In this ongoing series, we'll discuss what steps you need to take and what you need to know to add a successful subspecialty service to your practice.
 The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The role of other infectious diseases within dermatology, however, has remained strong. Many infectious diseases such as human papillomavirus, tinea, herpes, measles, varicella and impetigo have primary skin manifestations. Additionally, dermatologists have come to play a key role in the diagnosis and management of HIV as the epidemic has unfolded over the past 30 years. There are many academic dermatology departments that employ physicians who specialize in infectious diseases, actively serving, investigating and advancing this branch of dermatology. Trainees in the field who are inclined to the diagnostic challenge and treatable nature of infectious agents should strongly consider this subspecialty as a career choice.
Training and Human Capital Requirements
Neither the American Board of Dermatology (ABD) nor the Accreditation Council of Graduate Medical Education formally mandate the steps needed to specialize in infectious disease. The first step is to complete a dermatology residency as required by the ABD. During residency, trainees may request electives in their program or in other residency programs that enable them to work with mentors who focus in infectious disease. Patient populations for optimal learning include immigrants, which provides exposure to tropical diseases, transplant patients and the HIV population. A self-directed approach to teaching and exposure to a myriad of patients with infectious diseases is the best strategy, with particular attention to patients with refractory warts, herpes, sexually transmitted diseases and tropical diseases such as leishmaniasis and leprosy. Rotations at county hospitals or international rotations focusing on tropical diseases are particularly beneficial.
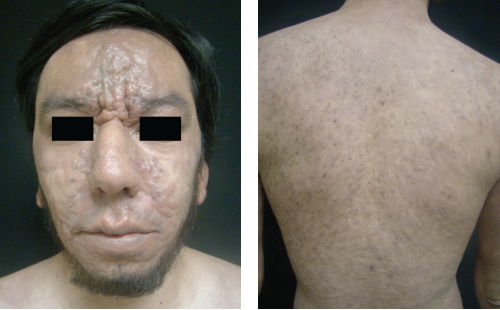
 Left: A patient with leprosy.
Left: A patient with leprosy.
Fellowships after residency provide additional training and are arranged by the individual by calling programs with faculty members who specialize in infectious diseases. For guidance and advice on such opportunities, finding mentors through your department chair or residency program director is recommended. In fellowships, trainees can conduct independent research on a breadth of topics or attend specialty clinics for a certain time period — usually 6 months to 1 year in length. A strong internal medicine background is also helpful for approaching and managing these conditions. Typically, an ID focus tends to be of greater interest for those leaning toward academic dermatology.
Regardless of whether the ID dermatologist is in academia or private practice, a well-trained ancillary staff is essential. With medical staff (such as nurses and medical assistants), administrative staff (such as billing and coding specialists), office managers and/or front desk staff, prior experience in dermatology or medicine is helpful. Prior experience facilitates the flow and productivity of the department, but no particular training other than the general education requirements for these positions is needed. With this training and staff, the dermatologist is ready to practice within the subspecialty of infectious disease.
Clinic Operations
As a subspecialty within dermatology, infectious disease is primarily an academic enterprise. It should be recognized, however, that few academic dermatologists — even those who have chosen the ID subspeciality — see only infectious disease patients, and most dermatologists in general private practice see infectious etiologies quite frequently. They can represent 20% of a private practitioner’s clientele, with the actual percentages depending on urban versus rural locale or the area of the country in which the clinic is located. Office visits with ID patients often lead to strong doctor-patient relationships, as complete discussions of outcomes are warranted. This often takes more time and, consequently, it can be difficult to see these patients in high-volume practice models. Also, the reimbursement for infectious disease visits may be lower than other dermatologic subspecialties.
 Left: A patient with leishmaniasis.
Left: A patient with leishmaniasis.
The satisfaction from this subspecialty comes from the challenge and opportunity to understand complex, unique disease processes and the associated clinical problem-solving. In the regular flow of an infectious disease clinic, there will be many visits for the common diseases mentioned earlier. Between these typical cases, however, patients will present with rare diseases that provide great learning opportunities and treatment predicaments. Additionally, biologic organisms are constantly evolving, leading to new paradigms in disease presentation, diagnosis and treatment. The academic setting further provides the opportunity to perform research that can greatly help your patients. This combination makes infectious disease an attractive and satisfying clinical experience.
Whether in the academic or private practice setting, the requirements to run an infectious disease clinic are fairly basic. The three major elements are: a lab where microbes can be cultured for diagnosis; a dermatopathology lab where special stains can be performed; and the equipment necessary for the removal and treatment of warts. Opening a lab to support an individual clinic is a somewhat challenging venture. There are many regulations, such as the Clinical Laboratory Improvement Amendments (CLIA) by the Centers for Medicare and Medicaid Services (CMS). The CLIA guidelines require multiple laboratory technicians, microscopes and other laboratory equipment, protective hoods, compliance and quality control programs and laboratory space of more than 10,000 sq ft — all at an expense of around $1 million — to satisfy requirements. Moreover, laboratory personnel must be CLIA certified before they can make final reports. The infectious disease subspecialist must then work with the lab in a local hospital or a regional laboratory to culture viruses, bacteria, fungi and acid-fast organisms.
The next requirement to run an infectious disease clinic is a good relationship with a trusted dermatopathologist. These specialists can often do the microbial cultures as well. If the physician is in an academic practice, they can usually send samples to the in-house dermatopathologist. It is important to remember that live tissue infections should not be sent to the lab or dermatopathologist and that formaldehyde inactivated samples are the norm. The dermatopathologist can perform special stains as needed depending on the clinical picture.
In terms of the special equipment used to treat warts, a smoke evacuator (typically less than $2,000), minor surgical equipment, hyfrecator for burning affected areas ($600 to $1,200) and lasers ($5,000 to $50,000) are needed.2 Additionally, a good working relationship with the hospital or local infectious disease specialist is very helpful. Overall, the needs for an infectious disease clinic are not particularly unique and can be easily integrated into a general dermatology practice.
Reimbursement Issues
In general, the area of infectious diseases does not have many reimbursement problems. Common codes are those for surgical destruction (17000 or 4600), KOH prep (87210) and punch and shave biopsy codes (11100). Sometimes negotiation with insurance companies is required when it comes to serology for herpes infections, as this modality is not standardized. However, typically, billing and coding is fairly straightforward.
Choosing the Area of Practice
The infectious disease subspecialty is intellectually stimulating and rewarding. It is much easier to concentrate solely on this area if you practice in the academic setting, but general dermatologists do see a significant number of infectious disease patients in their practices as well. The requirements for training of ancillary and administrative staff are similar to those of a general medical clinic. The office set up and equipment needs are minimal, but one must recognize the regulatory requirements. Reimbursement problems are uncommon. As a result, a person with a keen investigative mind and a liking of provocative skin findings will find the infectious disease subspecialty a true haven.
Drs. Venkat, West and Dabade are with the Center for Dermatology Research and Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Berger is with the Department of Dermatology, University of California – San Francisco School of Medicine in San Francisco, CA.
Disclosure: The Center for Dermatology Research is supported by an educational grant from Galderma Laboratories, L.P.
Drs. Venkat, West and Dabade have no disclosures.
Dr Berger is a consultant for Prescription Solutions and serves as a nonsalaried principal investigator in other research studies involving GlaxoSmithKline, Clinsys Clinical Research Inc, Merz Pharmaceuticals, and Pharmanet.
In this ongoing series, we'll discuss what steps you need to take and what you need to know to add a successful subspecialty service to your practice.
 The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The role of other infectious diseases within dermatology, however, has remained strong. Many infectious diseases such as human papillomavirus, tinea, herpes, measles, varicella and impetigo have primary skin manifestations. Additionally, dermatologists have come to play a key role in the diagnosis and management of HIV as the epidemic has unfolded over the past 30 years. There are many academic dermatology departments that employ physicians who specialize in infectious diseases, actively serving, investigating and advancing this branch of dermatology. Trainees in the field who are inclined to the diagnostic challenge and treatable nature of infectious agents should strongly consider this subspecialty as a career choice.
Training and Human Capital Requirements
Neither the American Board of Dermatology (ABD) nor the Accreditation Council of Graduate Medical Education formally mandate the steps needed to specialize in infectious disease. The first step is to complete a dermatology residency as required by the ABD. During residency, trainees may request electives in their program or in other residency programs that enable them to work with mentors who focus in infectious disease. Patient populations for optimal learning include immigrants, which provides exposure to tropical diseases, transplant patients and the HIV population. A self-directed approach to teaching and exposure to a myriad of patients with infectious diseases is the best strategy, with particular attention to patients with refractory warts, herpes, sexually transmitted diseases and tropical diseases such as leishmaniasis and leprosy. Rotations at county hospitals or international rotations focusing on tropical diseases are particularly beneficial.
 Left: A patient with leprosy.
Left: A patient with leprosy.
Fellowships after residency provide additional training and are arranged by the individual by calling programs with faculty members who specialize in infectious diseases. For guidance and advice on such opportunities, finding mentors through your department chair or residency program director is recommended. In fellowships, trainees can conduct independent research on a breadth of topics or attend specialty clinics for a certain time period — usually 6 months to 1 year in length. A strong internal medicine background is also helpful for approaching and managing these conditions. Typically, an ID focus tends to be of greater interest for those leaning toward academic dermatology.
Regardless of whether the ID dermatologist is in academia or private practice, a well-trained ancillary staff is essential. With medical staff (such as nurses and medical assistants), administrative staff (such as billing and coding specialists), office managers and/or front desk staff, prior experience in dermatology or medicine is helpful. Prior experience facilitates the flow and productivity of the department, but no particular training other than the general education requirements for these positions is needed. With this training and staff, the dermatologist is ready to practice within the subspecialty of infectious disease.
Clinic Operations
As a subspecialty within dermatology, infectious disease is primarily an academic enterprise. It should be recognized, however, that few academic dermatologists — even those who have chosen the ID subspeciality — see only infectious disease patients, and most dermatologists in general private practice see infectious etiologies quite frequently. They can represent 20% of a private practitioner’s clientele, with the actual percentages depending on urban versus rural locale or the area of the country in which the clinic is located. Office visits with ID patients often lead to strong doctor-patient relationships, as complete discussions of outcomes are warranted. This often takes more time and, consequently, it can be difficult to see these patients in high-volume practice models. Also, the reimbursement for infectious disease visits may be lower than other dermatologic subspecialties.
 Left: A patient with leishmaniasis.
Left: A patient with leishmaniasis.
The satisfaction from this subspecialty comes from the challenge and opportunity to understand complex, unique disease processes and the associated clinical problem-solving. In the regular flow of an infectious disease clinic, there will be many visits for the common diseases mentioned earlier. Between these typical cases, however, patients will present with rare diseases that provide great learning opportunities and treatment predicaments. Additionally, biologic organisms are constantly evolving, leading to new paradigms in disease presentation, diagnosis and treatment. The academic setting further provides the opportunity to perform research that can greatly help your patients. This combination makes infectious disease an attractive and satisfying clinical experience.
Whether in the academic or private practice setting, the requirements to run an infectious disease clinic are fairly basic. The three major elements are: a lab where microbes can be cultured for diagnosis; a dermatopathology lab where special stains can be performed; and the equipment necessary for the removal and treatment of warts. Opening a lab to support an individual clinic is a somewhat challenging venture. There are many regulations, such as the Clinical Laboratory Improvement Amendments (CLIA) by the Centers for Medicare and Medicaid Services (CMS). The CLIA guidelines require multiple laboratory technicians, microscopes and other laboratory equipment, protective hoods, compliance and quality control programs and laboratory space of more than 10,000 sq ft — all at an expense of around $1 million — to satisfy requirements. Moreover, laboratory personnel must be CLIA certified before they can make final reports. The infectious disease subspecialist must then work with the lab in a local hospital or a regional laboratory to culture viruses, bacteria, fungi and acid-fast organisms.
The next requirement to run an infectious disease clinic is a good relationship with a trusted dermatopathologist. These specialists can often do the microbial cultures as well. If the physician is in an academic practice, they can usually send samples to the in-house dermatopathologist. It is important to remember that live tissue infections should not be sent to the lab or dermatopathologist and that formaldehyde inactivated samples are the norm. The dermatopathologist can perform special stains as needed depending on the clinical picture.
In terms of the special equipment used to treat warts, a smoke evacuator (typically less than $2,000), minor surgical equipment, hyfrecator for burning affected areas ($600 to $1,200) and lasers ($5,000 to $50,000) are needed.2 Additionally, a good working relationship with the hospital or local infectious disease specialist is very helpful. Overall, the needs for an infectious disease clinic are not particularly unique and can be easily integrated into a general dermatology practice.
Reimbursement Issues
In general, the area of infectious diseases does not have many reimbursement problems. Common codes are those for surgical destruction (17000 or 4600), KOH prep (87210) and punch and shave biopsy codes (11100). Sometimes negotiation with insurance companies is required when it comes to serology for herpes infections, as this modality is not standardized. However, typically, billing and coding is fairly straightforward.
Choosing the Area of Practice
The infectious disease subspecialty is intellectually stimulating and rewarding. It is much easier to concentrate solely on this area if you practice in the academic setting, but general dermatologists do see a significant number of infectious disease patients in their practices as well. The requirements for training of ancillary and administrative staff are similar to those of a general medical clinic. The office set up and equipment needs are minimal, but one must recognize the regulatory requirements. Reimbursement problems are uncommon. As a result, a person with a keen investigative mind and a liking of provocative skin findings will find the infectious disease subspecialty a true haven.
Drs. Venkat, West and Dabade are with the Center for Dermatology Research and Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Berger is with the Department of Dermatology, University of California – San Francisco School of Medicine in San Francisco, CA.
Disclosure: The Center for Dermatology Research is supported by an educational grant from Galderma Laboratories, L.P.
Drs. Venkat, West and Dabade have no disclosures.
Dr Berger is a consultant for Prescription Solutions and serves as a nonsalaried principal investigator in other research studies involving GlaxoSmithKline, Clinsys Clinical Research Inc, Merz Pharmaceuticals, and Pharmanet.
In this ongoing series, we'll discuss what steps you need to take and what you need to know to add a successful subspecialty service to your practice.
The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The role of other infectious diseases within dermatology, however, has remained strong. Many infectious diseases such as human papillomavirus, tinea, herpes, measles, varicella and impetigo have primary skin manifestations. Additionally, dermatologists have come to play a key role in the diagnosis and management of HIV as the epidemic has unfolded over the past 30 years. There are many academic dermatology departments that employ physicians who specialize in infectious diseases, actively serving, investigating and advancing this branch of dermatology. Trainees in the field who are inclined to the diagnostic challenge and treatable nature of infectious agents should strongly consider this subspecialty as a career choice.
Training and Human Capital Requirements
Neither the American Board of Dermatology (ABD) nor the Accreditation Council of Graduate Medical Education formally mandate the steps needed to specialize in infectious disease. The first step is to complete a dermatology residency as required by the ABD. During residency, trainees may request electives in their program or in other residency programs that enable them to work with mentors who focus in infectious disease. Patient populations for optimal learning include immigrants, which provides exposure to tropical diseases, transplant patients and the HIV population. A self-directed approach to teaching and exposure to a myriad of patients with infectious diseases is the best strategy, with particular attention to patients with refractory warts, herpes, sexually transmitted diseases and tropical diseases such as leishmaniasis and leprosy. Rotations at county hospitals or international rotations focusing on tropical diseases are particularly beneficial.
Left: A patient with leprosy.
Fellowships after residency provide additional training and are arranged by the individual by calling programs with faculty members who specialize in infectious diseases. For guidance and advice on such opportunities, finding mentors through your department chair or residency program director is recommended. In fellowships, trainees can conduct independent research on a breadth of topics or attend specialty clinics for a certain time period — usually 6 months to 1 year in length. A strong internal medicine background is also helpful for approaching and managing these conditions. Typically, an ID focus tends to be of greater interest for those leaning toward academic dermatology.
Regardless of whether the ID dermatologist is in academia or private practice, a well-trained ancillary staff is essential. With medical staff (such as nurses and medical assistants), administrative staff (such as billing and coding specialists), office managers and/or front desk staff, prior experience in dermatology or medicine is helpful. Prior experience facilitates the flow and productivity of the department, but no particular training other than the general education requirements for these positions is needed. With this training and staff, the dermatologist is ready to practice within the subspecialty of infectious disease.
Clinic Operations
As a subspecialty within dermatology, infectious disease is primarily an academic enterprise. It should be recognized, however, that few academic dermatologists — even those who have chosen the ID subspeciality — see only infectious disease patients, and most dermatologists in general private practice see infectious etiologies quite frequently. They can represent 20% of a private practitioner’s clientele, with the actual percentages depending on urban versus rural locale or the area of the country in which the clinic is located. Office visits with ID patients often lead to strong doctor-patient relationships, as complete discussions of outcomes are warranted. This often takes more time and, consequently, it can be difficult to see these patients in high-volume practice models. Also, the reimbursement for infectious disease visits may be lower than other dermatologic subspecialties.
Left: A patient with leishmaniasis.
The satisfaction from this subspecialty comes from the challenge and opportunity to understand complex, unique disease processes and the associated clinical problem-solving. In the regular flow of an infectious disease clinic, there will be many visits for the common diseases mentioned earlier. Between these typical cases, however, patients will present with rare diseases that provide great learning opportunities and treatment predicaments. Additionally, biologic organisms are constantly evolving, leading to new paradigms in disease presentation, diagnosis and treatment. The academic setting further provides the opportunity to perform research that can greatly help your patients. This combination makes infectious disease an attractive and satisfying clinical experience.
Whether in the academic or private practice setting, the requirements to run an infectious disease clinic are fairly basic. The three major elements are: a lab where microbes can be cultured for diagnosis; a dermatopathology lab where special stains can be performed; and the equipment necessary for the removal and treatment of warts. Opening a lab to support an individual clinic is a somewhat challenging venture. There are many regulations, such as the Clinical Laboratory Improvement Amendments (CLIA) by the Centers for Medicare and Medicaid Services (CMS). The CLIA guidelines require multiple laboratory technicians, microscopes and other laboratory equipment, protective hoods, compliance and quality control programs and laboratory space of more than 10,000 sq ft — all at an expense of around $1 million — to satisfy requirements. Moreover, laboratory personnel must be CLIA certified before they can make final reports. The infectious disease subspecialist must then work with the lab in a local hospital or a regional laboratory to culture viruses, bacteria, fungi and acid-fast organisms.
The next requirement to run an infectious disease clinic is a good relationship with a trusted dermatopathologist. These specialists can often do the microbial cultures as well. If the physician is in an academic practice, they can usually send samples to the in-house dermatopathologist. It is important to remember that live tissue infections should not be sent to the lab or dermatopathologist and that formaldehyde inactivated samples are the norm. The dermatopathologist can perform special stains as needed depending on the clinical picture.
In terms of the special equipment used to treat warts, a smoke evacuator (typically less than $2,000), minor surgical equipment, hyfrecator for burning affected areas ($600 to $1,200) and lasers ($5,000 to $50,000) are needed.2 Additionally, a good working relationship with the hospital or local infectious disease specialist is very helpful. Overall, the needs for an infectious disease clinic are not particularly unique and can be easily integrated into a general dermatology practice.
Reimbursement Issues
In general, the area of infectious diseases does not have many reimbursement problems. Common codes are those for surgical destruction (17000 or 4600), KOH prep (87210) and punch and shave biopsy codes (11100). Sometimes negotiation with insurance companies is required when it comes to serology for herpes infections, as this modality is not standardized. However, typically, billing and coding is fairly straightforward.
Choosing the Area of Practice
The infectious disease subspecialty is intellectually stimulating and rewarding. It is much easier to concentrate solely on this area if you practice in the academic setting, but general dermatologists do see a significant number of infectious disease patients in their practices as well. The requirements for training of ancillary and administrative staff are similar to those of a general medical clinic. The office set up and equipment needs are minimal, but one must recognize the regulatory requirements. Reimbursement problems are uncommon. As a result, a person with a keen investigative mind and a liking of provocative skin findings will find the infectious disease subspecialty a true haven.
Drs. Venkat, West and Dabade are with the Center for Dermatology Research and Department of Dermatology at Wake Forest University School of Medicine in Winston-Salem, NC.
Dr. Berger is with the Department of Dermatology, University of California – San Francisco School of Medicine in San Francisco, CA.
Disclosure: The Center for Dermatology Research is supported by an educational grant from Galderma Laboratories, L.P.
Drs. Venkat, West and Dabade have no disclosures.
Dr Berger is a consultant for Prescription Solutions and serves as a nonsalaried principal investigator in other research studies involving GlaxoSmithKline, Clinsys Clinical Research Inc, Merz Pharmaceuticals, and Pharmanet.





 The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1
The area of infectious diseases (ID) has always played a significant role in dermatology. In 1932, the initial organization that was formed to maintain and elevate the standards in dermatology was called the American Board of Dermatology and Syphilology. It was only in 1955 that the name was changed to the American Board of Dermatology after the advent of penicillin greatly reduced the population of patients with syphilis.1 Left: A patient with leprosy.
Left: A patient with leprosy. Left: A patient with leishmaniasis.
Left: A patient with leishmaniasis.







