A 32-year-old Caucasian male was referred to the dermatology clinic for alternative treatment options after an initial clinical diagnosis and a skin biopsy that suggested lymphomatoid papulosis. Prior to his presentation, the patient was treated with topical triamcinolone 0.1% ointment twice daily and cyclosporine 3 mg/kg/d for 2 months with the intention of transitioning to methotrexate once pruritus was controlled. The patient’s history was pertinent for a rash of 3 months duration that began after a trip to Baja, Mexico.
On physical examination, there were excoriated, red papules in his axillae, groin, genitalia and buttocks. There were also scattered crusted and healing scars on the lower abdomen and pubic areas (Figure 1). Aside from extreme pruritus, review of his systems was negative. A skin scraping was obtained from a crusted papule and examined with potassium hydroxide preparation. A previous biopsy showed dense, wedge-shaped infiltrate of lymphocytes, eosinophils and large atypical lymphocytes that demonstrated CD30+ staining.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Scabies Mimicking Lymphomatoid Papulosis
Given the history of travel, clinical presentation and chronic history of pruritus, a diagnosis of scabies was suggested, hence the scraping and potassium hydroxide (KOH) preparation for microscopic examination, which showed scabies mites. Figures 1-2 show clinical presentation.

Figure1. Excoriated red papules on the lower abdomen and pubic area.

Figure 2. Crusting and healing scars.
Our clinical differential diagnosis at presentation also included CD30-positive lymphoproliferative disorders (or primary cutaneous anaplastic large cell lymphoma) and benign inflammatory diseases with atypical CD30-positive cells (drug-induced CD30+ T-cell pseudolymphoma, other chronic arthropod assault, syphilis and chronic allergic contact dermatitis).
Scabies is a common, highly pruritic infestation of the skin caused by Sarcoptes scabiei var. hominis. It is a very contagious parasitosis with specific lesions, such as burrows, and non-specific lesions, such as papules, vesicles and excoriations. The typical areas of the body it affects are finger webs, wrists, axillary folds, abdomen, buttocks, inframammary folds and genitalia. It is spread through close personal contact. The definitive diagnosis is made when the scabies mites or their eggs or fecal pellets (scybala) can be identified on a light microscope or newer epiluminescence microscopy.1
Even in cases of eruption associated with scabies, the mite detection rate varies widely from 10% to 60% in some reports.2-5 Nodular scabies may be difficult to diagnose due to presence of dense lymphocytic infiltrate.6 Figures 3-5 show histologic features of changes induced by scabies mite infestation.
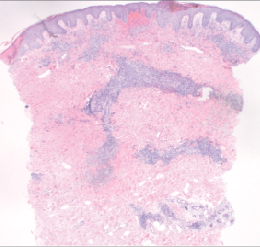
Figure 3. Punch biopsy: hematoxylin and esosin. Dense, nodular infiltrate arranged in superficial and deep pattern – 40x.
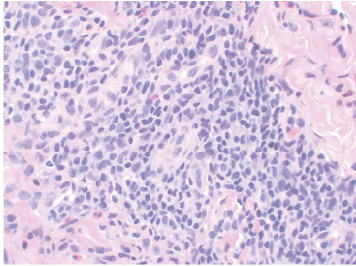
Figure 4. Large atypical lymphocytes – 400x.
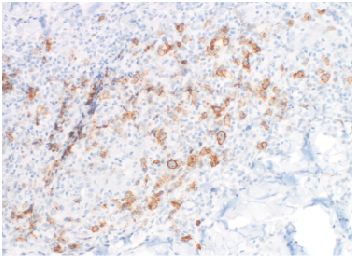
Figure 5. Large atypical lymphocytes demonstrating CD30+ staining – 100x.
Differential Diagnosis
The differential diagnosis between arthropod assault in general and lymphoproliferative disorders is a well-known pitfall in dermatopathology; a correct diagnosis can be made by careful clinicopathologic correlation.2
CD30 is a type 1 transmembrane glycoprotein, member of tumor necrosis factor family. Its expression can be induced on lymphoid cells of both B- and T-cell lineage. Expression of CD30 antigen is a distinct marker of lymphocyte activation that was originally described in the Reed-Sternberg cells of Hodgkin’s disease. The observation of CD30+ cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations. However, CD30 expression has also been reported in some cutaneous benign inflammatory infiltrates.6
The most common reactive conditions that can simulate CD30 lymphoproliferative conditions, include arthropod bite reactions, various viral infections, pityriasis lichenoides and lymphocytic papules in myelodysplastic syndrome.7 Viruses are the most common cause for presence of CD30-positive cells in cutaneous inflammatory infiltrates and a viral infection must always be suspected.8
Management
The most common topical treatments for scabies include lindane and permethrin. Permethrin provides a greater margin of tolerability because of its low inherent toxicity and low percutaneous absorption. Oral ivermectin is the most recently developed treatment for scabies. A single, oral dose of ivermectin 200 µg/kg (which is roughly 1 mg/10 lb body weight) given as a single dose and repeated in a week is a well-tolerated and very effective treatment.5
Our Patient
KOH preparation revealed a S scabiei mite. The patient was diagnosed with chronic scabies infestation and improved with oral ivermectin 12 mg by mouth and topical permethrin 5% x 2 doses 7 days apart.
Conclusion
While the presence of CD30+ T cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations, the clinician must consider chronic benign inflammatory diseases because expression of CD30 antigen is a distinct marker of lymphocyte activation and is not unique to neoplastic skin conditions.7
This case lends merit to dermatologic dogma often taught in dermatology residency training that, “If there is scale, you should scrape it for KOH preparation.” Also, travel history to less-industrialized countries should always raise the clinician’s suspicion for infection and infestation. n
Dr. Dougherty is a dermatologist in private practice in Santa Barbara, CA.
Disclosure: The author reports no relevant financial relationships.
References
1. Executive Committee of Guideline for the Diagnosis and Treatment of Scabies. Guideline for the diagnosis and treatment of scabies in Japan (second edition). J Dermatol. 2008;35(6):378-393.
2. Juranek DD. Scabies control in institutions. In: Orkin M, Maibach HI, eds. Cutaneous Infestations and Insect Bites. New York, NY: Marcel Dekker; 1985:139-156.
3. Ishii N, Miyazawa M, Kawaguchi H, Inami S, Nakajima H. Statistical analysis of scabies. STD. 1989;70:19-21.
4. Lettau LA. Nosocomial transmission and infection control aspects of parasitic and ectoparasitic diseases. Part III. Ectoparasites/summary and conclusions. Infect Control Hosp Epidemiol. 1991;12(3):179-185.
5. Chouela E, Abeldano A, Pellerano G, Hernandez MI. Diagnosis and treatment of scabies: a practical guide. Am J Clin Dermatol. 2002;3(1):9-18.
6. Gallardo F, Barranco C, Toll A, Pujol RM. CD30 antigen expression in cutaneous inflammatory infiltrates of scabies: a dynamic immunophenotypic pattern that should be distinguished from lymphomatoid papulosis. J Cutan Pathol. 2002;29(6):368-373.
7. Guitart J, Querfeld C. Cutaneous CD30 lymphoproliferative disorders and similar conditions: a clinical and pathologic prospective on a complex issue. Semin Diag Pathol. 2009;26(3):131-140.
8. Werner B, Massone C, Keri H, Cerroni L. Large CD 30-positive cells in benign atypical lymphoid infiltrates of the skin. J Cut Path 2008;35(12):1100-1107.
A 32-year-old Caucasian male was referred to the dermatology clinic for alternative treatment options after an initial clinical diagnosis and a skin biopsy that suggested lymphomatoid papulosis. Prior to his presentation, the patient was treated with topical triamcinolone 0.1% ointment twice daily and cyclosporine 3 mg/kg/d for 2 months with the intention of transitioning to methotrexate once pruritus was controlled. The patient’s history was pertinent for a rash of 3 months duration that began after a trip to Baja, Mexico.
On physical examination, there were excoriated, red papules in his axillae, groin, genitalia and buttocks. There were also scattered crusted and healing scars on the lower abdomen and pubic areas (Figure 1). Aside from extreme pruritus, review of his systems was negative. A skin scraping was obtained from a crusted papule and examined with potassium hydroxide preparation. A previous biopsy showed dense, wedge-shaped infiltrate of lymphocytes, eosinophils and large atypical lymphocytes that demonstrated CD30+ staining.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Scabies Mimicking Lymphomatoid Papulosis
Given the history of travel, clinical presentation and chronic history of pruritus, a diagnosis of scabies was suggested, hence the scraping and potassium hydroxide (KOH) preparation for microscopic examination, which showed scabies mites. Figures 1-2 show clinical presentation.

Figure1. Excoriated red papules on the lower abdomen and pubic area.

Figure 2. Crusting and healing scars.
Our clinical differential diagnosis at presentation also included CD30-positive lymphoproliferative disorders (or primary cutaneous anaplastic large cell lymphoma) and benign inflammatory diseases with atypical CD30-positive cells (drug-induced CD30+ T-cell pseudolymphoma, other chronic arthropod assault, syphilis and chronic allergic contact dermatitis).
Scabies is a common, highly pruritic infestation of the skin caused by Sarcoptes scabiei var. hominis. It is a very contagious parasitosis with specific lesions, such as burrows, and non-specific lesions, such as papules, vesicles and excoriations. The typical areas of the body it affects are finger webs, wrists, axillary folds, abdomen, buttocks, inframammary folds and genitalia. It is spread through close personal contact. The definitive diagnosis is made when the scabies mites or their eggs or fecal pellets (scybala) can be identified on a light microscope or newer epiluminescence microscopy.1
Even in cases of eruption associated with scabies, the mite detection rate varies widely from 10% to 60% in some reports.2-5 Nodular scabies may be difficult to diagnose due to presence of dense lymphocytic infiltrate.6 Figures 3-5 show histologic features of changes induced by scabies mite infestation.

Figure 3. Punch biopsy: hematoxylin and esosin. Dense, nodular infiltrate arranged in superficial and deep pattern – 40x.

Figure 4. Large atypical lymphocytes – 400x.

Figure 5. Large atypical lymphocytes demonstrating CD30+ staining – 100x.
Differential Diagnosis
The differential diagnosis between arthropod assault in general and lymphoproliferative disorders is a well-known pitfall in dermatopathology; a correct diagnosis can be made by careful clinicopathologic correlation.2
CD30 is a type 1 transmembrane glycoprotein, member of tumor necrosis factor family. Its expression can be induced on lymphoid cells of both B- and T-cell lineage. Expression of CD30 antigen is a distinct marker of lymphocyte activation that was originally described in the Reed-Sternberg cells of Hodgkin’s disease. The observation of CD30+ cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations. However, CD30 expression has also been reported in some cutaneous benign inflammatory infiltrates.6
The most common reactive conditions that can simulate CD30 lymphoproliferative conditions, include arthropod bite reactions, various viral infections, pityriasis lichenoides and lymphocytic papules in myelodysplastic syndrome.7 Viruses are the most common cause for presence of CD30-positive cells in cutaneous inflammatory infiltrates and a viral infection must always be suspected.8
Management
The most common topical treatments for scabies include lindane and permethrin. Permethrin provides a greater margin of tolerability because of its low inherent toxicity and low percutaneous absorption. Oral ivermectin is the most recently developed treatment for scabies. A single, oral dose of ivermectin 200 µg/kg (which is roughly 1 mg/10 lb body weight) given as a single dose and repeated in a week is a well-tolerated and very effective treatment.5
Our Patient
KOH preparation revealed a S scabiei mite. The patient was diagnosed with chronic scabies infestation and improved with oral ivermectin 12 mg by mouth and topical permethrin 5% x 2 doses 7 days apart.
Conclusion
While the presence of CD30+ T cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations, the clinician must consider chronic benign inflammatory diseases because expression of CD30 antigen is a distinct marker of lymphocyte activation and is not unique to neoplastic skin conditions.7
This case lends merit to dermatologic dogma often taught in dermatology residency training that, “If there is scale, you should scrape it for KOH preparation.” Also, travel history to less-industrialized countries should always raise the clinician’s suspicion for infection and infestation. n
Dr. Dougherty is a dermatologist in private practice in Santa Barbara, CA.
Disclosure: The author reports no relevant financial relationships.
References
1. Executive Committee of Guideline for the Diagnosis and Treatment of Scabies. Guideline for the diagnosis and treatment of scabies in Japan (second edition). J Dermatol. 2008;35(6):378-393.
2. Juranek DD. Scabies control in institutions. In: Orkin M, Maibach HI, eds. Cutaneous Infestations and Insect Bites. New York, NY: Marcel Dekker; 1985:139-156.
3. Ishii N, Miyazawa M, Kawaguchi H, Inami S, Nakajima H. Statistical analysis of scabies. STD. 1989;70:19-21.
4. Lettau LA. Nosocomial transmission and infection control aspects of parasitic and ectoparasitic diseases. Part III. Ectoparasites/summary and conclusions. Infect Control Hosp Epidemiol. 1991;12(3):179-185.
5. Chouela E, Abeldano A, Pellerano G, Hernandez MI. Diagnosis and treatment of scabies: a practical guide. Am J Clin Dermatol. 2002;3(1):9-18.
6. Gallardo F, Barranco C, Toll A, Pujol RM. CD30 antigen expression in cutaneous inflammatory infiltrates of scabies: a dynamic immunophenotypic pattern that should be distinguished from lymphomatoid papulosis. J Cutan Pathol. 2002;29(6):368-373.
7. Guitart J, Querfeld C. Cutaneous CD30 lymphoproliferative disorders and similar conditions: a clinical and pathologic prospective on a complex issue. Semin Diag Pathol. 2009;26(3):131-140.
8. Werner B, Massone C, Keri H, Cerroni L. Large CD 30-positive cells in benign atypical lymphoid infiltrates of the skin. J Cut Path 2008;35(12):1100-1107.
A 32-year-old Caucasian male was referred to the dermatology clinic for alternative treatment options after an initial clinical diagnosis and a skin biopsy that suggested lymphomatoid papulosis. Prior to his presentation, the patient was treated with topical triamcinolone 0.1% ointment twice daily and cyclosporine 3 mg/kg/d for 2 months with the intention of transitioning to methotrexate once pruritus was controlled. The patient’s history was pertinent for a rash of 3 months duration that began after a trip to Baja, Mexico.
On physical examination, there were excoriated, red papules in his axillae, groin, genitalia and buttocks. There were also scattered crusted and healing scars on the lower abdomen and pubic areas (Figure 1). Aside from extreme pruritus, review of his systems was negative. A skin scraping was obtained from a crusted papule and examined with potassium hydroxide preparation. A previous biopsy showed dense, wedge-shaped infiltrate of lymphocytes, eosinophils and large atypical lymphocytes that demonstrated CD30+ staining.
WHAT IS YOUR DIAGNOSIS?
Diagnosis: Scabies Mimicking Lymphomatoid Papulosis
Given the history of travel, clinical presentation and chronic history of pruritus, a diagnosis of scabies was suggested, hence the scraping and potassium hydroxide (KOH) preparation for microscopic examination, which showed scabies mites. Figures 1-2 show clinical presentation.
Figure1. Excoriated red papules on the lower abdomen and pubic area.
Figure 2. Crusting and healing scars.
Our clinical differential diagnosis at presentation also included CD30-positive lymphoproliferative disorders (or primary cutaneous anaplastic large cell lymphoma) and benign inflammatory diseases with atypical CD30-positive cells (drug-induced CD30+ T-cell pseudolymphoma, other chronic arthropod assault, syphilis and chronic allergic contact dermatitis).
Scabies is a common, highly pruritic infestation of the skin caused by Sarcoptes scabiei var. hominis. It is a very contagious parasitosis with specific lesions, such as burrows, and non-specific lesions, such as papules, vesicles and excoriations. The typical areas of the body it affects are finger webs, wrists, axillary folds, abdomen, buttocks, inframammary folds and genitalia. It is spread through close personal contact. The definitive diagnosis is made when the scabies mites or their eggs or fecal pellets (scybala) can be identified on a light microscope or newer epiluminescence microscopy.1
Even in cases of eruption associated with scabies, the mite detection rate varies widely from 10% to 60% in some reports.2-5 Nodular scabies may be difficult to diagnose due to presence of dense lymphocytic infiltrate.6 Figures 3-5 show histologic features of changes induced by scabies mite infestation.
Figure 3. Punch biopsy: hematoxylin and esosin. Dense, nodular infiltrate arranged in superficial and deep pattern – 40x.
Figure 4. Large atypical lymphocytes – 400x.
Figure 5. Large atypical lymphocytes demonstrating CD30+ staining – 100x.
Differential Diagnosis
The differential diagnosis between arthropod assault in general and lymphoproliferative disorders is a well-known pitfall in dermatopathology; a correct diagnosis can be made by careful clinicopathologic correlation.2
CD30 is a type 1 transmembrane glycoprotein, member of tumor necrosis factor family. Its expression can be induced on lymphoid cells of both B- and T-cell lineage. Expression of CD30 antigen is a distinct marker of lymphocyte activation that was originally described in the Reed-Sternberg cells of Hodgkin’s disease. The observation of CD30+ cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations. However, CD30 expression has also been reported in some cutaneous benign inflammatory infiltrates.6
The most common reactive conditions that can simulate CD30 lymphoproliferative conditions, include arthropod bite reactions, various viral infections, pityriasis lichenoides and lymphocytic papules in myelodysplastic syndrome.7 Viruses are the most common cause for presence of CD30-positive cells in cutaneous inflammatory infiltrates and a viral infection must always be suspected.8
Management
The most common topical treatments for scabies include lindane and permethrin. Permethrin provides a greater margin of tolerability because of its low inherent toxicity and low percutaneous absorption. Oral ivermectin is the most recently developed treatment for scabies. A single, oral dose of ivermectin 200 µg/kg (which is roughly 1 mg/10 lb body weight) given as a single dose and repeated in a week is a well-tolerated and very effective treatment.5
Our Patient
KOH preparation revealed a S scabiei mite. The patient was diagnosed with chronic scabies infestation and improved with oral ivermectin 12 mg by mouth and topical permethrin 5% x 2 doses 7 days apart.
Conclusion
While the presence of CD30+ T cells has been considered a diagnostic feature of cutaneous CD30 lymphoid proliferations, the clinician must consider chronic benign inflammatory diseases because expression of CD30 antigen is a distinct marker of lymphocyte activation and is not unique to neoplastic skin conditions.7
This case lends merit to dermatologic dogma often taught in dermatology residency training that, “If there is scale, you should scrape it for KOH preparation.” Also, travel history to less-industrialized countries should always raise the clinician’s suspicion for infection and infestation. n
Dr. Dougherty is a dermatologist in private practice in Santa Barbara, CA.
Disclosure: The author reports no relevant financial relationships.
References
1. Executive Committee of Guideline for the Diagnosis and Treatment of Scabies. Guideline for the diagnosis and treatment of scabies in Japan (second edition). J Dermatol. 2008;35(6):378-393.
2. Juranek DD. Scabies control in institutions. In: Orkin M, Maibach HI, eds. Cutaneous Infestations and Insect Bites. New York, NY: Marcel Dekker; 1985:139-156.
3. Ishii N, Miyazawa M, Kawaguchi H, Inami S, Nakajima H. Statistical analysis of scabies. STD. 1989;70:19-21.
4. Lettau LA. Nosocomial transmission and infection control aspects of parasitic and ectoparasitic diseases. Part III. Ectoparasites/summary and conclusions. Infect Control Hosp Epidemiol. 1991;12(3):179-185.
5. Chouela E, Abeldano A, Pellerano G, Hernandez MI. Diagnosis and treatment of scabies: a practical guide. Am J Clin Dermatol. 2002;3(1):9-18.
6. Gallardo F, Barranco C, Toll A, Pujol RM. CD30 antigen expression in cutaneous inflammatory infiltrates of scabies: a dynamic immunophenotypic pattern that should be distinguished from lymphomatoid papulosis. J Cutan Pathol. 2002;29(6):368-373.
7. Guitart J, Querfeld C. Cutaneous CD30 lymphoproliferative disorders and similar conditions: a clinical and pathologic prospective on a complex issue. Semin Diag Pathol. 2009;26(3):131-140.
8. Werner B, Massone C, Keri H, Cerroni L. Large CD 30-positive cells in benign atypical lymphoid infiltrates of the skin. J Cut Path 2008;35(12):1100-1107.












