 Biologic treatment has revolutionized the treatment of psoriasis and other inflammatory diseases. There are now multiple biologic options for patients, each with advantages and disadvantages. The purpose of this article is to describe how to select the right biologic for a patient who has not previously received biologic therapy. The article also discusses factors to consider when biologic treatment needs to be changed.
Biologic treatment has revolutionized the treatment of psoriasis and other inflammatory diseases. There are now multiple biologic options for patients, each with advantages and disadvantages. The purpose of this article is to describe how to select the right biologic for a patient who has not previously received biologic therapy. The article also discusses factors to consider when biologic treatment needs to be changed.
The main factors that affect the choice of biologic treatment include safety (such as short-term tolerability and long-term risk issues), efficacy (including the efficacy of the drug on the disease and on the comorbidities of the disease), cost of therapy, the convenience of the treatment, our general impressions of the drugs’ mechanism of action, or the story. (Table.)

Safety is often considered paramount, but safety may matter less than efficacy, cost and convenience. While efficacy differences between biologics are relatively easy to assess, safety differences are much more difficult. Cost is also surprisingly difficult to assess. Ultimately, patients should be informed of the advantages and disadvantages of the different options and be involved in the decision as to which biologic is best for them.
[Related: For more articles on Psoriasis visit the Psoriasis Medical Resource Center here.]
Safety
Safety is generally considered the single most important characteristic driving the choice of drug therapy. I would like to suggest that safety might not be nearly as important as we make it out to be. To attend the 2014 Interdisciplinary Autoimmune Summit (Figure 1), I had to make flight arrangements to Las Vegas. When making the airline reservations, my most important concern was making sure I got to where I wanted to go. I was also concerned about the cost and the convenience of the schedule. The tolerability of the flight (Coach or First Class) was also somewhat of a concern for me. Not once did I consider the safety of the airline in getting me to my destination. Federal Aviation Administration statistics on safety events vary considerably between airlines perhaps by as much as a factor of three.1 I paid no attention to those data nor did I even seek them out when making the plane reservations. Because all the airlines are safe, even a 3-fold difference in safety does not matter when we decide which airline to fly.
When we look at the biologics, we see they all have very good safety profiles, particularly in the population of patients with psoriasis; unlike patients with rheumatoid arthritis, psoriasis patients are not frequently taking other immunosuppressive agents such as prednisone and methotrexate. When looking at thousands of patients who were treated with adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), there was no statistically significant increased risk of serious adverse events, serious infections, malignancies or death.2

Figure 1. At the Interdisciplinary Autoimmune Summit, held in June 2014 in Las Vegas, experts and specialists from across the rheumatic autoimmune disease spectrum met to better understand how to treat and collaboratively care for patients with interrelated diseases.
A Cochran review of biologics safety found that there was a higher rate of total adverse events, withdrawal due to adverse events and risk of tuberculosis reactivation compared to control; but the rates of serious adverse events, serious infections, lymphoma and congestive heart failure were not statistically significantly different between biologics and placebo.3 Recently, the 5-year safety data for ustekinumab (Stelara; Janssen Biotech Inc.) has been reported revealing low rates of serious adverse events, serious infections, malignancies and no tendency for those risks to increase over the 5 years of treatment.4 Potentially there could be safety differences between the biologics, but it would take large head-to-head trials to show that there are meaningful differences. The fact that it takes such large trials suggests that the magnitude of the differences between these drugs is quite small. If the magnitude of the differences in risk is small, other factors such as efficacy, cost and convenience may be more important than safety in driving our decision-making process.
Efficacy
The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index (PASI 75) is used as the measure of success (Figure 2.). There are few head-to-head studies assessing PASI among biologics. Etanercept might be expected to give about a 50% PASI 75 rate, adalimumab and ustekinumab closer to 67% to 70%, while some of the newer biologics in development such as interleukin (IL)-17 inhibitors report PASI 75 rates of up to 80% or so.5-9
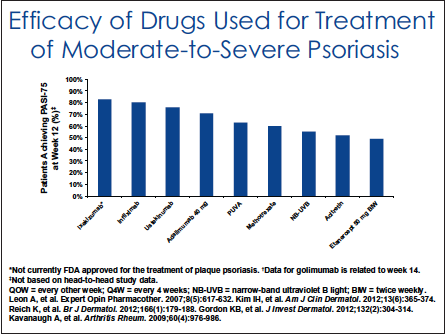
Figure 2. The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index is used as the measure of success.
Without head-to-head trial data, one cannot speak too confidently about the relative efficacy of the available agents, but it does appear that adalimumab and ustekinumab are a bit more potent than etanercept. Aside from the direct efficacy effects, the choice of biologics may be impacted by indirect efficacy effects on comorbidity, including improvements in psoriatic arthritis and cardiovascular comorbidities associated with psoriasis.10,11 Tumor necrosis factor (TNF) inhibitors have strong data for the prevention of joint destruction and overall benefit in psoriatic arthritis. Ustekinumab is now approved for psoriatic arthritis but does not have an indication for prevention of joint destruction. However, while untreated/undertreated psoriatic arthritis can cause permanent damage, 70% of patients with psoriasis do not develop psoriatic arthritis and therefore do not have progressive joint destruction. There is also accumulating evidence that the biologics reduce cardiovascular comorbidities. This may be reassuring to patients, as the reduction in cardiovascular risk may more than make up for any increased risk of a morbidity or mortality, infections or malignancies that might be associated with biologic treatment.
Cost
I used to feel that cost was an important driver in my choice of biologic because I like to be a good steward of healthcare resources. I have published extensively on the cost of biologic treatment. I have come to the conclusion that the cost to the insurer is not something that should weigh heavily in my decision-making because I really do not know what the cost is to the insurer. Because various insurers may contract for biologics at difference prices and because they do not tell me what those prices are, I cannot take those prices into consideration when deciding what therapy to give to a patient. Insurers have yet to tell me what to prescribe to a patient; however, they do tell me what they will pay for and that does have a major effect on the choice of a biologic for patients. Thus, I leave it to the insurer’s policies to address the cost-to-insurer issue.
While payer costs do not affect my decision-making process, patients’ costs do. The type of insurance they have, their copayments and the availability of copayment assistance are all factors that weigh heavily in the decision of what treatment to prescribe to the patient. That said, often copayments and support do not differ a lot between the biological treatments, and therefore cost plays less of a role than one might think when choosing a therapy.
Convenience and Tolerability
Convenience and tolerability of treatment makes a big impact on which biologic patients choose to take. Number and frequency of injections, the type of injections and the character and degree of pain associated with injection all affect the patient’s decision-making. Injection site reactions may also cause patients to prefer 1 treatment versus another. Some patients prefer treatments that require fewer injections, while other patients may prefer a drug that leaves their system quickly when they have to stop the drug therapy.
The Story
Mechanism of action does not play a significant role in the choice of therapy. The immune system is inscrutable; we have to rely on efficacy and safety data from trials, not mechanism of action, to know the benefit and risk of new drugs.
Nevertheless, knowing that TNF-related genes and IL-23 genes are associated with psoriasis may provide patients with some comfort about which biologics they want to take. Genetic defects in IL-23 are not lethal; patients with documented IL-23 deficiency may have susceptibility to unusual Salmonella infections.12 Because unusual Salmonella infections have not been observed in patients on ustekinumab, this may be comforting to some patients. IL-17 deficiency is associated with chronic mucocutaneous candidiasis; this may be more or less reassuring to patients (knowing that candidiasis is easily treated with a fluconazole pill).13
Helping Patients Decide
We are fortunate to have so many great options for our patients who have psoriasis. The choice of which biologic to take is a multidimensional problem.
Advantages and disadvantages are associated with each biologic treatment. Patients may be more or less concerned about different aspects of treatment. While I, as a doctor, may prefer 1 drug over another, my preferences may not match with patients’ preferences. Therefore, I think it is best to tell patients about their various options and let them choose.
Often they want to know my opinion. In those instances, I may tell them which drug I think is best, but again I leave the ultimate decision to the patient. This requires patients to be knowledgeable about the different treatment options and requires us to educate patients about the various reasonable treatment options. I rely heavily on resources from the National Psoriasis Foundation to accomplish this. The Foundation has fact sheets on the various biological treatments for psoriasis, as well as a terrific comparison chart so that patients can compare the difference treatment options.14,15
If a patient goes on a biologic and there is either insufficient efficacy or intolerable side effects or if they have to change drug therapy for other reasons (eg, cost of therapy), clinicians need to determine what treatments should be tried next. Ideally, we want to give patients the best balance of efficacy, safety and other considerations. In most cases if we have to switch from one biologic to another, (eg, because of their long half lives), we can just stop 1 drug and start the next without any issues. If a biologic from 1 class fails, it does not necessarily mean that another biologic of the same class would fail, but it certainly would not be unreasonable to try a biologic from another class in that situation.
Conclusion
When treating patients with psoriasis and other inflammatory diseases, clinicians should first consider that patients might not need a biologic. Phototherapy might still be a highly effective, safe and cost-effective option for patients. Second, there is no one best biologic for all patients. It is prudent to discuss all the reasonable options with patients. Finally, the resources available from the National Psoriasis Foundation may be one of the most efficient ways to present this information to patients and to educate them about the treatment options available.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol-Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
References
1. Feldman SR. Airline safety doesn’t matter. The Dermatologist. 2013;21(3):12. https://www.the-dermatologist.com/content/airline-safety-doesnt-matter. Accessed August 13, 2014.
2. Wiens A, Venson R, Correr CJ, Otuki MF, Pontarolo R. Meta-analysis of the efficacy and safety of adalimumab, etanercept, and infliximab for the treatment of rheumatoid arthritis. Pharmacotherapy. 2010;30(4):339-353.
3. Singh JA, Wells GA, Christensen R, et al. Adverse effects of biologics: a network meta-analysis and Cochrane overview. Cochrane Database Syst Rev. 2011;16(2):CD008794.
4. Papp KA, Griffiths CE, Gordon K, et al. Long-term safety of ustekinumab in patients with moderate-to-severe psoriasis: final results from 5 years of follow-up. Br J Dermatol. 2013;168(4):844-854.
5. Griffiths CE, Strober BE, van de Kerkhof P, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med. 2010;362(2):118-128.
6. Bansback N, Sizto S, Sun H, et al. Efficacy of systemic treatments for moderate to severe plaque psoriasis: systematic review and meta-analysis. Dermatology. 2009;219(3):209-218.
7. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366(13):1181-1189.
8. Papp KA, Langley RG, Sigurgeirsson B, et al. Efficacy and safety of secukinumab in the treatment of moderate-to-severe plaque psoriasis: a randomized, double-blind, placebo-controlled phase II dose-ranging study. Br J Dermatol. 2013;168(2):412-421.
9. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366(13):1190-1199.
10. Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5):851-864.
11. Boehncke WH, Boehncke S. Cardiovascular mortality in psoriasis and psoriatic arthritis: epidemiology, pathomechanisms, therapeutic implications, and perspectives. Curr Rheumatol Rep. 2012;14(4):343-348.
12. Torti DC, Felman SR. Interleukin-12, interleukin-23, and psoriasis: current prospects. J Am, Acad Dermatol. 2007;57(6):1059-1068.
13. Puel A, Cypowyj S, Maródi L, Abel L, Picard C, Casanova JL. Curr Opin Allergy Clin Immunol. 2012;12(6):616-622.
14. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed August 12, 2014.
15. National Psoriasis Foundation. Treatment Comparison for Psoriasis. https://www.psoriasis.org/publications/psoriasis-advance/2011/spring/treatment-comparison. Accessed August 12, 2014.
 Biologic treatment has revolutionized the treatment of psoriasis and other inflammatory diseases. There are now multiple biologic options for patients, each with advantages and disadvantages. The purpose of this article is to describe how to select the right biologic for a patient who has not previously received biologic therapy. The article also discusses factors to consider when biologic treatment needs to be changed.
Biologic treatment has revolutionized the treatment of psoriasis and other inflammatory diseases. There are now multiple biologic options for patients, each with advantages and disadvantages. The purpose of this article is to describe how to select the right biologic for a patient who has not previously received biologic therapy. The article also discusses factors to consider when biologic treatment needs to be changed.
The main factors that affect the choice of biologic treatment include safety (such as short-term tolerability and long-term risk issues), efficacy (including the efficacy of the drug on the disease and on the comorbidities of the disease), cost of therapy, the convenience of the treatment, our general impressions of the drugs’ mechanism of action, or the story. (Table.)

Safety is often considered paramount, but safety may matter less than efficacy, cost and convenience. While efficacy differences between biologics are relatively easy to assess, safety differences are much more difficult. Cost is also surprisingly difficult to assess. Ultimately, patients should be informed of the advantages and disadvantages of the different options and be involved in the decision as to which biologic is best for them.
[Related: For more articles on Psoriasis visit the Psoriasis Medical Resource Center here.]
Safety
Safety is generally considered the single most important characteristic driving the choice of drug therapy. I would like to suggest that safety might not be nearly as important as we make it out to be. To attend the 2014 Interdisciplinary Autoimmune Summit (Figure 1), I had to make flight arrangements to Las Vegas. When making the airline reservations, my most important concern was making sure I got to where I wanted to go. I was also concerned about the cost and the convenience of the schedule. The tolerability of the flight (Coach or First Class) was also somewhat of a concern for me. Not once did I consider the safety of the airline in getting me to my destination. Federal Aviation Administration statistics on safety events vary considerably between airlines perhaps by as much as a factor of three.1 I paid no attention to those data nor did I even seek them out when making the plane reservations. Because all the airlines are safe, even a 3-fold difference in safety does not matter when we decide which airline to fly.
When we look at the biologics, we see they all have very good safety profiles, particularly in the population of patients with psoriasis; unlike patients with rheumatoid arthritis, psoriasis patients are not frequently taking other immunosuppressive agents such as prednisone and methotrexate. When looking at thousands of patients who were treated with adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), there was no statistically significant increased risk of serious adverse events, serious infections, malignancies or death.2

Figure 1. At the Interdisciplinary Autoimmune Summit, held in June 2014 in Las Vegas, experts and specialists from across the rheumatic autoimmune disease spectrum met to better understand how to treat and collaboratively care for patients with interrelated diseases.
A Cochran review of biologics safety found that there was a higher rate of total adverse events, withdrawal due to adverse events and risk of tuberculosis reactivation compared to control; but the rates of serious adverse events, serious infections, lymphoma and congestive heart failure were not statistically significantly different between biologics and placebo.3 Recently, the 5-year safety data for ustekinumab (Stelara; Janssen Biotech Inc.) has been reported revealing low rates of serious adverse events, serious infections, malignancies and no tendency for those risks to increase over the 5 years of treatment.4 Potentially there could be safety differences between the biologics, but it would take large head-to-head trials to show that there are meaningful differences. The fact that it takes such large trials suggests that the magnitude of the differences between these drugs is quite small. If the magnitude of the differences in risk is small, other factors such as efficacy, cost and convenience may be more important than safety in driving our decision-making process.
Efficacy
The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index (PASI 75) is used as the measure of success (Figure 2.). There are few head-to-head studies assessing PASI among biologics. Etanercept might be expected to give about a 50% PASI 75 rate, adalimumab and ustekinumab closer to 67% to 70%, while some of the newer biologics in development such as interleukin (IL)-17 inhibitors report PASI 75 rates of up to 80% or so.5-9

Figure 2. The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index is used as the measure of success.
Without head-to-head trial data, one cannot speak too confidently about the relative efficacy of the available agents, but it does appear that adalimumab and ustekinumab are a bit more potent than etanercept. Aside from the direct efficacy effects, the choice of biologics may be impacted by indirect efficacy effects on comorbidity, including improvements in psoriatic arthritis and cardiovascular comorbidities associated with psoriasis.10,11 Tumor necrosis factor (TNF) inhibitors have strong data for the prevention of joint destruction and overall benefit in psoriatic arthritis. Ustekinumab is now approved for psoriatic arthritis but does not have an indication for prevention of joint destruction. However, while untreated/undertreated psoriatic arthritis can cause permanent damage, 70% of patients with psoriasis do not develop psoriatic arthritis and therefore do not have progressive joint destruction. There is also accumulating evidence that the biologics reduce cardiovascular comorbidities. This may be reassuring to patients, as the reduction in cardiovascular risk may more than make up for any increased risk of a morbidity or mortality, infections or malignancies that might be associated with biologic treatment.
Cost
I used to feel that cost was an important driver in my choice of biologic because I like to be a good steward of healthcare resources. I have published extensively on the cost of biologic treatment. I have come to the conclusion that the cost to the insurer is not something that should weigh heavily in my decision-making because I really do not know what the cost is to the insurer. Because various insurers may contract for biologics at difference prices and because they do not tell me what those prices are, I cannot take those prices into consideration when deciding what therapy to give to a patient. Insurers have yet to tell me what to prescribe to a patient; however, they do tell me what they will pay for and that does have a major effect on the choice of a biologic for patients. Thus, I leave it to the insurer’s policies to address the cost-to-insurer issue.
While payer costs do not affect my decision-making process, patients’ costs do. The type of insurance they have, their copayments and the availability of copayment assistance are all factors that weigh heavily in the decision of what treatment to prescribe to the patient. That said, often copayments and support do not differ a lot between the biological treatments, and therefore cost plays less of a role than one might think when choosing a therapy.
Convenience and Tolerability
Convenience and tolerability of treatment makes a big impact on which biologic patients choose to take. Number and frequency of injections, the type of injections and the character and degree of pain associated with injection all affect the patient’s decision-making. Injection site reactions may also cause patients to prefer 1 treatment versus another. Some patients prefer treatments that require fewer injections, while other patients may prefer a drug that leaves their system quickly when they have to stop the drug therapy.
The Story
Mechanism of action does not play a significant role in the choice of therapy. The immune system is inscrutable; we have to rely on efficacy and safety data from trials, not mechanism of action, to know the benefit and risk of new drugs.
Nevertheless, knowing that TNF-related genes and IL-23 genes are associated with psoriasis may provide patients with some comfort about which biologics they want to take. Genetic defects in IL-23 are not lethal; patients with documented IL-23 deficiency may have susceptibility to unusual Salmonella infections.12 Because unusual Salmonella infections have not been observed in patients on ustekinumab, this may be comforting to some patients. IL-17 deficiency is associated with chronic mucocutaneous candidiasis; this may be more or less reassuring to patients (knowing that candidiasis is easily treated with a fluconazole pill).13
Helping Patients Decide
We are fortunate to have so many great options for our patients who have psoriasis. The choice of which biologic to take is a multidimensional problem.
Advantages and disadvantages are associated with each biologic treatment. Patients may be more or less concerned about different aspects of treatment. While I, as a doctor, may prefer 1 drug over another, my preferences may not match with patients’ preferences. Therefore, I think it is best to tell patients about their various options and let them choose.
Often they want to know my opinion. In those instances, I may tell them which drug I think is best, but again I leave the ultimate decision to the patient. This requires patients to be knowledgeable about the different treatment options and requires us to educate patients about the various reasonable treatment options. I rely heavily on resources from the National Psoriasis Foundation to accomplish this. The Foundation has fact sheets on the various biological treatments for psoriasis, as well as a terrific comparison chart so that patients can compare the difference treatment options.14,15
If a patient goes on a biologic and there is either insufficient efficacy or intolerable side effects or if they have to change drug therapy for other reasons (eg, cost of therapy), clinicians need to determine what treatments should be tried next. Ideally, we want to give patients the best balance of efficacy, safety and other considerations. In most cases if we have to switch from one biologic to another, (eg, because of their long half lives), we can just stop 1 drug and start the next without any issues. If a biologic from 1 class fails, it does not necessarily mean that another biologic of the same class would fail, but it certainly would not be unreasonable to try a biologic from another class in that situation.
Conclusion
When treating patients with psoriasis and other inflammatory diseases, clinicians should first consider that patients might not need a biologic. Phototherapy might still be a highly effective, safe and cost-effective option for patients. Second, there is no one best biologic for all patients. It is prudent to discuss all the reasonable options with patients. Finally, the resources available from the National Psoriasis Foundation may be one of the most efficient ways to present this information to patients and to educate them about the treatment options available.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol-Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
References
1. Feldman SR. Airline safety doesn’t matter. The Dermatologist. 2013;21(3):12. https://www.the-dermatologist.com/content/airline-safety-doesnt-matter. Accessed August 13, 2014.
2. Wiens A, Venson R, Correr CJ, Otuki MF, Pontarolo R. Meta-analysis of the efficacy and safety of adalimumab, etanercept, and infliximab for the treatment of rheumatoid arthritis. Pharmacotherapy. 2010;30(4):339-353.
3. Singh JA, Wells GA, Christensen R, et al. Adverse effects of biologics: a network meta-analysis and Cochrane overview. Cochrane Database Syst Rev. 2011;16(2):CD008794.
4. Papp KA, Griffiths CE, Gordon K, et al. Long-term safety of ustekinumab in patients with moderate-to-severe psoriasis: final results from 5 years of follow-up. Br J Dermatol. 2013;168(4):844-854.
5. Griffiths CE, Strober BE, van de Kerkhof P, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med. 2010;362(2):118-128.
6. Bansback N, Sizto S, Sun H, et al. Efficacy of systemic treatments for moderate to severe plaque psoriasis: systematic review and meta-analysis. Dermatology. 2009;219(3):209-218.
7. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366(13):1181-1189.
8. Papp KA, Langley RG, Sigurgeirsson B, et al. Efficacy and safety of secukinumab in the treatment of moderate-to-severe plaque psoriasis: a randomized, double-blind, placebo-controlled phase II dose-ranging study. Br J Dermatol. 2013;168(2):412-421.
9. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366(13):1190-1199.
10. Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5):851-864.
11. Boehncke WH, Boehncke S. Cardiovascular mortality in psoriasis and psoriatic arthritis: epidemiology, pathomechanisms, therapeutic implications, and perspectives. Curr Rheumatol Rep. 2012;14(4):343-348.
12. Torti DC, Felman SR. Interleukin-12, interleukin-23, and psoriasis: current prospects. J Am, Acad Dermatol. 2007;57(6):1059-1068.
13. Puel A, Cypowyj S, Maródi L, Abel L, Picard C, Casanova JL. Curr Opin Allergy Clin Immunol. 2012;12(6):616-622.
14. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed August 12, 2014.
15. National Psoriasis Foundation. Treatment Comparison for Psoriasis. https://www.psoriasis.org/publications/psoriasis-advance/2011/spring/treatment-comparison. Accessed August 12, 2014.
Biologic treatment has revolutionized the treatment of psoriasis and other inflammatory diseases. There are now multiple biologic options for patients, each with advantages and disadvantages. The purpose of this article is to describe how to select the right biologic for a patient who has not previously received biologic therapy. The article also discusses factors to consider when biologic treatment needs to be changed.
The main factors that affect the choice of biologic treatment include safety (such as short-term tolerability and long-term risk issues), efficacy (including the efficacy of the drug on the disease and on the comorbidities of the disease), cost of therapy, the convenience of the treatment, our general impressions of the drugs’ mechanism of action, or the story. (Table.)
Safety is often considered paramount, but safety may matter less than efficacy, cost and convenience. While efficacy differences between biologics are relatively easy to assess, safety differences are much more difficult. Cost is also surprisingly difficult to assess. Ultimately, patients should be informed of the advantages and disadvantages of the different options and be involved in the decision as to which biologic is best for them.
[Related: For more articles on Psoriasis visit the Psoriasis Medical Resource Center here.]
Safety
Safety is generally considered the single most important characteristic driving the choice of drug therapy. I would like to suggest that safety might not be nearly as important as we make it out to be. To attend the 2014 Interdisciplinary Autoimmune Summit (Figure 1), I had to make flight arrangements to Las Vegas. When making the airline reservations, my most important concern was making sure I got to where I wanted to go. I was also concerned about the cost and the convenience of the schedule. The tolerability of the flight (Coach or First Class) was also somewhat of a concern for me. Not once did I consider the safety of the airline in getting me to my destination. Federal Aviation Administration statistics on safety events vary considerably between airlines perhaps by as much as a factor of three.1 I paid no attention to those data nor did I even seek them out when making the plane reservations. Because all the airlines are safe, even a 3-fold difference in safety does not matter when we decide which airline to fly.
When we look at the biologics, we see they all have very good safety profiles, particularly in the population of patients with psoriasis; unlike patients with rheumatoid arthritis, psoriasis patients are not frequently taking other immunosuppressive agents such as prednisone and methotrexate. When looking at thousands of patients who were treated with adalimumab (Humira, AbbVie Inc.), etanercept (Enbrel, Amgen Inc.) and infliximab (Remicade, Janssen Biotech Inc.), there was no statistically significant increased risk of serious adverse events, serious infections, malignancies or death.2
Figure 1. At the Interdisciplinary Autoimmune Summit, held in June 2014 in Las Vegas, experts and specialists from across the rheumatic autoimmune disease spectrum met to better understand how to treat and collaboratively care for patients with interrelated diseases.
A Cochran review of biologics safety found that there was a higher rate of total adverse events, withdrawal due to adverse events and risk of tuberculosis reactivation compared to control; but the rates of serious adverse events, serious infections, lymphoma and congestive heart failure were not statistically significantly different between biologics and placebo.3 Recently, the 5-year safety data for ustekinumab (Stelara; Janssen Biotech Inc.) has been reported revealing low rates of serious adverse events, serious infections, malignancies and no tendency for those risks to increase over the 5 years of treatment.4 Potentially there could be safety differences between the biologics, but it would take large head-to-head trials to show that there are meaningful differences. The fact that it takes such large trials suggests that the magnitude of the differences between these drugs is quite small. If the magnitude of the differences in risk is small, other factors such as efficacy, cost and convenience may be more important than safety in driving our decision-making process.
Efficacy
The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index (PASI 75) is used as the measure of success (Figure 2.). There are few head-to-head studies assessing PASI among biologics. Etanercept might be expected to give about a 50% PASI 75 rate, adalimumab and ustekinumab closer to 67% to 70%, while some of the newer biologics in development such as interleukin (IL)-17 inhibitors report PASI 75 rates of up to 80% or so.5-9
Figure 2. The efficacy of biologics is generally assessed by looking at the percentage of patients who achieve success within about 3 months of treatment. Usually a 75% improvement in Psoriasis Area and Severity Index is used as the measure of success.
Without head-to-head trial data, one cannot speak too confidently about the relative efficacy of the available agents, but it does appear that adalimumab and ustekinumab are a bit more potent than etanercept. Aside from the direct efficacy effects, the choice of biologics may be impacted by indirect efficacy effects on comorbidity, including improvements in psoriatic arthritis and cardiovascular comorbidities associated with psoriasis.10,11 Tumor necrosis factor (TNF) inhibitors have strong data for the prevention of joint destruction and overall benefit in psoriatic arthritis. Ustekinumab is now approved for psoriatic arthritis but does not have an indication for prevention of joint destruction. However, while untreated/undertreated psoriatic arthritis can cause permanent damage, 70% of patients with psoriasis do not develop psoriatic arthritis and therefore do not have progressive joint destruction. There is also accumulating evidence that the biologics reduce cardiovascular comorbidities. This may be reassuring to patients, as the reduction in cardiovascular risk may more than make up for any increased risk of a morbidity or mortality, infections or malignancies that might be associated with biologic treatment.
Cost
I used to feel that cost was an important driver in my choice of biologic because I like to be a good steward of healthcare resources. I have published extensively on the cost of biologic treatment. I have come to the conclusion that the cost to the insurer is not something that should weigh heavily in my decision-making because I really do not know what the cost is to the insurer. Because various insurers may contract for biologics at difference prices and because they do not tell me what those prices are, I cannot take those prices into consideration when deciding what therapy to give to a patient. Insurers have yet to tell me what to prescribe to a patient; however, they do tell me what they will pay for and that does have a major effect on the choice of a biologic for patients. Thus, I leave it to the insurer’s policies to address the cost-to-insurer issue.
While payer costs do not affect my decision-making process, patients’ costs do. The type of insurance they have, their copayments and the availability of copayment assistance are all factors that weigh heavily in the decision of what treatment to prescribe to the patient. That said, often copayments and support do not differ a lot between the biological treatments, and therefore cost plays less of a role than one might think when choosing a therapy.
Convenience and Tolerability
Convenience and tolerability of treatment makes a big impact on which biologic patients choose to take. Number and frequency of injections, the type of injections and the character and degree of pain associated with injection all affect the patient’s decision-making. Injection site reactions may also cause patients to prefer 1 treatment versus another. Some patients prefer treatments that require fewer injections, while other patients may prefer a drug that leaves their system quickly when they have to stop the drug therapy.
The Story
Mechanism of action does not play a significant role in the choice of therapy. The immune system is inscrutable; we have to rely on efficacy and safety data from trials, not mechanism of action, to know the benefit and risk of new drugs.
Nevertheless, knowing that TNF-related genes and IL-23 genes are associated with psoriasis may provide patients with some comfort about which biologics they want to take. Genetic defects in IL-23 are not lethal; patients with documented IL-23 deficiency may have susceptibility to unusual Salmonella infections.12 Because unusual Salmonella infections have not been observed in patients on ustekinumab, this may be comforting to some patients. IL-17 deficiency is associated with chronic mucocutaneous candidiasis; this may be more or less reassuring to patients (knowing that candidiasis is easily treated with a fluconazole pill).13
Helping Patients Decide
We are fortunate to have so many great options for our patients who have psoriasis. The choice of which biologic to take is a multidimensional problem.
Advantages and disadvantages are associated with each biologic treatment. Patients may be more or less concerned about different aspects of treatment. While I, as a doctor, may prefer 1 drug over another, my preferences may not match with patients’ preferences. Therefore, I think it is best to tell patients about their various options and let them choose.
Often they want to know my opinion. In those instances, I may tell them which drug I think is best, but again I leave the ultimate decision to the patient. This requires patients to be knowledgeable about the different treatment options and requires us to educate patients about the various reasonable treatment options. I rely heavily on resources from the National Psoriasis Foundation to accomplish this. The Foundation has fact sheets on the various biological treatments for psoriasis, as well as a terrific comparison chart so that patients can compare the difference treatment options.14,15
If a patient goes on a biologic and there is either insufficient efficacy or intolerable side effects or if they have to change drug therapy for other reasons (eg, cost of therapy), clinicians need to determine what treatments should be tried next. Ideally, we want to give patients the best balance of efficacy, safety and other considerations. In most cases if we have to switch from one biologic to another, (eg, because of their long half lives), we can just stop 1 drug and start the next without any issues. If a biologic from 1 class fails, it does not necessarily mean that another biologic of the same class would fail, but it certainly would not be unreasonable to try a biologic from another class in that situation.
Conclusion
When treating patients with psoriasis and other inflammatory diseases, clinicians should first consider that patients might not need a biologic. Phototherapy might still be a highly effective, safe and cost-effective option for patients. Second, there is no one best biologic for all patients. It is prudent to discuss all the reasonable options with patients. Finally, the resources available from the National Psoriasis Foundation may be one of the most efficient ways to present this information to patients and to educate them about the treatment options available.
Dr. Feldman is with the Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC.
Disclosure: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories, L.P. Dr. Feldman is a consultant and speaker for Galderma, Stiefel/GlaxoSmithKline, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec and Bristol-Myers Squibb. Dr. Feldman has received grants from Galderma, Astellas, Abbott Labs, Warner Chilcott, Janssen, Amgen, Photomedex, Genentech, BiogenIdec, Coria/Valeant, Pharmaderm, Ortho Pharmaceuticals, Aventis Pharmaceuticals, Roche Dermatology, 3M, Bristol-Myers Squibb, Stiefel/GlaxoSmithKline, Novartis, Medicis, Leo, HanAll Pharmaceuticals, Celgene, Basilea and Anacor and has received stock options from Photomedex. He is owner of www.DrScore.com and a founder of Causa Research.
References
1. Feldman SR. Airline safety doesn’t matter. The Dermatologist. 2013;21(3):12. https://www.the-dermatologist.com/content/airline-safety-doesnt-matter. Accessed August 13, 2014.
2. Wiens A, Venson R, Correr CJ, Otuki MF, Pontarolo R. Meta-analysis of the efficacy and safety of adalimumab, etanercept, and infliximab for the treatment of rheumatoid arthritis. Pharmacotherapy. 2010;30(4):339-353.
3. Singh JA, Wells GA, Christensen R, et al. Adverse effects of biologics: a network meta-analysis and Cochrane overview. Cochrane Database Syst Rev. 2011;16(2):CD008794.
4. Papp KA, Griffiths CE, Gordon K, et al. Long-term safety of ustekinumab in patients with moderate-to-severe psoriasis: final results from 5 years of follow-up. Br J Dermatol. 2013;168(4):844-854.
5. Griffiths CE, Strober BE, van de Kerkhof P, et al. Comparison of ustekinumab and etanercept for moderate-to-severe psoriasis. N Engl J Med. 2010;362(2):118-128.
6. Bansback N, Sizto S, Sun H, et al. Efficacy of systemic treatments for moderate to severe plaque psoriasis: systematic review and meta-analysis. Dermatology. 2009;219(3):209-218.
7. Papp KA, Leonardi C, Menter A, et al. Brodalumab, an anti-interleukin-17-receptor antibody for psoriasis. N Engl J Med. 2012;366(13):1181-1189.
8. Papp KA, Langley RG, Sigurgeirsson B, et al. Efficacy and safety of secukinumab in the treatment of moderate-to-severe plaque psoriasis: a randomized, double-blind, placebo-controlled phase II dose-ranging study. Br J Dermatol. 2013;168(2):412-421.
9. Leonardi C, Matheson R, Zachariae C, et al. Anti-interleukin-17 monoclonal antibody ixekizumab in chronic plaque psoriasis. N Engl J Med. 2012;366(13):1190-1199.
10. Gottlieb A, Korman NJ, Gordon KB, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 2. Psoriatic arthritis: overview and guidelines of care for treatment with an emphasis on the biologics. J Am Acad Dermatol. 2008;58(5):851-864.
11. Boehncke WH, Boehncke S. Cardiovascular mortality in psoriasis and psoriatic arthritis: epidemiology, pathomechanisms, therapeutic implications, and perspectives. Curr Rheumatol Rep. 2012;14(4):343-348.
12. Torti DC, Felman SR. Interleukin-12, interleukin-23, and psoriasis: current prospects. J Am, Acad Dermatol. 2007;57(6):1059-1068.
13. Puel A, Cypowyj S, Maródi L, Abel L, Picard C, Casanova JL. Curr Opin Allergy Clin Immunol. 2012;12(6):616-622.
14. National Psoriasis Foundations. Biologic Drugs: Fact Sheets. https://www.psoriasis.org/about-psoriasis/treatments/biologics/resources. Accessed August 12, 2014.
15. National Psoriasis Foundation. Treatment Comparison for Psoriasis. https://www.psoriasis.org/publications/psoriasis-advance/2011/spring/treatment-comparison. Accessed August 12, 2014.