



 Histologic examination characteristically reveals epithelioid cells in sheets or linear array diffusely in the dermis and subcutis without affecting the epidermis.1-9 The cells are often large and polygonal with pale cytoplasm and often a histiocytoid variant is described. The infiltrating cells display monomorphic, round, slightly pleomorphic nuclei.
Histologic examination characteristically reveals epithelioid cells in sheets or linear array diffusely in the dermis and subcutis without affecting the epidermis.1-9 The cells are often large and polygonal with pale cytoplasm and often a histiocytoid variant is described. The infiltrating cells display monomorphic, round, slightly pleomorphic nuclei. 
Figures 1 and 2. Physical examination revealed extensive firm dermal nodules scattered diffusely and coalescing into larger plaques on the chest, upper back, lateral neck, cheeks, ears and periocularly.
A 65-year-old cachectic gentleman presented to our clinic with a 12-month history of multiple non-tender progressive nodules. The nodules were slightly pruritic, but otherwise asymptomatic. His past medical and surgical history was positive for a surgical removal of growths on the right upper and lower eyelids.
Review of systems was positive for an unintentional 50 lb weight loss over the past year as well as extreme fatigue and weakness. Physical examination revealed extensive firm dermal nodules scattered diffusely and coalescing into larger plaques on the chest, upper back, lateral neck, cheeks, ears and periocularly (Figure 1). Lymph nodes were difficult to palpate due to the density of the cutaneous nodules.
What is Your Diagnosis?
See below for an answer and for more details.
Diagnosis: Primary Signet-ring Cell Carcinoma of the Eyelid with Cutaneous Metastases
Primary signet-ring cell carcinoma (PSCE) of the eyelid is a rare, primary cutaneous adenocarcinoma. The cell of origin is debatable, but is of either eccrine or apocrine origin.1,2 The first case was described by Rosen et al in 1975.3 Currently, there are less than 40 reported cases occurring either on the eyelid or more rarely in the axilla of elderly gentlemen.4
Etiology
PSCE is an adnexal neoplasm. However, the exact origin of PSCE is controversial as morphological and immunohistochemical features suggest both eccrine and apocrine differentiation.2,5,6 While cases involving the eye are more common, it has been reported to arise in the axillae where apoeccrine glands have been described. Apoeccrine glands are absent from the eyelids.2 Specific markers to separate the exact origin are lacking, and thus most authors conclude that it is impossible to distinguish apocrine from eccrine origin.2
Clinical Presentation
Patients present clinically with a characteristic swelling of the upper and lower eyelids, often with a ptosis. The initial lesion is fairly subtle, with slight erythema and swelling of the eyelid. The swelling and erythema from tumor infiltration in both the upper and lower eyelid creates the so-called “monocle-like” appearance.2 Occurrence in the axilla has been rarely described.4
Histopathology
 Histologic examination characteristically reveals epithelioid cells in sheets or linear array diffusely in the dermis and subcutis without affecting the epidermis.1-9 The cells are often large and polygonal with pale cytoplasm and often a histiocytoid variant is described. The infiltrating cells display monomorphic, round, slightly pleomorphic nuclei.
Histologic examination characteristically reveals epithelioid cells in sheets or linear array diffusely in the dermis and subcutis without affecting the epidermis.1-9 The cells are often large and polygonal with pale cytoplasm and often a histiocytoid variant is described. The infiltrating cells display monomorphic, round, slightly pleomorphic nuclei.
The tumor is further characterized by a variable number of cells showing eccentric nuclei, a vacuolated or signet-ring cell morphology.2,5 Often the tumor displays a linear or Indian-filing pattern that can dissect through skeletal muscle; and thus, clear surgical margins are difficult to achieve. PSCE is a diagnosis of exclusion and immunohistochemistry may aid in diagnosis.5,6,9 Tumor cells exhibit positivity for low molecular weight keratins, CEA, Ber-EP4, EMA, gross cystic disease fluid protein-15 and lysozymes and are negative for CK20, TTF-1, S-100, mucin, CDX-2, vimentin, RCC, PSA, HAS and CA19-9.2,5,6
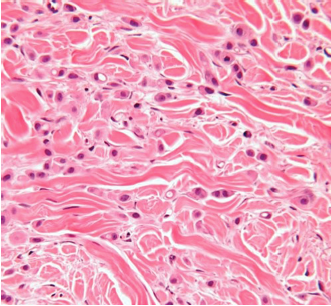
Figure 3. Hematoxylin and eosin 100x demonstrating epithelioid cells with rare signet-ring morphology.
Differential Diagnosis
Extensive work-up to exclude underlying visceral adenocarcinoma from the breast, gastrointestinal and genitourinary tract is necessary.5
Treatment
Exenteration of the orbit is recommended for orbital invasion and extensive involvement of the ocular adnexa and regional lymphadenectomy.5,9 Radiation and chemotherapy may be indicated in cases with extensive invasion. Despite surgical excision, the neoplasm often persists, extending to the surgical margins and often with involvement of the adjacent eyelid.3,5,9
Moreover, involvement of the adjacent orbit and distant metastases are not uncommon.5,9 The development of metastases to regional lymph nodes suggests an aggressive biologic behavior of the carcinoma.5,9 Only 3 reported cases of cutaneous metastases are reported in the English literature. However, none reported metastases as extensive as the present case5,7,8 (Figures 1 and 2).
Our Patient
His past medical history was significant for a poorly differentiated invasive, adenocarcinoma of the right upper and lower eyelids, which were incompletely excised in 2009. A chart review revealed he initially presented to the ophthalmology clinic with the chief complaint of swelling in the right lower eyelid and was noted on physical examination to have a lid ptosis of the ipsilateral upper eyelid. A biopsy was performed and histologic examination revealed an aggressive adenocarcinoma.
An extensive work-up ensued to uncover a possible primary source of the carcinoma, however, none was discovered. Therefore, a diagnosis of primary cutaneous adenocarcinoma was rendered. Treatment in 2009 included multiple surgical excisions by the plastic surgery department, with continued positive margins. Lymph node dissection of the ipsilateral cervical lymph nodes were positive for disease. Due to margin positivity, exenteration followed by radiation therapy was recommended. The patient refused further surgery or treatment and discontinued care.
Upon presentation to the dermatology clinic in 2013, a biopsy of the dermal nodules of the chest revealed tumor cells that appeared morphologically similar to the original periocular tumor. The biopsy was positive for pan keratin, CAM 5.2 and CK7 and negative for CK20.
The original histologic report of the right periorbital lesion demonstrated a diffuse infiltration of the entire dermis and subcutis by epithelioid cells in sheets, nests and linear arrays embedded in a desmoplastic stroma (Figure 3). The tumor cells had abundant eosinophilic cytoplasm. Intracytoplasmic vacuoles were noted in some of the tumor cells.
Mucicarmine stain was positive. Immunoperoxidase staining showed a positive reaction for CEA and CK7 and a negative reaction for CK20, TTF-1, S-100, mucin, CDX-2, vimentin, RCC, PSA, HAS, CA19-9 and thyroglobulin. The case presentation, along with histologic and immunohistochemistry review, and failure to identify visceral malignancy, supports a diagnosis most consistent with PSCE of the eyelid with subsequent cutaneous metastases. A chest x-ray revealed bilateral metastatic disease in the bones and soft tissues. Our patient expired shortly after presentation to our clinic.
Conclusion
PSCE of the eyelid is a rare, primary cutaneous adenocarcinoma with less than 40 cases reported in the literature. It is a diagnosis of exclusion, as metastatic adenocarcinoma of the breast, lung, gastrointestinal and genitourinary tract must be excluded. PSCE can present subtly but is an aggressive tumor, often extending to the margins of excisions. Histologic examination reveals sheets of epithelioid cells in the dermis with rare signet-ring cell morphology. Exenteration of the orbit is the treatment of choice followed by radiation therapy. While metastatic disease has been reported in the literature, there are no cases that match the extent of metastatic disease that our patient subsequently developed.
It is an important diagnostic consideration in patients presenting with eyelid swelling and ptosis and therefore substantiates aggressive treatment, as highlighted by our case presentation. Thus, the importance of a multidisciplinary approach to patient care, and risk of poor outcome if exenteration of the orbit followed by radiation therapy is not pursued is emphasized.
Dr. Walls, PGY4, is a dermatology resident at Nova Southeastern University College of Osteopathic Medicine in Largo, FL.
Dr. Hogan is with the dermatology department at CW Bill Young Department of Veteran Affairs Medical Center in St Petersburg, FL.
Dr. Heaphy is with Gulf Coast Dermatopathology Laboratory, Inc. in Tampa, FL.
Disclosure: The authors report no relevant financial relationships.
Acknowledgement: The authors thank Dr. Zitman, MD, at CW Bill Young VA for helping to obtain prior biopsy slides for review and for his review of the pathology slides with the authors.
References
1. Jakobiec FA, Austin P, Iwamoto T, Trokel SL, Marquardt MD, Harrison W. Primary infiltrating signet ring carcinoma of the eyelid. Ophthalmol. 1983;90(3):291-299.
2. Mortensen AL, Heegaard S, Clemmensen O, Prause JU. Signet ring cell carcinoma of the eyelid – the monocle tumor. APMIS. 2008;116(4):326-332.
3. Rosen Y, Kim B, Yermakov VA. Eccrine sweat gland tumor of clear cell origin involving the eyelids. Cancer. 1975;36(3):1034-1041.
4. Hansen MS, Chi SL, Cummings T, Woodward J. Uncorrectable ptosis: primary cutaneous signet-ring cell carcinoma. Dermatol Online J. 2013;19(9):19615.
5. Requena L, Prieto VG, Requena C, et al. Primary signet-ring cell/histiocytoid carcinoma of the eyelid: a clinicopathologic study of 5 cases and review of the literature. Am J Surg Patholol. 2011;35(3):378-391.
6. Betis F. Hofman V, Lagier J, Gastaud P, Santini J, Hofman P. Primary signet ring cell carcinoma of the eccrine sweat gland in the eyelid. Immunohistochemical and ultrastructural study of a case. J Fr Ophtalmol. 2002;25(5):547-551.
7. Bellman B, Gregory NA, Silvers D, Foutain KS. Sweat gland carcinoma with metastases to the skin: response to 5-fluorouracil chemotherapy. Cutis. 1995;55(4):221-224.
8. Wollensak G, Witschel H, Böhm N. Signet ring cell carcinoma of the eccrine sweat glands in the eyelid. Ophthalmology. 1996;103(11):1788-1793.
9. Tanboon J, Uiprasertkul M, Luemsamran P. Signet-ring cell/histiocytoid carcinoma of the eyelid: a case report and review of the literature. Am J Dermatopathol. 2013;35(1):e1-e5.









