It is estimated in the United States approximately 1 in 5 people will develop skin cancer in their lifetime leading to more patients visiting a dermatologist for routine skin exams.1 As most skin cancers are asymptomatic, most patients are unaware of these worrisome lesions. The most common forms of skin cancer are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) with melanoma accounting for 2% of skin cancer cases.2,3 Rarely, more unusual types of skin cancer are identified on routine skin exams.
Primary cutaneous lymphomas are a heterogeneous group of extranodal non-Hodgkin lymphomas. They are defined as “malignant lymphomas confined to the skin at presentation after complete staging procedures.”4 The majority of cutaneous lymphomas are T cell but approximately 25% of these are B-cell derived lymphomas.5 The B-cell derived cutaneous lymphomas are classified into several major entities by the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC) including primary cutaneous follicle-center lymphoma, primary cutaneous diffuse large B-cell lymphoma leg type, primary cutaneous marginal zone lymphoma (PCMZL, also known as extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue [MALT lymphoma]), primary cutaneous diffuse large B-cell lymphoma, other and intravascular diffuse large B-cell lymphoma.4
The incidence of cutaneous B-cell lymphoma has been increasing and is 3.1 per million persons, based on Surveillance, Epidemiology and End Results registry data.5 At presentation, most of the patients do not have extracutaneous signs and symptoms; therefore, most of the cutaneous lymphomas are diagnosed by dermatologists.6 With the increasing incidence, dermatologists must be on the lookout for cases of cutaneous B-cell lymphoma. This article presents a case of PCMZL that was diagnosed on routine skin exam.
Case Presentation
A 61-year-old female presented to the general dermatology clinic for a routine skin exam. The patient has a past medical history of hypertension and uterine fibroids. She has a personal history of BCC that was resected by Mohs micrographic surgery as well as a family history of colon and lung cancer. She denied fevers, chills, night sweats and weight loss and all other review of systems were negative. Patient had no knowledge of any new or changing skin lesions or moles. She had no lesions that were hurting, itching or bleeding. A complete skin exam was performed.
A small 3 mm erythematous papule was noted on the left upper arm. The patient had not noticed the lesion prior to the exam and did not know how long it had been there. No other similar lesions were noted on exam. Due to its unique appearance, the lesion was biopsied (Figure 1).

Figure 1. Post-biopsy photograph of the lesion showing small size and normal surrounding skin.
Histopathologic analysis revealed a dermal nodule comprised of sheets of plasma cells mixed with small lymphoid cells with irregular nuclear outlines (Figure 2). Several immunohistochemical stains were done. The lesion was positive for both lambda and kappa immunoglobulin light chains with kappa staining being stronger than lambda staining. Further immunologic analysis could not be done due to the small size of the specimen.
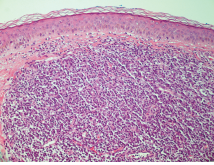
Figure 2. Hematoxylin and eosin stain of the lesion.
Despite this, the combination of findings favored cutaneous marginal zone (MALT) lymphoma with marked plasmacytic differentiation. Based on the clinicopathologic correlation, the patient was diagnosed with PCMZL. The pathologist suggested additional workup to rule out systemic lymphoma or plasma cell dyscrasia.
Discussion
PCMZL is believed to be the cutaneous counterpart of extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.7 With the new WHO-EORTC classification that came out in 2008, cases previously classified as primary cutaneous immunocytoma or primary cutaneous plasmacytoma were reclassified as PCMZL with prominent lymphoplasmacytic or plasmacytic differentiation respectively.4 Due to these changes, PCMZL is now one of the most common forms of primary cutaneous B-cell lymphoma.8
The etiology of PCMZL is unclear. Because the clinicopathologic features observed in the gastric mucosa-associated lymphoid tissue, (MALT) lymphomas are similar to the PCMZL, many believe there is a similar cause. MALT lymphomas have been linked to long-standing antigenic stimulation possibly due to chronic infection with Helicobacter pylori.9
Several studies show this same antigen-driven lymphomagenesis in the skin could be secondary to Borrelia burgdorferi infection.7,9 Some case reports from Europe show that some of PCMZL lesions contain B burgdorferi gene sequences on polymerase chain reaction.7,10 Very few of these cases have been found in the United States. Most people believe that the geographic variation is due to the different genospecies of Borrelia.7 No other microorganism has been convincingly linked to the development of PCMZL, and in the United States, the B burgdorferi connection has not been established.5 Therefore, no definitive cause PCMZL is identified in the United States.
The preponderance of patients with PCMZL are men over the age of 40.8 PCMZL can present with multiple phenotypes. The most common presentation is pink-violet to red-brown papules, plaques or nodules.6,7 The lesions are usually localized on the extremities or trunk and can be solitary or multiple.7 The differential diagnosis includes other skin cancers such as BCC, SCC, amelanotic melanoma, other cutaneous lymphomas and reactive lymphoid hyperplasias such as lymphomatoid papulosis. Unlike other forms of skin cancer, the lesions rarely ulcerate and are typically asymptomatic. Systemic signs or symptoms including fever, night sweats, weight loss and malaise are typically not present.6 The lack of B-cell symptoms is concordant with the fact that PCMZL is usually skin localized; however, systemic disease can be present and staging workup is necessary.7
Diagnosis
The diagnosis of PCMZL is made by biopsy with careful morphologic and immunohistochemical analysis. Histology of PCMZL on hematoxylin and eosin stain shows dense, lymphocytic infiltrate found mainly in the dermis and subcutaneous fat. Epidermotropism is not a feature of PCMZL and a grenz zone is commonly observed.7 Cytologically PCMZL is characterized by a polymorphous infiltrate that includes marginal zone cells, centrocyte-like cells, monocytoid cells and/or blastoid cells.8 Also, plasma cells, eosinophils and small lymphocytes can be found in the infiltrate.6 Germinal centers that are reactive but can contain malignant cells can be seen in about 70% of cases.7 Positive staining with CD20, CD79a and Bcl-2 can be seen in the centrocyte-like cells, but these cells are negative for CD5, CD10 and Bcl-6.6 As in our patient, monotypic expression of immunoglobulin light chains can be observed especially in cases expressing plasmacytoid differentitiation.7
The International Society for Cutaneous Lymphomas (ISCL) and EORTC recently proposed staging recommendations for cutaneous lymphomas.10 Workup should include a history, physical examination, laboratory studies including a lactate dehydrogenase (LDH) and imaging of the chest, abdomen and pelvis with either a computed tomography (CT) scan, positron emission tomography (PET) scan or combination PET/CT.3 The ISCL did not recommend bone marrow biopsy for the PCMZL.10 The International Extranodal Lymphoma Study Group identified 3 independent prognostic factors for PCMZL: elevated LDH, >2 skin lesions and nodular lesions.5 These factors make up the cutaneous lymphoma international prognostic index, which states that the absence of any adverse prognostic factor was associated with a 5-year progression-free survival (PFS) of 91%.5 The presence of 2 or 3 adverse prognostic factors was associated with a 5-year PFS of 48%.5 Most of the relapses seen are local relapses. Despite this, the overall 5-year disease specific survival is greater than 95% with PCMZL.5
Treatment
Patients with solitary lesions or a few grouped lesions of PCMZL can be treated by local radiotherapy, simple surgical excision or surgical excision followed by radiotherapy of the field.6,7
Radiation therapy is associated with a high response rate especially if associated with wide margin in the radiation field.5,6 One study showed complete remission after initial therapy was reached in 130 out of 132 patients.11 Systemic disease is more difficult to treat. Some advocate treating asymptomatic disease with observation.5 However, once patients with systemic disease have become symptomatic, corticosteroids, systemic interferon alfa, polychemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisone) and anti-CD20 monoclonal antibodies have been used with variable results.7 An initial trial of antibiotics due to the possible association of B burgdorferi has been recommended, but may not be useful for North American patients.5
Patient Outcome
Our patient was referred to a hematologist oncologist who did a staging workup. She received a CT scan as well as blood work including a complete metabolic panel, LDH level and a complete blood count with differential. The blood work was within normal limits and the CT scan did not show any evidence of other disease. The oncologist classified her as stage I skin limited PCMZL. Patient was referred to radiation oncology for local radiation therapy to the left arm.
Conclusion
The incidence of skin cancer continues to rise in the United States, and many patients are presenting to the dermatologist for routine preventative care. The incidence of primary cutaneous B-cell lymphoma is also rising, and it has become the job of the dermatologist to identify these patients. With attentive physical exams and awareness of the possibility of cutaneous lymphomas, the assiduous and skilled dermatologist can make a dramatic impact on the lives and health of their patients.
Dr. Pilcher is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Goldfaden is a practicing dermatologist at Affiliated Dermatologists in Morristown, NJ.
Dr. Rogachefsky is a practicing dermatologist and the Program Director of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologist Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-282.
2. Soyer PH, Rigel DS, Wurm EM. Actinic keratosis, basal cell carcinoma, and squamous cell carcinoma. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 108.
3. American Cancer Society. Cancer Facts & Figures 2015. https://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed March 23, 2015.
4. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768-3785.
5. Wilcox RA. Cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90(1):73-76.
6. Cerroni L. B-cell lymphomas of the skin. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 119.
7. Cho-Vega JH, Vega F, Rassidakis G, Medeiros LJ. Primary cutaneous marginal zone B-cell lymphoma. Am J Clin Pathol. 2006;125(suppl):S38-S49.
8. Servitje O, Gallardo F, Estrach T, et al. Primary cutaneous marginal zone B-cell lymphoma: a clinical, histopathological, immunophenotypic and molecular genetic study of 22 cases. Br J Dermatol. 2002;147(6):1147-1158.
9. Goodlad JR, Davidson MM, Hollowood K, Batstone P, Ho-Yen DO. Borrelia burgdorferi-associated cutaneous marginal zone lymphoma: a clinicopathlogical study of two cases illustrating the temporal progression of B. Burgdorferi-associated B-cell proliferation in the skin. Histopathology. 2000;37(6):501-508.
10. Kim YH, Willemze R, Pimpinelli N, et al. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(2):479-484.
11. Senff NJ, Noordijk EM, Kim YH, et al. European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for management of cutaneous B-cell lymphomas. Blood. 2008;112(5):1600-1609.
It is estimated in the United States approximately 1 in 5 people will develop skin cancer in their lifetime leading to more patients visiting a dermatologist for routine skin exams.1 As most skin cancers are asymptomatic, most patients are unaware of these worrisome lesions. The most common forms of skin cancer are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) with melanoma accounting for 2% of skin cancer cases.2,3 Rarely, more unusual types of skin cancer are identified on routine skin exams.
Primary cutaneous lymphomas are a heterogeneous group of extranodal non-Hodgkin lymphomas. They are defined as “malignant lymphomas confined to the skin at presentation after complete staging procedures.”4 The majority of cutaneous lymphomas are T cell but approximately 25% of these are B-cell derived lymphomas.5 The B-cell derived cutaneous lymphomas are classified into several major entities by the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC) including primary cutaneous follicle-center lymphoma, primary cutaneous diffuse large B-cell lymphoma leg type, primary cutaneous marginal zone lymphoma (PCMZL, also known as extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue [MALT lymphoma]), primary cutaneous diffuse large B-cell lymphoma, other and intravascular diffuse large B-cell lymphoma.4
The incidence of cutaneous B-cell lymphoma has been increasing and is 3.1 per million persons, based on Surveillance, Epidemiology and End Results registry data.5 At presentation, most of the patients do not have extracutaneous signs and symptoms; therefore, most of the cutaneous lymphomas are diagnosed by dermatologists.6 With the increasing incidence, dermatologists must be on the lookout for cases of cutaneous B-cell lymphoma. This article presents a case of PCMZL that was diagnosed on routine skin exam.
Case Presentation
A 61-year-old female presented to the general dermatology clinic for a routine skin exam. The patient has a past medical history of hypertension and uterine fibroids. She has a personal history of BCC that was resected by Mohs micrographic surgery as well as a family history of colon and lung cancer. She denied fevers, chills, night sweats and weight loss and all other review of systems were negative. Patient had no knowledge of any new or changing skin lesions or moles. She had no lesions that were hurting, itching or bleeding. A complete skin exam was performed.
A small 3 mm erythematous papule was noted on the left upper arm. The patient had not noticed the lesion prior to the exam and did not know how long it had been there. No other similar lesions were noted on exam. Due to its unique appearance, the lesion was biopsied (Figure 1).

Figure 1. Post-biopsy photograph of the lesion showing small size and normal surrounding skin.
Histopathologic analysis revealed a dermal nodule comprised of sheets of plasma cells mixed with small lymphoid cells with irregular nuclear outlines (Figure 2). Several immunohistochemical stains were done. The lesion was positive for both lambda and kappa immunoglobulin light chains with kappa staining being stronger than lambda staining. Further immunologic analysis could not be done due to the small size of the specimen.

Figure 2. Hematoxylin and eosin stain of the lesion.
Despite this, the combination of findings favored cutaneous marginal zone (MALT) lymphoma with marked plasmacytic differentiation. Based on the clinicopathologic correlation, the patient was diagnosed with PCMZL. The pathologist suggested additional workup to rule out systemic lymphoma or plasma cell dyscrasia.
Discussion
PCMZL is believed to be the cutaneous counterpart of extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.7 With the new WHO-EORTC classification that came out in 2008, cases previously classified as primary cutaneous immunocytoma or primary cutaneous plasmacytoma were reclassified as PCMZL with prominent lymphoplasmacytic or plasmacytic differentiation respectively.4 Due to these changes, PCMZL is now one of the most common forms of primary cutaneous B-cell lymphoma.8
The etiology of PCMZL is unclear. Because the clinicopathologic features observed in the gastric mucosa-associated lymphoid tissue, (MALT) lymphomas are similar to the PCMZL, many believe there is a similar cause. MALT lymphomas have been linked to long-standing antigenic stimulation possibly due to chronic infection with Helicobacter pylori.9
Several studies show this same antigen-driven lymphomagenesis in the skin could be secondary to Borrelia burgdorferi infection.7,9 Some case reports from Europe show that some of PCMZL lesions contain B burgdorferi gene sequences on polymerase chain reaction.7,10 Very few of these cases have been found in the United States. Most people believe that the geographic variation is due to the different genospecies of Borrelia.7 No other microorganism has been convincingly linked to the development of PCMZL, and in the United States, the B burgdorferi connection has not been established.5 Therefore, no definitive cause PCMZL is identified in the United States.
The preponderance of patients with PCMZL are men over the age of 40.8 PCMZL can present with multiple phenotypes. The most common presentation is pink-violet to red-brown papules, plaques or nodules.6,7 The lesions are usually localized on the extremities or trunk and can be solitary or multiple.7 The differential diagnosis includes other skin cancers such as BCC, SCC, amelanotic melanoma, other cutaneous lymphomas and reactive lymphoid hyperplasias such as lymphomatoid papulosis. Unlike other forms of skin cancer, the lesions rarely ulcerate and are typically asymptomatic. Systemic signs or symptoms including fever, night sweats, weight loss and malaise are typically not present.6 The lack of B-cell symptoms is concordant with the fact that PCMZL is usually skin localized; however, systemic disease can be present and staging workup is necessary.7
Diagnosis
The diagnosis of PCMZL is made by biopsy with careful morphologic and immunohistochemical analysis. Histology of PCMZL on hematoxylin and eosin stain shows dense, lymphocytic infiltrate found mainly in the dermis and subcutaneous fat. Epidermotropism is not a feature of PCMZL and a grenz zone is commonly observed.7 Cytologically PCMZL is characterized by a polymorphous infiltrate that includes marginal zone cells, centrocyte-like cells, monocytoid cells and/or blastoid cells.8 Also, plasma cells, eosinophils and small lymphocytes can be found in the infiltrate.6 Germinal centers that are reactive but can contain malignant cells can be seen in about 70% of cases.7 Positive staining with CD20, CD79a and Bcl-2 can be seen in the centrocyte-like cells, but these cells are negative for CD5, CD10 and Bcl-6.6 As in our patient, monotypic expression of immunoglobulin light chains can be observed especially in cases expressing plasmacytoid differentitiation.7
The International Society for Cutaneous Lymphomas (ISCL) and EORTC recently proposed staging recommendations for cutaneous lymphomas.10 Workup should include a history, physical examination, laboratory studies including a lactate dehydrogenase (LDH) and imaging of the chest, abdomen and pelvis with either a computed tomography (CT) scan, positron emission tomography (PET) scan or combination PET/CT.3 The ISCL did not recommend bone marrow biopsy for the PCMZL.10 The International Extranodal Lymphoma Study Group identified 3 independent prognostic factors for PCMZL: elevated LDH, >2 skin lesions and nodular lesions.5 These factors make up the cutaneous lymphoma international prognostic index, which states that the absence of any adverse prognostic factor was associated with a 5-year progression-free survival (PFS) of 91%.5 The presence of 2 or 3 adverse prognostic factors was associated with a 5-year PFS of 48%.5 Most of the relapses seen are local relapses. Despite this, the overall 5-year disease specific survival is greater than 95% with PCMZL.5
Treatment
Patients with solitary lesions or a few grouped lesions of PCMZL can be treated by local radiotherapy, simple surgical excision or surgical excision followed by radiotherapy of the field.6,7
Radiation therapy is associated with a high response rate especially if associated with wide margin in the radiation field.5,6 One study showed complete remission after initial therapy was reached in 130 out of 132 patients.11 Systemic disease is more difficult to treat. Some advocate treating asymptomatic disease with observation.5 However, once patients with systemic disease have become symptomatic, corticosteroids, systemic interferon alfa, polychemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisone) and anti-CD20 monoclonal antibodies have been used with variable results.7 An initial trial of antibiotics due to the possible association of B burgdorferi has been recommended, but may not be useful for North American patients.5
Patient Outcome
Our patient was referred to a hematologist oncologist who did a staging workup. She received a CT scan as well as blood work including a complete metabolic panel, LDH level and a complete blood count with differential. The blood work was within normal limits and the CT scan did not show any evidence of other disease. The oncologist classified her as stage I skin limited PCMZL. Patient was referred to radiation oncology for local radiation therapy to the left arm.
Conclusion
The incidence of skin cancer continues to rise in the United States, and many patients are presenting to the dermatologist for routine preventative care. The incidence of primary cutaneous B-cell lymphoma is also rising, and it has become the job of the dermatologist to identify these patients. With attentive physical exams and awareness of the possibility of cutaneous lymphomas, the assiduous and skilled dermatologist can make a dramatic impact on the lives and health of their patients.
Dr. Pilcher is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Goldfaden is a practicing dermatologist at Affiliated Dermatologists in Morristown, NJ.
Dr. Rogachefsky is a practicing dermatologist and the Program Director of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologist Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-282.
2. Soyer PH, Rigel DS, Wurm EM. Actinic keratosis, basal cell carcinoma, and squamous cell carcinoma. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 108.
3. American Cancer Society. Cancer Facts & Figures 2015. https://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed March 23, 2015.
4. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768-3785.
5. Wilcox RA. Cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90(1):73-76.
6. Cerroni L. B-cell lymphomas of the skin. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 119.
7. Cho-Vega JH, Vega F, Rassidakis G, Medeiros LJ. Primary cutaneous marginal zone B-cell lymphoma. Am J Clin Pathol. 2006;125(suppl):S38-S49.
8. Servitje O, Gallardo F, Estrach T, et al. Primary cutaneous marginal zone B-cell lymphoma: a clinical, histopathological, immunophenotypic and molecular genetic study of 22 cases. Br J Dermatol. 2002;147(6):1147-1158.
9. Goodlad JR, Davidson MM, Hollowood K, Batstone P, Ho-Yen DO. Borrelia burgdorferi-associated cutaneous marginal zone lymphoma: a clinicopathlogical study of two cases illustrating the temporal progression of B. Burgdorferi-associated B-cell proliferation in the skin. Histopathology. 2000;37(6):501-508.
10. Kim YH, Willemze R, Pimpinelli N, et al. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(2):479-484.
11. Senff NJ, Noordijk EM, Kim YH, et al. European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for management of cutaneous B-cell lymphomas. Blood. 2008;112(5):1600-1609.
It is estimated in the United States approximately 1 in 5 people will develop skin cancer in their lifetime leading to more patients visiting a dermatologist for routine skin exams.1 As most skin cancers are asymptomatic, most patients are unaware of these worrisome lesions. The most common forms of skin cancer are basal cell carcinoma (BCC) and squamous cell carcinoma (SCC) with melanoma accounting for 2% of skin cancer cases.2,3 Rarely, more unusual types of skin cancer are identified on routine skin exams.
Primary cutaneous lymphomas are a heterogeneous group of extranodal non-Hodgkin lymphomas. They are defined as “malignant lymphomas confined to the skin at presentation after complete staging procedures.”4 The majority of cutaneous lymphomas are T cell but approximately 25% of these are B-cell derived lymphomas.5 The B-cell derived cutaneous lymphomas are classified into several major entities by the World Health Organization (WHO) and the European Organization for Research and Treatment of Cancer (EORTC) including primary cutaneous follicle-center lymphoma, primary cutaneous diffuse large B-cell lymphoma leg type, primary cutaneous marginal zone lymphoma (PCMZL, also known as extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue [MALT lymphoma]), primary cutaneous diffuse large B-cell lymphoma, other and intravascular diffuse large B-cell lymphoma.4
The incidence of cutaneous B-cell lymphoma has been increasing and is 3.1 per million persons, based on Surveillance, Epidemiology and End Results registry data.5 At presentation, most of the patients do not have extracutaneous signs and symptoms; therefore, most of the cutaneous lymphomas are diagnosed by dermatologists.6 With the increasing incidence, dermatologists must be on the lookout for cases of cutaneous B-cell lymphoma. This article presents a case of PCMZL that was diagnosed on routine skin exam.
Case Presentation
A 61-year-old female presented to the general dermatology clinic for a routine skin exam. The patient has a past medical history of hypertension and uterine fibroids. She has a personal history of BCC that was resected by Mohs micrographic surgery as well as a family history of colon and lung cancer. She denied fevers, chills, night sweats and weight loss and all other review of systems were negative. Patient had no knowledge of any new or changing skin lesions or moles. She had no lesions that were hurting, itching or bleeding. A complete skin exam was performed.
A small 3 mm erythematous papule was noted on the left upper arm. The patient had not noticed the lesion prior to the exam and did not know how long it had been there. No other similar lesions were noted on exam. Due to its unique appearance, the lesion was biopsied (Figure 1).
Figure 1. Post-biopsy photograph of the lesion showing small size and normal surrounding skin.
Histopathologic analysis revealed a dermal nodule comprised of sheets of plasma cells mixed with small lymphoid cells with irregular nuclear outlines (Figure 2). Several immunohistochemical stains were done. The lesion was positive for both lambda and kappa immunoglobulin light chains with kappa staining being stronger than lambda staining. Further immunologic analysis could not be done due to the small size of the specimen.
Figure 2. Hematoxylin and eosin stain of the lesion.
Despite this, the combination of findings favored cutaneous marginal zone (MALT) lymphoma with marked plasmacytic differentiation. Based on the clinicopathologic correlation, the patient was diagnosed with PCMZL. The pathologist suggested additional workup to rule out systemic lymphoma or plasma cell dyscrasia.
Discussion
PCMZL is believed to be the cutaneous counterpart of extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue.7 With the new WHO-EORTC classification that came out in 2008, cases previously classified as primary cutaneous immunocytoma or primary cutaneous plasmacytoma were reclassified as PCMZL with prominent lymphoplasmacytic or plasmacytic differentiation respectively.4 Due to these changes, PCMZL is now one of the most common forms of primary cutaneous B-cell lymphoma.8
The etiology of PCMZL is unclear. Because the clinicopathologic features observed in the gastric mucosa-associated lymphoid tissue, (MALT) lymphomas are similar to the PCMZL, many believe there is a similar cause. MALT lymphomas have been linked to long-standing antigenic stimulation possibly due to chronic infection with Helicobacter pylori.9
Several studies show this same antigen-driven lymphomagenesis in the skin could be secondary to Borrelia burgdorferi infection.7,9 Some case reports from Europe show that some of PCMZL lesions contain B burgdorferi gene sequences on polymerase chain reaction.7,10 Very few of these cases have been found in the United States. Most people believe that the geographic variation is due to the different genospecies of Borrelia.7 No other microorganism has been convincingly linked to the development of PCMZL, and in the United States, the B burgdorferi connection has not been established.5 Therefore, no definitive cause PCMZL is identified in the United States.
The preponderance of patients with PCMZL are men over the age of 40.8 PCMZL can present with multiple phenotypes. The most common presentation is pink-violet to red-brown papules, plaques or nodules.6,7 The lesions are usually localized on the extremities or trunk and can be solitary or multiple.7 The differential diagnosis includes other skin cancers such as BCC, SCC, amelanotic melanoma, other cutaneous lymphomas and reactive lymphoid hyperplasias such as lymphomatoid papulosis. Unlike other forms of skin cancer, the lesions rarely ulcerate and are typically asymptomatic. Systemic signs or symptoms including fever, night sweats, weight loss and malaise are typically not present.6 The lack of B-cell symptoms is concordant with the fact that PCMZL is usually skin localized; however, systemic disease can be present and staging workup is necessary.7
Diagnosis
The diagnosis of PCMZL is made by biopsy with careful morphologic and immunohistochemical analysis. Histology of PCMZL on hematoxylin and eosin stain shows dense, lymphocytic infiltrate found mainly in the dermis and subcutaneous fat. Epidermotropism is not a feature of PCMZL and a grenz zone is commonly observed.7 Cytologically PCMZL is characterized by a polymorphous infiltrate that includes marginal zone cells, centrocyte-like cells, monocytoid cells and/or blastoid cells.8 Also, plasma cells, eosinophils and small lymphocytes can be found in the infiltrate.6 Germinal centers that are reactive but can contain malignant cells can be seen in about 70% of cases.7 Positive staining with CD20, CD79a and Bcl-2 can be seen in the centrocyte-like cells, but these cells are negative for CD5, CD10 and Bcl-6.6 As in our patient, monotypic expression of immunoglobulin light chains can be observed especially in cases expressing plasmacytoid differentitiation.7
The International Society for Cutaneous Lymphomas (ISCL) and EORTC recently proposed staging recommendations for cutaneous lymphomas.10 Workup should include a history, physical examination, laboratory studies including a lactate dehydrogenase (LDH) and imaging of the chest, abdomen and pelvis with either a computed tomography (CT) scan, positron emission tomography (PET) scan or combination PET/CT.3 The ISCL did not recommend bone marrow biopsy for the PCMZL.10 The International Extranodal Lymphoma Study Group identified 3 independent prognostic factors for PCMZL: elevated LDH, >2 skin lesions and nodular lesions.5 These factors make up the cutaneous lymphoma international prognostic index, which states that the absence of any adverse prognostic factor was associated with a 5-year progression-free survival (PFS) of 91%.5 The presence of 2 or 3 adverse prognostic factors was associated with a 5-year PFS of 48%.5 Most of the relapses seen are local relapses. Despite this, the overall 5-year disease specific survival is greater than 95% with PCMZL.5
Treatment
Patients with solitary lesions or a few grouped lesions of PCMZL can be treated by local radiotherapy, simple surgical excision or surgical excision followed by radiotherapy of the field.6,7
Radiation therapy is associated with a high response rate especially if associated with wide margin in the radiation field.5,6 One study showed complete remission after initial therapy was reached in 130 out of 132 patients.11 Systemic disease is more difficult to treat. Some advocate treating asymptomatic disease with observation.5 However, once patients with systemic disease have become symptomatic, corticosteroids, systemic interferon alfa, polychemotherapy (cyclophosphamide, doxorubicin, vincristine and prednisone) and anti-CD20 monoclonal antibodies have been used with variable results.7 An initial trial of antibiotics due to the possible association of B burgdorferi has been recommended, but may not be useful for North American patients.5
Patient Outcome
Our patient was referred to a hematologist oncologist who did a staging workup. She received a CT scan as well as blood work including a complete metabolic panel, LDH level and a complete blood count with differential. The blood work was within normal limits and the CT scan did not show any evidence of other disease. The oncologist classified her as stage I skin limited PCMZL. Patient was referred to radiation oncology for local radiation therapy to the left arm.
Conclusion
The incidence of skin cancer continues to rise in the United States, and many patients are presenting to the dermatologist for routine preventative care. The incidence of primary cutaneous B-cell lymphoma is also rising, and it has become the job of the dermatologist to identify these patients. With attentive physical exams and awareness of the possibility of cutaneous lymphomas, the assiduous and skilled dermatologist can make a dramatic impact on the lives and health of their patients.
Dr. Pilcher is a fellow at Affiliated Dermatologists in Morristown, NJ.
Dr. Goldfaden is a practicing dermatologist at Affiliated Dermatologists in Morristown, NJ.
Dr. Rogachefsky is a practicing dermatologist and the Program Director of the ACGME-approved Procedural Dermatology Fellowship at Affiliated Dermatologists & Dermatologist Surgeons in Morristown, NJ.
Disclosure: The authors report no relevant financial relationships.
References
1. Stern RS. Prevalence of a history of skin cancer in 2007: results of an incidence-based model. Arch Dermatol. 2010;146(3):279-282.
2. Soyer PH, Rigel DS, Wurm EM. Actinic keratosis, basal cell carcinoma, and squamous cell carcinoma. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 108.
3. American Cancer Society. Cancer Facts & Figures 2015. https://www.cancer.org/acs/groups/content/@editorial/documents/document/acspc-044552.pdf. Accessed March 23, 2015.
4. Willemze R, Jaffe ES, Burg G, et al. WHO-EORTC classification for cutaneous lymphomas. Blood. 2005;105(10):3768-3785.
5. Wilcox RA. Cutaneous B-cell lymphomas: 2015 update on diagnosis, risk-stratification, and management. Am J Hematol. 2015;90(1):73-76.
6. Cerroni L. B-cell lymphomas of the skin. In: Bolognia JL, Jorizzo JL, Schaffer JV, eds. Dermatology. 3rd ed. Philadelphia, PA: Elsevier, Inc; 2012:chap 119.
7. Cho-Vega JH, Vega F, Rassidakis G, Medeiros LJ. Primary cutaneous marginal zone B-cell lymphoma. Am J Clin Pathol. 2006;125(suppl):S38-S49.
8. Servitje O, Gallardo F, Estrach T, et al. Primary cutaneous marginal zone B-cell lymphoma: a clinical, histopathological, immunophenotypic and molecular genetic study of 22 cases. Br J Dermatol. 2002;147(6):1147-1158.
9. Goodlad JR, Davidson MM, Hollowood K, Batstone P, Ho-Yen DO. Borrelia burgdorferi-associated cutaneous marginal zone lymphoma: a clinicopathlogical study of two cases illustrating the temporal progression of B. Burgdorferi-associated B-cell proliferation in the skin. Histopathology. 2000;37(6):501-508.
10. Kim YH, Willemze R, Pimpinelli N, et al. TNM classification system for primary cutaneous lymphomas other than mycosis fungoides and Sezary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the Cutaneous Lymphoma Task Force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(2):479-484.
11. Senff NJ, Noordijk EM, Kim YH, et al. European Organization for Research and Treatment of Cancer and International Society for Cutaneous Lymphoma consensus recommendations for management of cutaneous B-cell lymphomas. Blood. 2008;112(5):1600-1609.











