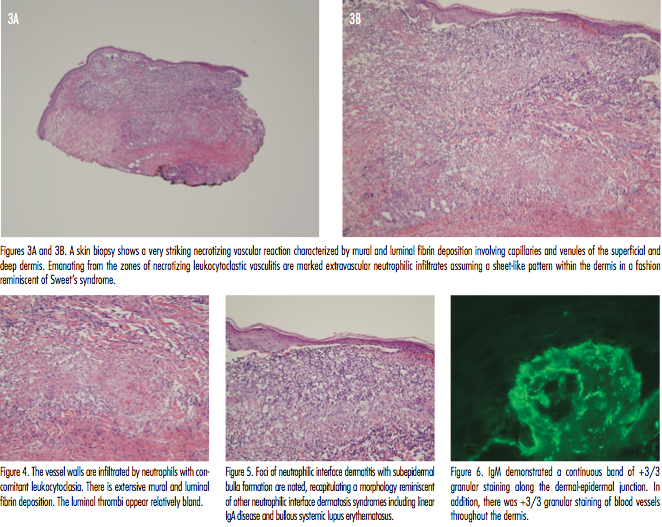
A skin biopsy was performed, demonstrating a very striking necrotizing vascular reaction characterized by mural and luminal fibrin deposition involving capillaries and venules of the superficial and deep dermis (Figures 3A and B). The vessel walls were infiltrated by neutrophils with concomitant leukocytoclasia (Figure 4). Vessels in the mid-dermis were occluded by acellular fibrin thrombi. Emanating from the zones of necrotizing leukocytoclastic vasculitis were marked extravascular neutrophilic infiltrates assuming a sheet-like pattern within the dermis albeit without frank dermolysis (Figures 3 and 4). Foci of neutrophilic interface dermatitis with subepidermal bulla formation were observed (Figure 5). While neutrophils were present along the dermal-epidermal junction, frank intraepidermal pustulation was not discernible. Special stains to evaluate for microbial pathogens were negative.
Direct immunofluorescent studies were obtained showing +3/3 granular staining of blood vessels throughout the dermis for IgM, C5-9 and C3 compatible with a microvascular injury syndrome (Figure 6).
Esophagus
An esophageal nodule showed a morphology that essentially mirrored that noted in the skin biopsy of a necrotizing leukocytoclastic vasculitis with accompanying extravascular neutrophilia.
Discussion
This is a case of a patient who developed a very distinctive vasculitic syndromic complex associated with positive ANCAs in the setting of long-term ingestion of the drug hydralazine. The patient was an older female who was on hydralazine in excess of 250 mg a day for several years before developing a distinctive cutaneous and extracutaneous vasculitis. The cutaneous lesions differed from classic palpable purpura due to their bullous hemorrhagic nodular quality in concert with their acral localization, resulting in a clinical morphologic semblance to a septic embolic event. In addition, also unusual in the realm of cutaneous vasculitis including drug-induced vasculitis, was the involvement of the oral cavity with extension to include the esophagus as well as lesions affecting the epiglottis and aryepiglottic fold bilaterally. Overall, the findings were consistent with hydralazine-induced ANCA positive vasculitis based on the similarity of this case to other cases reported in the literature. As with many other drug-induced autoimmune syndromic complexes, often the implicated drug has been ingested for a long period of time before the patient develops autoimmune sequelae.
The first reported series of hydralazine-associated vasculitis described 2 patients who developed a necrotizing leukocytoclastic vasculitis associated with high doses of hydralazine over several years, whereby in both cases cessation of the drug eventually led to resolution of their vasculitic syndrome.1 One of the 2 patients had lesions localized to the dorsum of the feet similar to our patient. Since that first paper, other anecdotal case reports have been published.2-7 The patients are typically older females who have been on higher doses of the drugs for years. The hemorrhagic blistering nature of the eruption with lower extremity involvement is also characteristic.7
The most recent reported case manifests a striking similarity to our case. In particular, Keasberry and colleagues8 described a patient with bullous hemorrhagic features involving the dorsum of the feet accompanied by night sweats, lethargy and weight loss in the setting of hydralazine therapy for 3 years prior to her presentation. Investigations revealed a high antinuclear antibody, antidouble stranded DNA antibody and anti-MPO antibody. As with our patient, the rash was bullous and hemorrhagic in quality. She also had a concomitant sore throat, mouth ulcers and otalgia.8
A characteristic feature of our case and potentially 1 other reported case is involvement of the epiglottis and aryepiglottic folds. Weiser et al described ulcerative lesions involving the epiglottis and arytenoepiglottic folds in the setting of hydralazine used for 6 months.9 The epiglottic lesion had a pseudotumorous morphology very similar to the esophageal lesions identified in our patient.
In the early 1990s, it became apparent that the hydralazine induced a lupus-like syndrome. Hydralazine-associated vasculitis was also associated with very specific antibodies, including lactoferrin and ANCAs. In 1994, Nasberger et al10 reported that anti-lactoferrin antibodies of IgG and IgM isotype were identified in 5% and 10% of systemic lupus erythematosus patients, respectively, while all patients with hydralazine-induced systemic lupus erythematosus had antibodies of both isotypes with a rapid decrement in the antibody levels following drug withdrawal. In this regard, the researchers suggested that anti-lactoferrin antibodies were clearly able to discriminate between hydralazine-induced systemic lupus erythematosus and true endogenous lupus erythematosus.10 According to Cambridge and colleagues, the presence of ANCAs was very distinctive for drug-induced lupus like reactions.3 They showed that patients with endogenous lupus did not have high titers of anti-MPO antibodies but invariably contained antinuclear antibodies, while anti-MPO antibodies of IgG and IgM isotype were observed in patients with both drug-induced nephritis as well as drug-induced systemic lupus erythematosus. The exact pathogenetic basis by which hydralazine evokes antibodies to MPO remains hypothetical.
There may be several different mechanisms by which drugs induce autoantibody formation. Neutrophil mediated metabolism of drugs may occur. Procainamide and hydralazine are both metabolized by MPO released from activated neutrophils to form reactive intermediate compounds. Such metabolites may be directly cytotoxic, leading to cell death and abnormal degradation of chromatin, whereby in a susceptible individual an autoimmune response directed against histone DNA complexes may occur. Alternatively, the reactive metabolites may act as a hapten for MPO and result in anti-MPO antibody formation.3 In the report by Short and Lockwood, the authors felt that the combined pattern of antibodies to MPO and lactoferrin were very characteristic and almost diagnostic of hydralazine-induced vasculitis.11 Hydralazine and procainamide have been shown to inhibit T cell DNA methylase, leading to a reduced amount of 5-methylcytosine in the genome and to induce autoreactivity in cloned CD4 positive T cells. This decrease in T cell DNA methylation may provide a link between drug therapy and autoreactivity.
Conclusion
Hydralazine-associated ANCA positive vasculitis is a very distinctive syndromic complex characterized by bullous hemorrhagic lesions with a predilection to involve the dorsal surfaces of the feet, often with a distinctive pattern of upper aerodigestive and intraoral ulceration with a tendency to involve the larynx.
Dr. Magro is the director of dermatopathology at the Weill Cornell Medical College in Manhattan, NY, and is board certified in anatomic pathology, dermatopathology and cytopathology.
Disclosure: The author reports no relevant financial relationships.
References
1. Finlay AY, Statham B, Knight AG. Hydrallazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6277):1703-1704.
2. Bernstein RM, Eqerton-Vernon J, Webster J. Hydrallazine-induced cutaneous vasculitis. Br Med J. 1980;280(6208):156-157.
3. Cambridge G, Wallace H, Bernstein RM, Leaker B. Autoantibodies to myeloperoxidase in idiopathic and drug-induced systemic lupus erythematosus and vasculitis. Br J Rheumatol. 1994;33(2):109-114.
4. Norris JH, Leeds J, Jeffrey RF. P-ANCA positive renal vasculitis in association with renal cell carcinoma and prolonged hydralazine therapy. Ren Fail. 2003;25(2)311-314.
5. Peacock A, Weatherell D. Hydralazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6270):1121-1122.
6. Reynolds NJ, Wallington TB, Burton JL. Hydralazine predisposes to acute cutaneous vasculitis following urography with iopamidol. Br J Dermatol. 1993;129(1) 82-85.
7. Sangala N, Lee RW, Horsfield C, Goldsmith DJ. Combined ANCA-associated vasculitis and lupus syndrome following prolonged use of hydralazine: a timely reminder of an old foe. Int Urol Nephrol 2010;42(2):503-506.
8. Keasberry J, Frazier J, Isbel NM, Van Eps CL, Oliver K, Mudge DW. Hydralazine-induced anti-neutrophil cytoplasmic antibody-positive renal vasculitis presenting with a vasculitic syndrome, acute nephritis and a puzzling skin rash: a case report. J Med Case Rep. 2013;7:20.
9. Weiser GA, Farouhar FA, White WB. Hydralazine hoarseness. Anew appearance. Arch Intern Med .1984;144(11):2271-2272.
10. Nasberger L, Hultquist R, Sturfelt G. Occurrence of anti-lactoferrin antibodies in patients with systemic lupus erythematosus, hydralazine-induced lupus, and rheumatoid arthritis. Scand J Rheumatol. 1994;23(4):206-210.
11. Short AK, Lockwood CM. Antigen specificity in hydralazine associated ANCA positive systemic vasculitis. QJM. 1995;88(11):775-783.
The patient was a 71-year-old female nursing home resident with a past medical history remarkable for end-stage renal disease on hemodialysis, hypertension, diabetes mellitus and coronary artery disease. She also had a remote history of breast carcinoma and anemia, the latter resulting in a few bone marrow biopsies without any conclusive evidence regarding an underlying hematologic dyscrasia.
Case Presentation
From January 22, 2013, to February 13, 2013, the patient was hospitalized for respiratory insufficiency requiring intubation and pressor support. Approximately 1 month later on March 17, 2013, the patient developed difficulty swallowing and breathing although the shortness of breath was more due to upper airway abnormalities, according to the patient. She found it difficult to swallow solids with the symptoms of odynophagia becoming progressively worse over the ensuing days. She also complained of generalized weakness, fatigue and lightheadedness when standing. Over the past 2 days prior to admission to the hospital, she had a decreased appetite. Almost concurrent with the sore throat was the onset of a very distinctive skin rash that she described as otherwise asymptomatic.
At the time of admission, the patient was evaluated by an ear, nose and throat specialist in the emergency room; a flexible laryngoscopy demonstrated ulcerations involving the epiglottis, aryepiglottic folds and arytenoids. She also had a skin biopsy. Endoscopy of the esophagus and stomach showed intraoral ulcerations along with a small ulcerative nodule involving the gastroesophageal junction. The patient was placed in the intensive care unit and intubated due to difficulty breathing associated with laryngeal edema and ulcerations. The patient had been on various long-term medications including hydralazine (3/100 mg tablets per day) for treatment of hypertension.
On physical examination, the patient showed left eyelid swelling with conjunctival injection in the lateral aspect. There were ulcerations of the lips and mucous membranes; the rest of the oral mucosa could not be visualized. Cutaneous examination revealed multiple lesions including hemorrhagic bullae scattered on the upper and lower extremities as well as palms and plantar surfaces of the foot and forehead (Figures 1 and 2).
Laboratory studies revealed a white blood cell count of 6.3, hemoglobin of 9.7, hematocrit of 28.6 and platelet count of 218. Blood cultures were negative. Viral serologies were also negative. A repeat bone marrow biopsy showed an increase in erythropoiesis and decreased granulopoiesis, whereby a low-grade myelodysplastic syndrome could not be excluded. The patient had a positive antineutrophilic cytoplasmic antibody (ANCA) assay showing a characteristic perinuclear staining pattern, while enzyme-linked immunosorbent assay studies demonstrated markedly elevated antibodies to myeloperoxidase (MPO). The patient was suspected of having a primary ANCA positive vasculitic syndrome such as microscopic polyarteritis. Skin and esophageal biopsies were performed to better elucidate the nature of the vasculitic process.


Pathology
Skin
A skin biopsy was performed, demonstrating a very striking necrotizing vascular reaction characterized by mural and luminal fibrin deposition involving capillaries and venules of the superficial and deep dermis (Figures 3A and B). The vessel walls were infiltrated by neutrophils with concomitant leukocytoclasia (Figure 4). Vessels in the mid-dermis were occluded by acellular fibrin thrombi. Emanating from the zones of necrotizing leukocytoclastic vasculitis were marked extravascular neutrophilic infiltrates assuming a sheet-like pattern within the dermis albeit without frank dermolysis (Figures 3 and 4). Foci of neutrophilic interface dermatitis with subepidermal bulla formation were observed (Figure 5). While neutrophils were present along the dermal-epidermal junction, frank intraepidermal pustulation was not discernible. Special stains to evaluate for microbial pathogens were negative.
Direct immunofluorescent studies were obtained showing +3/3 granular staining of blood vessels throughout the dermis for IgM, C5-9 and C3 compatible with a microvascular injury syndrome (Figure 6).
Esophagus
An esophageal nodule showed a morphology that essentially mirrored that noted in the skin biopsy of a necrotizing leukocytoclastic vasculitis with accompanying extravascular neutrophilia.
Discussion
This is a case of a patient who developed a very distinctive vasculitic syndromic complex associated with positive ANCAs in the setting of long-term ingestion of the drug hydralazine. The patient was an older female who was on hydralazine in excess of 250 mg a day for several years before developing a distinctive cutaneous and extracutaneous vasculitis. The cutaneous lesions differed from classic palpable purpura due to their bullous hemorrhagic nodular quality in concert with their acral localization, resulting in a clinical morphologic semblance to a septic embolic event. In addition, also unusual in the realm of cutaneous vasculitis including drug-induced vasculitis, was the involvement of the oral cavity with extension to include the esophagus as well as lesions affecting the epiglottis and aryepiglottic fold bilaterally. Overall, the findings were consistent with hydralazine-induced ANCA positive vasculitis based on the similarity of this case to other cases reported in the literature. As with many other drug-induced autoimmune syndromic complexes, often the implicated drug has been ingested for a long period of time before the patient develops autoimmune sequelae.
The first reported series of hydralazine-associated vasculitis described 2 patients who developed a necrotizing leukocytoclastic vasculitis associated with high doses of hydralazine over several years, whereby in both cases cessation of the drug eventually led to resolution of their vasculitic syndrome.1 One of the 2 patients had lesions localized to the dorsum of the feet similar to our patient. Since that first paper, other anecdotal case reports have been published.2-7 The patients are typically older females who have been on higher doses of the drugs for years. The hemorrhagic blistering nature of the eruption with lower extremity involvement is also characteristic.7
The most recent reported case manifests a striking similarity to our case. In particular, Keasberry and colleagues8 described a patient with bullous hemorrhagic features involving the dorsum of the feet accompanied by night sweats, lethargy and weight loss in the setting of hydralazine therapy for 3 years prior to her presentation. Investigations revealed a high antinuclear antibody, antidouble stranded DNA antibody and anti-MPO antibody. As with our patient, the rash was bullous and hemorrhagic in quality. She also had a concomitant sore throat, mouth ulcers and otalgia.8
A characteristic feature of our case and potentially 1 other reported case is involvement of the epiglottis and aryepiglottic folds. Weiser et al described ulcerative lesions involving the epiglottis and arytenoepiglottic folds in the setting of hydralazine used for 6 months.9 The epiglottic lesion had a pseudotumorous morphology very similar to the esophageal lesions identified in our patient.
In the early 1990s, it became apparent that the hydralazine induced a lupus-like syndrome. Hydralazine-associated vasculitis was also associated with very specific antibodies, including lactoferrin and ANCAs. In 1994, Nasberger et al10 reported that anti-lactoferrin antibodies of IgG and IgM isotype were identified in 5% and 10% of systemic lupus erythematosus patients, respectively, while all patients with hydralazine-induced systemic lupus erythematosus had antibodies of both isotypes with a rapid decrement in the antibody levels following drug withdrawal. In this regard, the researchers suggested that anti-lactoferrin antibodies were clearly able to discriminate between hydralazine-induced systemic lupus erythematosus and true endogenous lupus erythematosus.10 According to Cambridge and colleagues, the presence of ANCAs was very distinctive for drug-induced lupus like reactions.3 They showed that patients with endogenous lupus did not have high titers of anti-MPO antibodies but invariably contained antinuclear antibodies, while anti-MPO antibodies of IgG and IgM isotype were observed in patients with both drug-induced nephritis as well as drug-induced systemic lupus erythematosus. The exact pathogenetic basis by which hydralazine evokes antibodies to MPO remains hypothetical.
There may be several different mechanisms by which drugs induce autoantibody formation. Neutrophil mediated metabolism of drugs may occur. Procainamide and hydralazine are both metabolized by MPO released from activated neutrophils to form reactive intermediate compounds. Such metabolites may be directly cytotoxic, leading to cell death and abnormal degradation of chromatin, whereby in a susceptible individual an autoimmune response directed against histone DNA complexes may occur. Alternatively, the reactive metabolites may act as a hapten for MPO and result in anti-MPO antibody formation.3 In the report by Short and Lockwood, the authors felt that the combined pattern of antibodies to MPO and lactoferrin were very characteristic and almost diagnostic of hydralazine-induced vasculitis.11 Hydralazine and procainamide have been shown to inhibit T cell DNA methylase, leading to a reduced amount of 5-methylcytosine in the genome and to induce autoreactivity in cloned CD4 positive T cells. This decrease in T cell DNA methylation may provide a link between drug therapy and autoreactivity.
Conclusion
Hydralazine-associated ANCA positive vasculitis is a very distinctive syndromic complex characterized by bullous hemorrhagic lesions with a predilection to involve the dorsal surfaces of the feet, often with a distinctive pattern of upper aerodigestive and intraoral ulceration with a tendency to involve the larynx.
Dr. Magro is the director of dermatopathology at the Weill Cornell Medical College in Manhattan, NY, and is board certified in anatomic pathology, dermatopathology and cytopathology.
Disclosure: The author reports no relevant financial relationships.
References
1. Finlay AY, Statham B, Knight AG. Hydrallazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6277):1703-1704.
2. Bernstein RM, Eqerton-Vernon J, Webster J. Hydrallazine-induced cutaneous vasculitis. Br Med J. 1980;280(6208):156-157.
3. Cambridge G, Wallace H, Bernstein RM, Leaker B. Autoantibodies to myeloperoxidase in idiopathic and drug-induced systemic lupus erythematosus and vasculitis. Br J Rheumatol. 1994;33(2):109-114.
4. Norris JH, Leeds J, Jeffrey RF. P-ANCA positive renal vasculitis in association with renal cell carcinoma and prolonged hydralazine therapy. Ren Fail. 2003;25(2)311-314.
5. Peacock A, Weatherell D. Hydralazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6270):1121-1122.
6. Reynolds NJ, Wallington TB, Burton JL. Hydralazine predisposes to acute cutaneous vasculitis following urography with iopamidol. Br J Dermatol. 1993;129(1) 82-85.
7. Sangala N, Lee RW, Horsfield C, Goldsmith DJ. Combined ANCA-associated vasculitis and lupus syndrome following prolonged use of hydralazine: a timely reminder of an old foe. Int Urol Nephrol 2010;42(2):503-506.
8. Keasberry J, Frazier J, Isbel NM, Van Eps CL, Oliver K, Mudge DW. Hydralazine-induced anti-neutrophil cytoplasmic antibody-positive renal vasculitis presenting with a vasculitic syndrome, acute nephritis and a puzzling skin rash: a case report. J Med Case Rep. 2013;7:20.
9. Weiser GA, Farouhar FA, White WB. Hydralazine hoarseness. Anew appearance. Arch Intern Med .1984;144(11):2271-2272.
10. Nasberger L, Hultquist R, Sturfelt G. Occurrence of anti-lactoferrin antibodies in patients with systemic lupus erythematosus, hydralazine-induced lupus, and rheumatoid arthritis. Scand J Rheumatol. 1994;23(4):206-210.
11. Short AK, Lockwood CM. Antigen specificity in hydralazine associated ANCA positive systemic vasculitis. QJM. 1995;88(11):775-783.
The patient was a 71-year-old female nursing home resident with a past medical history remarkable for end-stage renal disease on hemodialysis, hypertension, diabetes mellitus and coronary artery disease. She also had a remote history of breast carcinoma and anemia, the latter resulting in a few bone marrow biopsies without any conclusive evidence regarding an underlying hematologic dyscrasia.
Case Presentation
From January 22, 2013, to February 13, 2013, the patient was hospitalized for respiratory insufficiency requiring intubation and pressor support. Approximately 1 month later on March 17, 2013, the patient developed difficulty swallowing and breathing although the shortness of breath was more due to upper airway abnormalities, according to the patient. She found it difficult to swallow solids with the symptoms of odynophagia becoming progressively worse over the ensuing days. She also complained of generalized weakness, fatigue and lightheadedness when standing. Over the past 2 days prior to admission to the hospital, she had a decreased appetite. Almost concurrent with the sore throat was the onset of a very distinctive skin rash that she described as otherwise asymptomatic.
At the time of admission, the patient was evaluated by an ear, nose and throat specialist in the emergency room; a flexible laryngoscopy demonstrated ulcerations involving the epiglottis, aryepiglottic folds and arytenoids. She also had a skin biopsy. Endoscopy of the esophagus and stomach showed intraoral ulcerations along with a small ulcerative nodule involving the gastroesophageal junction. The patient was placed in the intensive care unit and intubated due to difficulty breathing associated with laryngeal edema and ulcerations. The patient had been on various long-term medications including hydralazine (3/100 mg tablets per day) for treatment of hypertension.
On physical examination, the patient showed left eyelid swelling with conjunctival injection in the lateral aspect. There were ulcerations of the lips and mucous membranes; the rest of the oral mucosa could not be visualized. Cutaneous examination revealed multiple lesions including hemorrhagic bullae scattered on the upper and lower extremities as well as palms and plantar surfaces of the foot and forehead (Figures 1 and 2).
Laboratory studies revealed a white blood cell count of 6.3, hemoglobin of 9.7, hematocrit of 28.6 and platelet count of 218. Blood cultures were negative. Viral serologies were also negative. A repeat bone marrow biopsy showed an increase in erythropoiesis and decreased granulopoiesis, whereby a low-grade myelodysplastic syndrome could not be excluded. The patient had a positive antineutrophilic cytoplasmic antibody (ANCA) assay showing a characteristic perinuclear staining pattern, while enzyme-linked immunosorbent assay studies demonstrated markedly elevated antibodies to myeloperoxidase (MPO). The patient was suspected of having a primary ANCA positive vasculitic syndrome such as microscopic polyarteritis. Skin and esophageal biopsies were performed to better elucidate the nature of the vasculitic process.
Pathology
Skin
A skin biopsy was performed, demonstrating a very striking necrotizing vascular reaction characterized by mural and luminal fibrin deposition involving capillaries and venules of the superficial and deep dermis (Figures 3A and B). The vessel walls were infiltrated by neutrophils with concomitant leukocytoclasia (Figure 4). Vessels in the mid-dermis were occluded by acellular fibrin thrombi. Emanating from the zones of necrotizing leukocytoclastic vasculitis were marked extravascular neutrophilic infiltrates assuming a sheet-like pattern within the dermis albeit without frank dermolysis (Figures 3 and 4). Foci of neutrophilic interface dermatitis with subepidermal bulla formation were observed (Figure 5). While neutrophils were present along the dermal-epidermal junction, frank intraepidermal pustulation was not discernible. Special stains to evaluate for microbial pathogens were negative.
Direct immunofluorescent studies were obtained showing +3/3 granular staining of blood vessels throughout the dermis for IgM, C5-9 and C3 compatible with a microvascular injury syndrome (Figure 6).
Esophagus
An esophageal nodule showed a morphology that essentially mirrored that noted in the skin biopsy of a necrotizing leukocytoclastic vasculitis with accompanying extravascular neutrophilia.
Discussion
This is a case of a patient who developed a very distinctive vasculitic syndromic complex associated with positive ANCAs in the setting of long-term ingestion of the drug hydralazine. The patient was an older female who was on hydralazine in excess of 250 mg a day for several years before developing a distinctive cutaneous and extracutaneous vasculitis. The cutaneous lesions differed from classic palpable purpura due to their bullous hemorrhagic nodular quality in concert with their acral localization, resulting in a clinical morphologic semblance to a septic embolic event. In addition, also unusual in the realm of cutaneous vasculitis including drug-induced vasculitis, was the involvement of the oral cavity with extension to include the esophagus as well as lesions affecting the epiglottis and aryepiglottic fold bilaterally. Overall, the findings were consistent with hydralazine-induced ANCA positive vasculitis based on the similarity of this case to other cases reported in the literature. As with many other drug-induced autoimmune syndromic complexes, often the implicated drug has been ingested for a long period of time before the patient develops autoimmune sequelae.
The first reported series of hydralazine-associated vasculitis described 2 patients who developed a necrotizing leukocytoclastic vasculitis associated with high doses of hydralazine over several years, whereby in both cases cessation of the drug eventually led to resolution of their vasculitic syndrome.1 One of the 2 patients had lesions localized to the dorsum of the feet similar to our patient. Since that first paper, other anecdotal case reports have been published.2-7 The patients are typically older females who have been on higher doses of the drugs for years. The hemorrhagic blistering nature of the eruption with lower extremity involvement is also characteristic.7
The most recent reported case manifests a striking similarity to our case. In particular, Keasberry and colleagues8 described a patient with bullous hemorrhagic features involving the dorsum of the feet accompanied by night sweats, lethargy and weight loss in the setting of hydralazine therapy for 3 years prior to her presentation. Investigations revealed a high antinuclear antibody, antidouble stranded DNA antibody and anti-MPO antibody. As with our patient, the rash was bullous and hemorrhagic in quality. She also had a concomitant sore throat, mouth ulcers and otalgia.8
A characteristic feature of our case and potentially 1 other reported case is involvement of the epiglottis and aryepiglottic folds. Weiser et al described ulcerative lesions involving the epiglottis and arytenoepiglottic folds in the setting of hydralazine used for 6 months.9 The epiglottic lesion had a pseudotumorous morphology very similar to the esophageal lesions identified in our patient.
In the early 1990s, it became apparent that the hydralazine induced a lupus-like syndrome. Hydralazine-associated vasculitis was also associated with very specific antibodies, including lactoferrin and ANCAs. In 1994, Nasberger et al10 reported that anti-lactoferrin antibodies of IgG and IgM isotype were identified in 5% and 10% of systemic lupus erythematosus patients, respectively, while all patients with hydralazine-induced systemic lupus erythematosus had antibodies of both isotypes with a rapid decrement in the antibody levels following drug withdrawal. In this regard, the researchers suggested that anti-lactoferrin antibodies were clearly able to discriminate between hydralazine-induced systemic lupus erythematosus and true endogenous lupus erythematosus.10 According to Cambridge and colleagues, the presence of ANCAs was very distinctive for drug-induced lupus like reactions.3 They showed that patients with endogenous lupus did not have high titers of anti-MPO antibodies but invariably contained antinuclear antibodies, while anti-MPO antibodies of IgG and IgM isotype were observed in patients with both drug-induced nephritis as well as drug-induced systemic lupus erythematosus. The exact pathogenetic basis by which hydralazine evokes antibodies to MPO remains hypothetical.
There may be several different mechanisms by which drugs induce autoantibody formation. Neutrophil mediated metabolism of drugs may occur. Procainamide and hydralazine are both metabolized by MPO released from activated neutrophils to form reactive intermediate compounds. Such metabolites may be directly cytotoxic, leading to cell death and abnormal degradation of chromatin, whereby in a susceptible individual an autoimmune response directed against histone DNA complexes may occur. Alternatively, the reactive metabolites may act as a hapten for MPO and result in anti-MPO antibody formation.3 In the report by Short and Lockwood, the authors felt that the combined pattern of antibodies to MPO and lactoferrin were very characteristic and almost diagnostic of hydralazine-induced vasculitis.11 Hydralazine and procainamide have been shown to inhibit T cell DNA methylase, leading to a reduced amount of 5-methylcytosine in the genome and to induce autoreactivity in cloned CD4 positive T cells. This decrease in T cell DNA methylation may provide a link between drug therapy and autoreactivity.
Conclusion
Hydralazine-associated ANCA positive vasculitis is a very distinctive syndromic complex characterized by bullous hemorrhagic lesions with a predilection to involve the dorsal surfaces of the feet, often with a distinctive pattern of upper aerodigestive and intraoral ulceration with a tendency to involve the larynx.
Dr. Magro is the director of dermatopathology at the Weill Cornell Medical College in Manhattan, NY, and is board certified in anatomic pathology, dermatopathology and cytopathology.
Disclosure: The author reports no relevant financial relationships.
References
1. Finlay AY, Statham B, Knight AG. Hydrallazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6277):1703-1704.
2. Bernstein RM, Eqerton-Vernon J, Webster J. Hydrallazine-induced cutaneous vasculitis. Br Med J. 1980;280(6208):156-157.
3. Cambridge G, Wallace H, Bernstein RM, Leaker B. Autoantibodies to myeloperoxidase in idiopathic and drug-induced systemic lupus erythematosus and vasculitis. Br J Rheumatol. 1994;33(2):109-114.
4. Norris JH, Leeds J, Jeffrey RF. P-ANCA positive renal vasculitis in association with renal cell carcinoma and prolonged hydralazine therapy. Ren Fail. 2003;25(2)311-314.
5. Peacock A, Weatherell D. Hydralazine-induced necrotizing vasculitis. Br Med J (Clin Res Ed). 1981;282(6270):1121-1122.
6. Reynolds NJ, Wallington TB, Burton JL. Hydralazine predisposes to acute cutaneous vasculitis following urography with iopamidol. Br J Dermatol. 1993;129(1) 82-85.
7. Sangala N, Lee RW, Horsfield C, Goldsmith DJ. Combined ANCA-associated vasculitis and lupus syndrome following prolonged use of hydralazine: a timely reminder of an old foe. Int Urol Nephrol 2010;42(2):503-506.
8. Keasberry J, Frazier J, Isbel NM, Van Eps CL, Oliver K, Mudge DW. Hydralazine-induced anti-neutrophil cytoplasmic antibody-positive renal vasculitis presenting with a vasculitic syndrome, acute nephritis and a puzzling skin rash: a case report. J Med Case Rep. 2013;7:20.
9. Weiser GA, Farouhar FA, White WB. Hydralazine hoarseness. Anew appearance. Arch Intern Med .1984;144(11):2271-2272.
10. Nasberger L, Hultquist R, Sturfelt G. Occurrence of anti-lactoferrin antibodies in patients with systemic lupus erythematosus, hydralazine-induced lupus, and rheumatoid arthritis. Scand J Rheumatol. 1994;23(4):206-210.
11. Short AK, Lockwood CM. Antigen specificity in hydralazine associated ANCA positive systemic vasculitis. QJM. 1995;88(11):775-783.