Among the most exciting developments in dermatology are new, non-surgical approaches to the treatment of both melanoma and non-melanoma skin cancer. In a series of articles published in The Dermatologist, approaches to the management of locally advanced and metastatic basal cell carcinoma (BCC) were discussed.1,2
The factors that define a given tumor as being locally advanced were discussed in the first article,1 and a treatment paradigm for advanced BCC was presented in the second.2 While surgery should always be viewed as the gold standard for treatment and will have the best chance for a durable cure, it is not always the optimal approach. Certain patient and/or tumor characteristics may limit the utility of surgical management. For instance, if surgery would result in loss of vital function such as vision or hearing, or if an elderly patient with multiple comorbidities would be at high risk for surgical complications, then non-surgical therapy may be preferred.
Clinical Decision-Making
With respect to advanced BCC, non-surgical approaches for advanced tumors include radiation therapy and oral hedgehog inhibitors (HHI). This article will focus on factors that may guide clinical decision-making when considering the use of HHI, how best to discuss their use and clinical course with patients and how to manage some of the more common side effects associated with their use.
HHI have been developed for the treatment of locally advanced and metastatic BCC. Vismodegib (Erivedge, Genentech, Inc.) is FDA approved and several other agents are in clinical trials nearing submission for approval. Vismodegib is used to treat adults with a BCC that has spread to other parts of the body or that has come back after surgery or that a healthcare provider decides cannot be treated with surgery or radiation. Efficacy of these agents has been established and reported previously.3
As with any new drug, questions and concerns arise regarding safety and real-world implementation. In order to successfully incorporate HHI into a practice, clinicians will need to feel comfortable with proper patient selection, as well as how to counsel patients and how to manage potential adverse events (AEs). Once the decision has been made to pursue non-surgical options for treatment, HHI can be an excellent choice for the appropriate patient.
Vismodegib is an oral capsule administered once daily. Dosing is standard at 150 mg and should not be altered. In this regard, it is a simpler medication to administer than many of the existing systemic agents used in dermatology, as it does not require any dosage calculation, no injections and no baseline or ongoing laboratory monitoring.
Safety and Tolerability
Product warnings are noted in the package insert for vismodegib4(Table 1). Among these is the warning that inhibition of the hedgehog pathway can have detrimental teratogenic effects on an unborn fetus. For this reason, when counseling women of childbearing age, it is critical to inform them of this risk and to verify pregnancy status prior to initiation of the drug. In women with a negative pregnancy test within 7 days prior to starting treatment, initiate a highly effective form (failure rate <1%) of contraception. This should be continued for 7 months after the last dose.
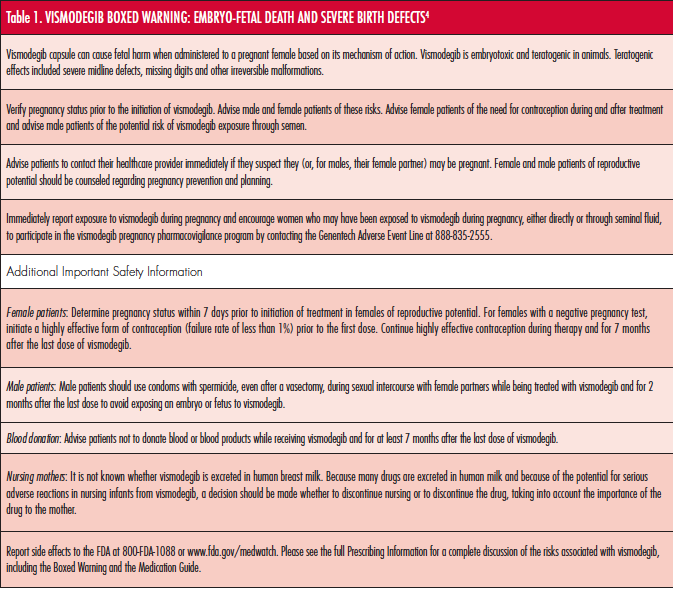
For male patients on HHI, there may be a risk of exposure of a fetus to the deleterious effects of the drug. Thus, they should use condoms with spermicide, even after vasectomy, during intercourse with female partners while being treated and for 2 months after their last dose. It is unknown whether HHI are excreted in human breast milk, thus a decision should be made whether to discontinue nursing or to discontinue the drug on a case-by-case basis. Other warnings advise patients not to donate blood while on vismodegib, and for at least 7 months after discontinuation.
Safety and tolerability are of major concern for both patient and provider with any treatment, particularly with new classes of treatment. Safety data collected from the pivotal Phase II trial, ERIVANCE,3 indicate very few serious AEs with vismodegib administration. With few exceptions, all reported AEs were grades 1 to 2 and only 1 patient experienced a grade 4 AE (fatigue). Certain AEs, however, are common, and knowledge of these ahead of time will help better prepare patients for what may come and to increase the likelihood of compliance through the duration of treatment.
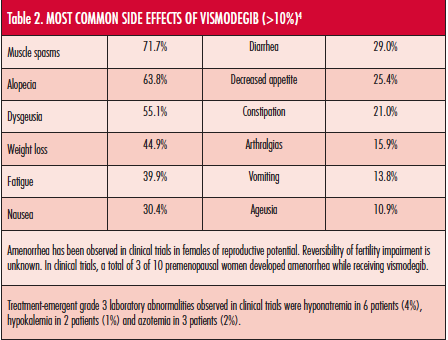
The most common AEs (>10%) associated with vismodegib are listed in Table 2 in order of decreasing frequency.4 All patients experienced at least 1 AE in the Phase II trial, but of the 104 patients in the trial, only 13 (12%) had an AE leading to discontinuation of the drug. Seven patients died during the study, however, no clear causative association with study the drug was identified.3
When counseling new patients, they will often ask how long they need to be on the medication. It is important to mention that different patients will experience different response rates to therapy, however, if they are going to experience a favorable response, then this can be apparent within a relatively short period of time. Often this visible and potentially profound shrinkage in tumor is excellent motivation for patients to continue treatment. For patients with conditions such as basal cell nevus syndrome or metastatic BCC, treatment should be continued until there is an intolerable AE or progression of disease while on drug.
As patients proceed with treatment, they will begin to experience some degree of AEs, and these may take several weeks to manifest. It is a good idea to clearly document tumor characteristics photographically from several angles or radiologically for metastatic disease. Careful measurements and tumor dimensions should also be recorded for each visit. No blood work is needed at routine follow-up visits. No established guidelines exist for timing of follow-up visits, however, when initiating any new systemic agent, close and frequent visits are helpful in identifying any potential AEs, helping patients stay motivated and assessing response to therapy.
No published reports exist with recommendations on how best to manage side effects. Anecdotal reports indicate that nausea can be managed with oral anti-emetics and muscle cramping can be tempered with low-dose muscle relaxants. Other AEs, such as alopecia and dysgeusia, will occur to different degrees, but by definition cannot have greater than grade 2 severity.
In the event of intolerable side effects, patients can be offered a break in treatment for several weeks and then resume the drug. This approach is particularly helpful in patients who experience an initial positive response to the drug but are discouraged by side effects. Other tips to consider for patients who are experiencing AEs to vismodegib are listed in Table 3.
Conclusion
Identification of the right patient for oral HHI can ensure the best chances for compliance and completing the course of treatment. Elderly patients who cannot tolerate surgery or radiation are often ideal candidates for HHI use. Locally advanced BCC in this group tend to be neglected tumors and can be deeply invasive and destructive. The elderly nursing home patient is often an ideal candidate for HHI therapy, as they are often unable to tolerate surgery. Families of these patients are often hesitant to treat skin cancers, however, duration of life expectancy is unpredictable. HHI offer an alternative to surgery and radiation and only requires a few office visits for the patient. HHI treatment should not be used in children or young patients who are still growing or developing. This may come in to play with patients that have certain genetic conditions such as basal cell nevus syndrome. Because of the teratogenic effects of vismodegib, it may have unknown consequences for growth and/or development.
As with the elderly, patients who have numerous medical comorbidities are often poor candidates for surgery or radiation and may tolerate HHI well. For reasons discussed earlier, women of childbearing age will require an additional level of counseling and close monitoring. Patients with genetic syndromes such as basal cell nevus syndrome can have an extremely high tumor burden, and HHI have proven to be life altering for this population. Lastly, prior to the approval of vismodegib, patients with metastatic BCC had no truly effective option for disease management, and HHI have been very beneficial in these cases.
BCC is a condition that dermatologists see more than any other medical specialty. The applications for HHI will continue to increase as we gain comfort and experience with their use. Although these drugs are not appropriate for every situation, proper patient selection, counseling and management of AEs are critical to ensure success.
Dr. Ibrahim is an assistant professor in dermatology, division of dermatologic surgery, Wilmot Cancer Center at University of Rochester in Rochester, NY.
Disclosure: Dr. Ibrahim is a consultant and speaker for Genentech
References
1. Ibrahim SF. Advanced basal cell carcinoma: Treatment overview. The Dermatologist. 2014;22(3)32-34.
2. Ibrahim SF. Practical use of vismodegib for advanced BCC. The Dermatologist. 2014;22(7)30-33.
3. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):2171-2179.
4. Erivedge [Product Insert], South San Francisco, CA: Genentech Inc; 2012.
5. American Society of Clinical Oncology. ASCO answers: Nausea and Vomiting. https://www.cancer.net/sites/cancer.net/files/asco_answers_nausea_vomiting.pdf. Accessed April 22, 2015.
6. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Nausea and Vomiting. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-common-side-effects-nausea-and-vomiting. Accessed April 22, 2015.
7. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Diarrhea. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-more-side-effects-diarrhea. Accessed April 22, 2015.
8. National Cancer Institute. Managing Chemotherapy Side Effects: Diarrhea. https://www.cancer.gov/cancertopcis/chemo-side-effects/diarrhea.pdf. Accessed April 22, 2015.
9. National Cancer Institute. Managing Chemotherapy Side Effects: Constipation. https://www.cancer.gov/publications/patient-education/constipation.pdf. Accessed April 22, 2015.
10. American Society of Clinical Oncology. ASCO answers: Cancer-Related Fatigue. https://www.cancer.net/sites/cancer.net/files/asco_answers_fatigue.pdf. Accessed April 22, 2015.
11. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Cancer-Related Fatigue. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive. Accessed April 22, 2015.
12. Cancercare. Coping with Cancer-Related Weight Changes and Muscle Loss. https://www.cancercare.org/publications/140-coping_with_cancer-related_weight_changes_and_muscle_loss. Accessed April 22, 2015.
13. American Society of Clinical Oncology. Appetite Loss. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/appetite-loss. Accessed April 22, 2015.
14. Wright A, Sluka KA. Nonpharmacological treatments for musculoskeletal pain. Clin J Pain. 2001;17(1):33-46.
15. Breastcancer.org. Muscle Pain (myalgia). https://www.breastcancer.org/treatment/side_effects/muscle_pain. Accessed April 22, 2015.
16. American Society of Clinical Oncology. Taste Changes. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/taste-changes. Accessed April 22, 2015.
17. American Society of Clinical Oncology. Hair Loss or Alopecia. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/hair-loss-or-alopecia. Accessed April 22, 2015.
18. Breastcancer.org. Bone and Joint Pain. https://www.breastcancer.org/treatment/side_effects/bone_joint_pain. Accessed April 22, 2015.
Among the most exciting developments in dermatology are new, non-surgical approaches to the treatment of both melanoma and non-melanoma skin cancer. In a series of articles published in The Dermatologist, approaches to the management of locally advanced and metastatic basal cell carcinoma (BCC) were discussed.1,2
The factors that define a given tumor as being locally advanced were discussed in the first article,1 and a treatment paradigm for advanced BCC was presented in the second.2 While surgery should always be viewed as the gold standard for treatment and will have the best chance for a durable cure, it is not always the optimal approach. Certain patient and/or tumor characteristics may limit the utility of surgical management. For instance, if surgery would result in loss of vital function such as vision or hearing, or if an elderly patient with multiple comorbidities would be at high risk for surgical complications, then non-surgical therapy may be preferred.
Clinical Decision-Making
With respect to advanced BCC, non-surgical approaches for advanced tumors include radiation therapy and oral hedgehog inhibitors (HHI). This article will focus on factors that may guide clinical decision-making when considering the use of HHI, how best to discuss their use and clinical course with patients and how to manage some of the more common side effects associated with their use.
HHI have been developed for the treatment of locally advanced and metastatic BCC. Vismodegib (Erivedge, Genentech, Inc.) is FDA approved and several other agents are in clinical trials nearing submission for approval. Vismodegib is used to treat adults with a BCC that has spread to other parts of the body or that has come back after surgery or that a healthcare provider decides cannot be treated with surgery or radiation. Efficacy of these agents has been established and reported previously.3
As with any new drug, questions and concerns arise regarding safety and real-world implementation. In order to successfully incorporate HHI into a practice, clinicians will need to feel comfortable with proper patient selection, as well as how to counsel patients and how to manage potential adverse events (AEs). Once the decision has been made to pursue non-surgical options for treatment, HHI can be an excellent choice for the appropriate patient.
Vismodegib is an oral capsule administered once daily. Dosing is standard at 150 mg and should not be altered. In this regard, it is a simpler medication to administer than many of the existing systemic agents used in dermatology, as it does not require any dosage calculation, no injections and no baseline or ongoing laboratory monitoring.
Safety and Tolerability
Product warnings are noted in the package insert for vismodegib4(Table 1). Among these is the warning that inhibition of the hedgehog pathway can have detrimental teratogenic effects on an unborn fetus. For this reason, when counseling women of childbearing age, it is critical to inform them of this risk and to verify pregnancy status prior to initiation of the drug. In women with a negative pregnancy test within 7 days prior to starting treatment, initiate a highly effective form (failure rate <1%) of contraception. This should be continued for 7 months after the last dose.

For male patients on HHI, there may be a risk of exposure of a fetus to the deleterious effects of the drug. Thus, they should use condoms with spermicide, even after vasectomy, during intercourse with female partners while being treated and for 2 months after their last dose. It is unknown whether HHI are excreted in human breast milk, thus a decision should be made whether to discontinue nursing or to discontinue the drug on a case-by-case basis. Other warnings advise patients not to donate blood while on vismodegib, and for at least 7 months after discontinuation.
Safety and tolerability are of major concern for both patient and provider with any treatment, particularly with new classes of treatment. Safety data collected from the pivotal Phase II trial, ERIVANCE,3 indicate very few serious AEs with vismodegib administration. With few exceptions, all reported AEs were grades 1 to 2 and only 1 patient experienced a grade 4 AE (fatigue). Certain AEs, however, are common, and knowledge of these ahead of time will help better prepare patients for what may come and to increase the likelihood of compliance through the duration of treatment.
The most common AEs (>10%) associated with vismodegib are listed in Table 2 in order of decreasing frequency.4 All patients experienced at least 1 AE in the Phase II trial, but of the 104 patients in the trial, only 13 (12%) had an AE leading to discontinuation of the drug. Seven patients died during the study, however, no clear causative association with study the drug was identified.3

When counseling new patients, they will often ask how long they need to be on the medication. It is important to mention that different patients will experience different response rates to therapy, however, if they are going to experience a favorable response, then this can be apparent within a relatively short period of time. Often this visible and potentially profound shrinkage in tumor is excellent motivation for patients to continue treatment. For patients with conditions such as basal cell nevus syndrome or metastatic BCC, treatment should be continued until there is an intolerable AE or progression of disease while on drug.
As patients proceed with treatment, they will begin to experience some degree of AEs, and these may take several weeks to manifest. It is a good idea to clearly document tumor characteristics photographically from several angles or radiologically for metastatic disease. Careful measurements and tumor dimensions should also be recorded for each visit. No blood work is needed at routine follow-up visits. No established guidelines exist for timing of follow-up visits, however, when initiating any new systemic agent, close and frequent visits are helpful in identifying any potential AEs, helping patients stay motivated and assessing response to therapy.
No published reports exist with recommendations on how best to manage side effects. Anecdotal reports indicate that nausea can be managed with oral anti-emetics and muscle cramping can be tempered with low-dose muscle relaxants. Other AEs, such as alopecia and dysgeusia, will occur to different degrees, but by definition cannot have greater than grade 2 severity.
In the event of intolerable side effects, patients can be offered a break in treatment for several weeks and then resume the drug. This approach is particularly helpful in patients who experience an initial positive response to the drug but are discouraged by side effects. Other tips to consider for patients who are experiencing AEs to vismodegib are listed in Table 3.
Conclusion
Identification of the right patient for oral HHI can ensure the best chances for compliance and completing the course of treatment. Elderly patients who cannot tolerate surgery or radiation are often ideal candidates for HHI use. Locally advanced BCC in this group tend to be neglected tumors and can be deeply invasive and destructive. The elderly nursing home patient is often an ideal candidate for HHI therapy, as they are often unable to tolerate surgery. Families of these patients are often hesitant to treat skin cancers, however, duration of life expectancy is unpredictable. HHI offer an alternative to surgery and radiation and only requires a few office visits for the patient. HHI treatment should not be used in children or young patients who are still growing or developing. This may come in to play with patients that have certain genetic conditions such as basal cell nevus syndrome. Because of the teratogenic effects of vismodegib, it may have unknown consequences for growth and/or development.
As with the elderly, patients who have numerous medical comorbidities are often poor candidates for surgery or radiation and may tolerate HHI well. For reasons discussed earlier, women of childbearing age will require an additional level of counseling and close monitoring. Patients with genetic syndromes such as basal cell nevus syndrome can have an extremely high tumor burden, and HHI have proven to be life altering for this population. Lastly, prior to the approval of vismodegib, patients with metastatic BCC had no truly effective option for disease management, and HHI have been very beneficial in these cases.
BCC is a condition that dermatologists see more than any other medical specialty. The applications for HHI will continue to increase as we gain comfort and experience with their use. Although these drugs are not appropriate for every situation, proper patient selection, counseling and management of AEs are critical to ensure success.
Dr. Ibrahim is an assistant professor in dermatology, division of dermatologic surgery, Wilmot Cancer Center at University of Rochester in Rochester, NY.
Disclosure: Dr. Ibrahim is a consultant and speaker for Genentech
References
1. Ibrahim SF. Advanced basal cell carcinoma: Treatment overview. The Dermatologist. 2014;22(3)32-34.
2. Ibrahim SF. Practical use of vismodegib for advanced BCC. The Dermatologist. 2014;22(7)30-33.
3. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):2171-2179.
4. Erivedge [Product Insert], South San Francisco, CA: Genentech Inc; 2012.
5. American Society of Clinical Oncology. ASCO answers: Nausea and Vomiting. https://www.cancer.net/sites/cancer.net/files/asco_answers_nausea_vomiting.pdf. Accessed April 22, 2015.
6. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Nausea and Vomiting. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-common-side-effects-nausea-and-vomiting. Accessed April 22, 2015.
7. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Diarrhea. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-more-side-effects-diarrhea. Accessed April 22, 2015.
8. National Cancer Institute. Managing Chemotherapy Side Effects: Diarrhea. https://www.cancer.gov/cancertopcis/chemo-side-effects/diarrhea.pdf. Accessed April 22, 2015.
9. National Cancer Institute. Managing Chemotherapy Side Effects: Constipation. https://www.cancer.gov/publications/patient-education/constipation.pdf. Accessed April 22, 2015.
10. American Society of Clinical Oncology. ASCO answers: Cancer-Related Fatigue. https://www.cancer.net/sites/cancer.net/files/asco_answers_fatigue.pdf. Accessed April 22, 2015.
11. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Cancer-Related Fatigue. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive. Accessed April 22, 2015.
12. Cancercare. Coping with Cancer-Related Weight Changes and Muscle Loss. https://www.cancercare.org/publications/140-coping_with_cancer-related_weight_changes_and_muscle_loss. Accessed April 22, 2015.
13. American Society of Clinical Oncology. Appetite Loss. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/appetite-loss. Accessed April 22, 2015.
14. Wright A, Sluka KA. Nonpharmacological treatments for musculoskeletal pain. Clin J Pain. 2001;17(1):33-46.
15. Breastcancer.org. Muscle Pain (myalgia). https://www.breastcancer.org/treatment/side_effects/muscle_pain. Accessed April 22, 2015.
16. American Society of Clinical Oncology. Taste Changes. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/taste-changes. Accessed April 22, 2015.
17. American Society of Clinical Oncology. Hair Loss or Alopecia. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/hair-loss-or-alopecia. Accessed April 22, 2015.
18. Breastcancer.org. Bone and Joint Pain. https://www.breastcancer.org/treatment/side_effects/bone_joint_pain. Accessed April 22, 2015.
Among the most exciting developments in dermatology are new, non-surgical approaches to the treatment of both melanoma and non-melanoma skin cancer. In a series of articles published in The Dermatologist, approaches to the management of locally advanced and metastatic basal cell carcinoma (BCC) were discussed.1,2
The factors that define a given tumor as being locally advanced were discussed in the first article,1 and a treatment paradigm for advanced BCC was presented in the second.2 While surgery should always be viewed as the gold standard for treatment and will have the best chance for a durable cure, it is not always the optimal approach. Certain patient and/or tumor characteristics may limit the utility of surgical management. For instance, if surgery would result in loss of vital function such as vision or hearing, or if an elderly patient with multiple comorbidities would be at high risk for surgical complications, then non-surgical therapy may be preferred.
Clinical Decision-Making
With respect to advanced BCC, non-surgical approaches for advanced tumors include radiation therapy and oral hedgehog inhibitors (HHI). This article will focus on factors that may guide clinical decision-making when considering the use of HHI, how best to discuss their use and clinical course with patients and how to manage some of the more common side effects associated with their use.
HHI have been developed for the treatment of locally advanced and metastatic BCC. Vismodegib (Erivedge, Genentech, Inc.) is FDA approved and several other agents are in clinical trials nearing submission for approval. Vismodegib is used to treat adults with a BCC that has spread to other parts of the body or that has come back after surgery or that a healthcare provider decides cannot be treated with surgery or radiation. Efficacy of these agents has been established and reported previously.3
As with any new drug, questions and concerns arise regarding safety and real-world implementation. In order to successfully incorporate HHI into a practice, clinicians will need to feel comfortable with proper patient selection, as well as how to counsel patients and how to manage potential adverse events (AEs). Once the decision has been made to pursue non-surgical options for treatment, HHI can be an excellent choice for the appropriate patient.
Vismodegib is an oral capsule administered once daily. Dosing is standard at 150 mg and should not be altered. In this regard, it is a simpler medication to administer than many of the existing systemic agents used in dermatology, as it does not require any dosage calculation, no injections and no baseline or ongoing laboratory monitoring.
Safety and Tolerability
Product warnings are noted in the package insert for vismodegib4(Table 1). Among these is the warning that inhibition of the hedgehog pathway can have detrimental teratogenic effects on an unborn fetus. For this reason, when counseling women of childbearing age, it is critical to inform them of this risk and to verify pregnancy status prior to initiation of the drug. In women with a negative pregnancy test within 7 days prior to starting treatment, initiate a highly effective form (failure rate <1%) of contraception. This should be continued for 7 months after the last dose.
For male patients on HHI, there may be a risk of exposure of a fetus to the deleterious effects of the drug. Thus, they should use condoms with spermicide, even after vasectomy, during intercourse with female partners while being treated and for 2 months after their last dose. It is unknown whether HHI are excreted in human breast milk, thus a decision should be made whether to discontinue nursing or to discontinue the drug on a case-by-case basis. Other warnings advise patients not to donate blood while on vismodegib, and for at least 7 months after discontinuation.
Safety and tolerability are of major concern for both patient and provider with any treatment, particularly with new classes of treatment. Safety data collected from the pivotal Phase II trial, ERIVANCE,3 indicate very few serious AEs with vismodegib administration. With few exceptions, all reported AEs were grades 1 to 2 and only 1 patient experienced a grade 4 AE (fatigue). Certain AEs, however, are common, and knowledge of these ahead of time will help better prepare patients for what may come and to increase the likelihood of compliance through the duration of treatment.
The most common AEs (>10%) associated with vismodegib are listed in Table 2 in order of decreasing frequency.4 All patients experienced at least 1 AE in the Phase II trial, but of the 104 patients in the trial, only 13 (12%) had an AE leading to discontinuation of the drug. Seven patients died during the study, however, no clear causative association with study the drug was identified.3
When counseling new patients, they will often ask how long they need to be on the medication. It is important to mention that different patients will experience different response rates to therapy, however, if they are going to experience a favorable response, then this can be apparent within a relatively short period of time. Often this visible and potentially profound shrinkage in tumor is excellent motivation for patients to continue treatment. For patients with conditions such as basal cell nevus syndrome or metastatic BCC, treatment should be continued until there is an intolerable AE or progression of disease while on drug.
As patients proceed with treatment, they will begin to experience some degree of AEs, and these may take several weeks to manifest. It is a good idea to clearly document tumor characteristics photographically from several angles or radiologically for metastatic disease. Careful measurements and tumor dimensions should also be recorded for each visit. No blood work is needed at routine follow-up visits. No established guidelines exist for timing of follow-up visits, however, when initiating any new systemic agent, close and frequent visits are helpful in identifying any potential AEs, helping patients stay motivated and assessing response to therapy.
No published reports exist with recommendations on how best to manage side effects. Anecdotal reports indicate that nausea can be managed with oral anti-emetics and muscle cramping can be tempered with low-dose muscle relaxants. Other AEs, such as alopecia and dysgeusia, will occur to different degrees, but by definition cannot have greater than grade 2 severity.
In the event of intolerable side effects, patients can be offered a break in treatment for several weeks and then resume the drug. This approach is particularly helpful in patients who experience an initial positive response to the drug but are discouraged by side effects. Other tips to consider for patients who are experiencing AEs to vismodegib are listed in Table 3.
Conclusion
Identification of the right patient for oral HHI can ensure the best chances for compliance and completing the course of treatment. Elderly patients who cannot tolerate surgery or radiation are often ideal candidates for HHI use. Locally advanced BCC in this group tend to be neglected tumors and can be deeply invasive and destructive. The elderly nursing home patient is often an ideal candidate for HHI therapy, as they are often unable to tolerate surgery. Families of these patients are often hesitant to treat skin cancers, however, duration of life expectancy is unpredictable. HHI offer an alternative to surgery and radiation and only requires a few office visits for the patient. HHI treatment should not be used in children or young patients who are still growing or developing. This may come in to play with patients that have certain genetic conditions such as basal cell nevus syndrome. Because of the teratogenic effects of vismodegib, it may have unknown consequences for growth and/or development.
As with the elderly, patients who have numerous medical comorbidities are often poor candidates for surgery or radiation and may tolerate HHI well. For reasons discussed earlier, women of childbearing age will require an additional level of counseling and close monitoring. Patients with genetic syndromes such as basal cell nevus syndrome can have an extremely high tumor burden, and HHI have proven to be life altering for this population. Lastly, prior to the approval of vismodegib, patients with metastatic BCC had no truly effective option for disease management, and HHI have been very beneficial in these cases.
BCC is a condition that dermatologists see more than any other medical specialty. The applications for HHI will continue to increase as we gain comfort and experience with their use. Although these drugs are not appropriate for every situation, proper patient selection, counseling and management of AEs are critical to ensure success.
Dr. Ibrahim is an assistant professor in dermatology, division of dermatologic surgery, Wilmot Cancer Center at University of Rochester in Rochester, NY.
Disclosure: Dr. Ibrahim is a consultant and speaker for Genentech
References
1. Ibrahim SF. Advanced basal cell carcinoma: Treatment overview. The Dermatologist. 2014;22(3)32-34.
2. Ibrahim SF. Practical use of vismodegib for advanced BCC. The Dermatologist. 2014;22(7)30-33.
3. Sekulic A, Migden MR, Oro AE, et al. Efficacy and safety of vismodegib in advanced basal-cell carcinoma. N Engl J Med. 2012;366(23):2171-2179.
4. Erivedge [Product Insert], South San Francisco, CA: Genentech Inc; 2012.
5. American Society of Clinical Oncology. ASCO answers: Nausea and Vomiting. https://www.cancer.net/sites/cancer.net/files/asco_answers_nausea_vomiting.pdf. Accessed April 22, 2015.
6. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Nausea and Vomiting. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-common-side-effects-nausea-and-vomiting. Accessed April 22, 2015.
7. American Cancer Society. Understanding Chemotherapy: A Guide for Patients and Families: Diarrhea. https://www.cancer.org/treatment/treatmentsandsideeffects/treatmenttypes/chemotherapy/understandingchemotherapyaguideforpatientsandfamilies/understanding-chemotherapy-more-side-effects-diarrhea. Accessed April 22, 2015.
8. National Cancer Institute. Managing Chemotherapy Side Effects: Diarrhea. https://www.cancer.gov/cancertopcis/chemo-side-effects/diarrhea.pdf. Accessed April 22, 2015.
9. National Cancer Institute. Managing Chemotherapy Side Effects: Constipation. https://www.cancer.gov/publications/patient-education/constipation.pdf. Accessed April 22, 2015.
10. American Society of Clinical Oncology. ASCO answers: Cancer-Related Fatigue. https://www.cancer.net/sites/cancer.net/files/asco_answers_fatigue.pdf. Accessed April 22, 2015.
11. National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology. Cancer-Related Fatigue. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#supportive. Accessed April 22, 2015.
12. Cancercare. Coping with Cancer-Related Weight Changes and Muscle Loss. https://www.cancercare.org/publications/140-coping_with_cancer-related_weight_changes_and_muscle_loss. Accessed April 22, 2015.
13. American Society of Clinical Oncology. Appetite Loss. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/appetite-loss. Accessed April 22, 2015.
14. Wright A, Sluka KA. Nonpharmacological treatments for musculoskeletal pain. Clin J Pain. 2001;17(1):33-46.
15. Breastcancer.org. Muscle Pain (myalgia). https://www.breastcancer.org/treatment/side_effects/muscle_pain. Accessed April 22, 2015.
16. American Society of Clinical Oncology. Taste Changes. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/taste-changes. Accessed April 22, 2015.
17. American Society of Clinical Oncology. Hair Loss or Alopecia. https://www.cancer.net/all-about-cancer/treating-cancer/managing-side-effects/hair-loss-or-alopecia. Accessed April 22, 2015.
18. Breastcancer.org. Bone and Joint Pain. https://www.breastcancer.org/treatment/side_effects/bone_joint_pain. Accessed April 22, 2015.














