Patient Presentation

 A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Angiolymphoid Hyperplasia With Eosinophilia (ALHE)
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an uncommon, benign vascular proliferation characterized by the presence of histologically distinct endothelial cells forming vessels. ALHE was first described by Wells and Whimster in 1969 as a late stage of Kimura’s disease and was later determined to be a histologically distinct entity.1,2 ALHE occurs most frequently in young to middle-age adults with a predilection for females,3 although it can occur in children and the elderly.
ALHE typically presents as multiple pink to reddish brown smooth-topped, dome-shaped papules or nodules on the head and neck, especially on the scalp and periauricular region.4 Rarely, lesions have been described in the mouth, trunk, extremities, genitals, muscle and bone.5-8 The papules may be isolated or grouped or may occur as plaques. Individual lesions seldom exceed
2 cm to 3 cm.9 A history of trauma to the area has been suggested as an inciting factor. Symptoms of ALHE lesions include pain, pruritus, pulsatile quality and bleeding after minor trauma.10 Regional lymph node enlargement and peripheral eosinophilia may be present in up to 20% of cases.3
Differential Diagnosis
ALHE may appear clinically similar to a variety of malignant and benign tumors. Most commonly, ALHE may be confused with Kaposi’s sarcoma, angiosarcoma, lymphoma cutis or vascularized metastases. Other conditions that may mimic ALHE include hemangiomas, pyogenic granulomas and sarcoidosis.
Histopathology
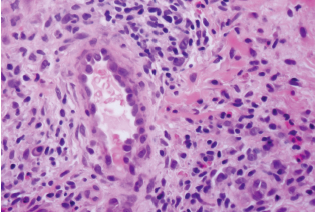
 Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
The vascular component of ALHE contains vessels of varying sizes, lined by plump endothelial cells that may project into the lumen, creating a distinct hobnailed appearance. These hobnailed endothelial cells contain a large nucleus with abundant eosinophilic cytoplasm and are characteristic of ALHE. Cytoplasmic vacuoles are seen in some cells, and may represent primitive vascular lumen. A muscular artery is often present at the center of the lesion.11 The thick walls of the larger vessels may demonstrate prominent myxoid degeneration. Mitotic figures may sometimes be present.
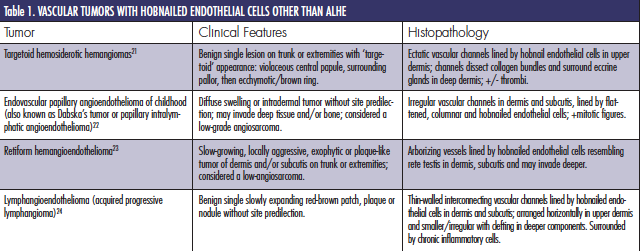
 Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
The pathophysiology of ALHE is still largely unknown. There is often mural damage or rupture in the large vessels of ALHE, which may suggest trauma or arteriovenous shunting as a mode of pathogenesis.8 Others have suggested that ALHE represents an abnormal vascular hypersensitivity reaction due to dysregulated expression of vasculogenic factors occurring from trauma or vascular malformations.13,14
Dermatoscopy
Dermatoscopy for the diagnosis of pigmented lesions is commonly employed, but its utility in identifying vascular lesions has yet to be determined.15 To our knowledge, we demonstrate the first report of the dermatoscopic features of ALHE. In our patient, the papules of ALHE demonstrate a diffuse reddish-brown erythema and whitish globules with fine vessels on the surface of the papules. The typical lacunae (red, blue, black) of hemangiomatous lesions were not appreciated. The reddish-brown erythema may represent the mixed inflammatory infiltrate overlying the vascular components of ALHE and the whitish globules may represent fibrotic stroma. Further dermatoscopic descriptions should be done to better delineate the features of ALHE and potentially aid in diagnosis.
Management
Although ALHE is a benign condition, lesions are often difficult to eliminate and recurrence is common with a tendency for significant local cutaneous growth.4,9 Surgical treatment is the standard treatment, although recurrence occurs in up to one third of cases.8,16 Other possible treatment modalities such as intralesional corticosteroids, imiquimod, tacrolimus, photodynamic therapy, pulsed dye laser therapy and Mohs micrographic surgery16-20 have been used. Records obtained of our patient’s biopsied lesion one year ago from the same retroauricular site revealed ALHE as well. Our patient will be monitored and treated for any recurrence of ALHE.
Summary
ALHE is a benign vascular proliferation of unknown pathogenesis with histologically distinct endothelial cells and a mixed inflammatory infiltrate composed of mainly lymphocytes and eosinophils. It commonly occurs on the head and neck and has a tendency to recur after excision.
Drs. Hui and Khachemoune are with the Department of Dermatology, State University of New York Downstate Medical Center, and Veterans Affairs Medical Center, Brooklyn, NY.
Disclosure: The authors have no conflicts of interest to disclose.
Patient Presentation

 A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Angiolymphoid Hyperplasia With Eosinophilia (ALHE)
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an uncommon, benign vascular proliferation characterized by the presence of histologically distinct endothelial cells forming vessels. ALHE was first described by Wells and Whimster in 1969 as a late stage of Kimura’s disease and was later determined to be a histologically distinct entity.1,2 ALHE occurs most frequently in young to middle-age adults with a predilection for females,3 although it can occur in children and the elderly.
ALHE typically presents as multiple pink to reddish brown smooth-topped, dome-shaped papules or nodules on the head and neck, especially on the scalp and periauricular region.4 Rarely, lesions have been described in the mouth, trunk, extremities, genitals, muscle and bone.5-8 The papules may be isolated or grouped or may occur as plaques. Individual lesions seldom exceed
2 cm to 3 cm.9 A history of trauma to the area has been suggested as an inciting factor. Symptoms of ALHE lesions include pain, pruritus, pulsatile quality and bleeding after minor trauma.10 Regional lymph node enlargement and peripheral eosinophilia may be present in up to 20% of cases.3
Differential Diagnosis
ALHE may appear clinically similar to a variety of malignant and benign tumors. Most commonly, ALHE may be confused with Kaposi’s sarcoma, angiosarcoma, lymphoma cutis or vascularized metastases. Other conditions that may mimic ALHE include hemangiomas, pyogenic granulomas and sarcoidosis.
Histopathology
 Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
The vascular component of ALHE contains vessels of varying sizes, lined by plump endothelial cells that may project into the lumen, creating a distinct hobnailed appearance. These hobnailed endothelial cells contain a large nucleus with abundant eosinophilic cytoplasm and are characteristic of ALHE. Cytoplasmic vacuoles are seen in some cells, and may represent primitive vascular lumen. A muscular artery is often present at the center of the lesion.11 The thick walls of the larger vessels may demonstrate prominent myxoid degeneration. Mitotic figures may sometimes be present.
 Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
The pathophysiology of ALHE is still largely unknown. There is often mural damage or rupture in the large vessels of ALHE, which may suggest trauma or arteriovenous shunting as a mode of pathogenesis.8 Others have suggested that ALHE represents an abnormal vascular hypersensitivity reaction due to dysregulated expression of vasculogenic factors occurring from trauma or vascular malformations.13,14
Dermatoscopy
Dermatoscopy for the diagnosis of pigmented lesions is commonly employed, but its utility in identifying vascular lesions has yet to be determined.15 To our knowledge, we demonstrate the first report of the dermatoscopic features of ALHE. In our patient, the papules of ALHE demonstrate a diffuse reddish-brown erythema and whitish globules with fine vessels on the surface of the papules. The typical lacunae (red, blue, black) of hemangiomatous lesions were not appreciated. The reddish-brown erythema may represent the mixed inflammatory infiltrate overlying the vascular components of ALHE and the whitish globules may represent fibrotic stroma. Further dermatoscopic descriptions should be done to better delineate the features of ALHE and potentially aid in diagnosis.
Management
Although ALHE is a benign condition, lesions are often difficult to eliminate and recurrence is common with a tendency for significant local cutaneous growth.4,9 Surgical treatment is the standard treatment, although recurrence occurs in up to one third of cases.8,16 Other possible treatment modalities such as intralesional corticosteroids, imiquimod, tacrolimus, photodynamic therapy, pulsed dye laser therapy and Mohs micrographic surgery16-20 have been used. Records obtained of our patient’s biopsied lesion one year ago from the same retroauricular site revealed ALHE as well. Our patient will be monitored and treated for any recurrence of ALHE.
Summary
ALHE is a benign vascular proliferation of unknown pathogenesis with histologically distinct endothelial cells and a mixed inflammatory infiltrate composed of mainly lymphocytes and eosinophils. It commonly occurs on the head and neck and has a tendency to recur after excision.
Drs. Hui and Khachemoune are with the Department of Dermatology, State University of New York Downstate Medical Center, and Veterans Affairs Medical Center, Brooklyn, NY.
Disclosure: The authors have no conflicts of interest to disclose.
Patient Presentation
A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Angiolymphoid Hyperplasia With Eosinophilia (ALHE)
Angiolymphoid hyperplasia with eosinophilia (ALHE) is an uncommon, benign vascular proliferation characterized by the presence of histologically distinct endothelial cells forming vessels. ALHE was first described by Wells and Whimster in 1969 as a late stage of Kimura’s disease and was later determined to be a histologically distinct entity.1,2 ALHE occurs most frequently in young to middle-age adults with a predilection for females,3 although it can occur in children and the elderly.
ALHE typically presents as multiple pink to reddish brown smooth-topped, dome-shaped papules or nodules on the head and neck, especially on the scalp and periauricular region.4 Rarely, lesions have been described in the mouth, trunk, extremities, genitals, muscle and bone.5-8 The papules may be isolated or grouped or may occur as plaques. Individual lesions seldom exceed
2 cm to 3 cm.9 A history of trauma to the area has been suggested as an inciting factor. Symptoms of ALHE lesions include pain, pruritus, pulsatile quality and bleeding after minor trauma.10 Regional lymph node enlargement and peripheral eosinophilia may be present in up to 20% of cases.3
Differential Diagnosis
ALHE may appear clinically similar to a variety of malignant and benign tumors. Most commonly, ALHE may be confused with Kaposi’s sarcoma, angiosarcoma, lymphoma cutis or vascularized metastases. Other conditions that may mimic ALHE include hemangiomas, pyogenic granulomas and sarcoidosis.
Histopathology
Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
The vascular component of ALHE contains vessels of varying sizes, lined by plump endothelial cells that may project into the lumen, creating a distinct hobnailed appearance. These hobnailed endothelial cells contain a large nucleus with abundant eosinophilic cytoplasm and are characteristic of ALHE. Cytoplasmic vacuoles are seen in some cells, and may represent primitive vascular lumen. A muscular artery is often present at the center of the lesion.11 The thick walls of the larger vessels may demonstrate prominent myxoid degeneration. Mitotic figures may sometimes be present.
Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
The pathophysiology of ALHE is still largely unknown. There is often mural damage or rupture in the large vessels of ALHE, which may suggest trauma or arteriovenous shunting as a mode of pathogenesis.8 Others have suggested that ALHE represents an abnormal vascular hypersensitivity reaction due to dysregulated expression of vasculogenic factors occurring from trauma or vascular malformations.13,14
Dermatoscopy
Dermatoscopy for the diagnosis of pigmented lesions is commonly employed, but its utility in identifying vascular lesions has yet to be determined.15 To our knowledge, we demonstrate the first report of the dermatoscopic features of ALHE. In our patient, the papules of ALHE demonstrate a diffuse reddish-brown erythema and whitish globules with fine vessels on the surface of the papules. The typical lacunae (red, blue, black) of hemangiomatous lesions were not appreciated. The reddish-brown erythema may represent the mixed inflammatory infiltrate overlying the vascular components of ALHE and the whitish globules may represent fibrotic stroma. Further dermatoscopic descriptions should be done to better delineate the features of ALHE and potentially aid in diagnosis.
Management
Although ALHE is a benign condition, lesions are often difficult to eliminate and recurrence is common with a tendency for significant local cutaneous growth.4,9 Surgical treatment is the standard treatment, although recurrence occurs in up to one third of cases.8,16 Other possible treatment modalities such as intralesional corticosteroids, imiquimod, tacrolimus, photodynamic therapy, pulsed dye laser therapy and Mohs micrographic surgery16-20 have been used. Records obtained of our patient’s biopsied lesion one year ago from the same retroauricular site revealed ALHE as well. Our patient will be monitored and treated for any recurrence of ALHE.
Summary
ALHE is a benign vascular proliferation of unknown pathogenesis with histologically distinct endothelial cells and a mixed inflammatory infiltrate composed of mainly lymphocytes and eosinophils. It commonly occurs on the head and neck and has a tendency to recur after excision.
Drs. Hui and Khachemoune are with the Department of Dermatology, State University of New York Downstate Medical Center, and Veterans Affairs Medical Center, Brooklyn, NY.
Disclosure: The authors have no conflicts of interest to disclose.






 A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed.
A 92-year-old white male presented to the dermatology clinic with two pink shiny growths on his retroauricular scalp that had been growing slowly for several months. The lesions were occasionally tender and sometimes bled following minor trauma. The patient stated that he had a similar lesion in the same area, which had been biopsied one year prior. He did not recall the diagnosis. He denied any personal or family history of skin cancer. Examination revealed two erythematous, shiny, mildly firm 0.5-cm and 0.4-cm papules overlying a subcutaneous plaque, located on the right retroauricular scalp (Figure 1, left). Dermatoscopic examination was performed (Figure 2, right). An excision was performed. Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic.
Lesions of ALHE appear as circumscribed proliferations of vessels with perivascular inflammation within the dermis and subcutis (Figure 3). The inflammatory infiltrate consists of lymphocytes and eosinophils. Mast cells and plasma cells may also be present. Nodular lymphoid aggregates with and without germinal centers are occasionally found. The stroma may be myxoid or fibrotic. Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12
Histologically and historically, the presence of hobnailed endothelial cells represents a group of vascular tumors with a staining profile demonstrating endothelial cells of lymphatic origin (Table 1). The epithelioid cells of ALHE share characteristic features of epithelial cells, including ultrastructural Weibel-Palade bodies, storage granules that help regulate hemostasis and inflammation.8 AHLE cells also stain positively for epithelial cell markers such as CD31, CD34, factor VIII-related antigen and Ulex europaeus, but not for cytokeratins or epithelial membrane antigen. ALHE also stains positively for D2-40, which suggests ALHE could derive from lymphatic endothelium.12 ALHE does not stain for HHV-8.12







