PATIENT PRESENTATION
 A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Digital Mucous Cyst
Benign growths form the majority of tumors of the hand. A digital mucous cyst is a common, benign cystic growth of the hand.1 They are often found on the dorsal aspect of the distal interphalangeal (DIP) joint, at the proximal nail fold and, rarely, under the nail matrix. They are filled with mucin and considered to result from focal degeneration of connective tissue and overproduction of hyaluronic acid.2
Epidemiology
Digital mucous cysts are seen among young adults and elderly people. They are 2-3 times more common in women than in men.
Clinical Presentation
Digital mucous cysts are usually clinically asymptomatic. Swelling can appear suddenly or over time. Patients may seek medical help after a recent increase in size or after trauma, which can cause pain.3 Pain can also result from an enlarging cyst and, depending on its location, nerve compression. Patients may complain of impaired joint movement or interference with function.4
Digital mucous cysts appear as round to oval, flesh-colored, dome-shaped papulonodules. They have a smooth and shiny surface. On palpation they can be firm to fluctuant with a cystic consistency and may show transillumination. They contain a viscous, gelatinous fluid, which may be clear or yellow-tinged. On the finger, they are frequently found on the dorsolateral aspect between the DIP and proximal nail fold. Less commonly, they can be found between the proximal nail fold and the nail plate or beneath the nail matrix. They may often cause grooving or pitting of the adjacent nail.
Differential Diagnosis
Digital mucous cysts may appear clinically similar to ganglion cysts and synovial cysts. Other entities in the differential diagnosis include Heberden’s nodes, tophi, herpetic whitlow, granuloma annulare, molluscum contagiosum, rheumatoid nodules, sarcoidosis and nodules associated with repetitive trauma.5
Histology
The digital mucous cyst is a pseudocyst. The wall of the cyst is formed by fibrous tissue and contains omorphous, often myxoid material. The cyst fluid is made up of hyaluronic acid, which is the predominate mucopolysaccharide within the cyst’s cavity.6
Management
The diagnosis of digital mucous cyst is usually clinical and straightforward. Regular X-rays may reveal non-specific soft tissue density with underlying arthritis in the adjacent joint and the presence of loose bodies in the joint. Ultrasound may demonstrate a rounded mass with a hypoechoic appearance and can be used for needle-guided aspiration of cysts in larger joints. On MRI, a homogenous mass can be seen with occasional intracystic septa, satellite cysts, cyst pedicles, osteoarthritis of joint, subungual cyst and many flattened cysts. Physicians may occasionally use it preoperatively.7
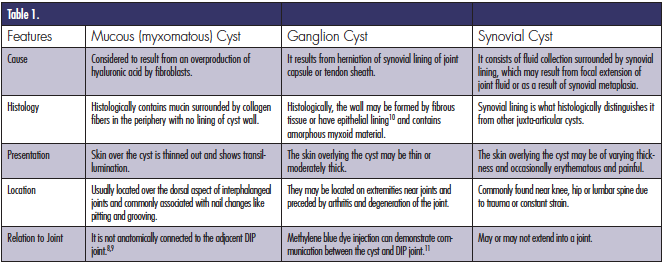
 The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
Some cysts resolve spontaneously and require only observation. Physicians may recommend aspiration and multiple perforations with a 25 gauge, but the recurrence and infection rates are quite high.12 Aspiration of the cyst can be followed by injection with cortisone or hyaluronic acid.13,14 These techniques may result in skin hypopigmentation, subcutaneous fat necrosis, injury to adjacent structures and recurrence.
Cryosurgery with liquid nitrogen can be used to unroof the cyst and drain it. Cure rate is said to be around 85% after a single treatment. Complications may include proximal nail fold notching.
Surgical excision with an open or orthoscopic procedure can be indicated in cases with pain, functional disability, cosmetic disfigurement and recurrence of cyst.14-17 Excision is done with local infiltration of anesthetics or with a local digital nerve block. Complications are rare but may include neurovascular injury, recurrence and scarring.
Our Patient
The cyst was excised and sent for histopathology. The pathology revealed cup-shaped invagination of the epidermis containing abundant myxonatous granular material with few scattered stellate cells. The mucinous contents were basophilic when stained with acid mucopolysaccharides with alcian blue stain, confirming digital mucous cyst. On a 2-week follow up visit, the patient was asymptomatic and no recurrence was noticed.
Conclusion
Digital mucous cysts are benign swellings most commonly found over the DIP. They are filled with mucin and are commonly asymptomatic. The most common presentation is due to disfigurement or rupture due to trauma. They can be aspirated but are most commonly excised to reduce the incidence of recurrence.
Dr. Mohamed is a research fellow at Saint Luke’s Roosevelt Hospital in New York, NY.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Angelides AC. Ganglions of the hand and wrist. In: Green DP, editor. Operative hand surgery, vol. 2. New York: Churchill Livingstone; 1993. p. 2171–83.
2. Steiner E, Steinbach LS, Schnarkowski P, Tirman PF, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am.1996;34(2):395-425.
3. Pope TL, Fechner RE, Keats TE. Intraosseous ganglion. Report of four cases and review of the literature. Skeletal Radiol.1989;18(3):185–187.
4. Schrank C, Meirer R, Stäbler A, Nerlich A, Reiser M, Putz R. Morphology and topography of intraosseous ganglion cysts in the carpus: An anatomic, histopathologic, and Magnetic Resonance Imaging correlation study. J Hand Surg. 2003;28(1):52–61.
5. Vasani SS, Demetriades AK, Joshi SM, Yeh J, Ellamushi H. Traumatic intraspinal extradural ganglion cyst in a teenager: Case report and review of the literature. Clin Neurol Neurosurg. 2007;109(1):88–91.
6. Soren A. Pathogenesis and treatment of ganglion. Clin Orthop Relat Res. Sep-Oct 1966;48:173-79.
7. Drape JL, Idy-Peretti I, Goettmann S, et al. MR imaging of digital mucoid cysts. Radiology. 1996;200(2):531-36.
8. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: the ganglion type. Int J Dermatol. 1999;38(7):533–535.
9. Salasche SJ. Myxoid cysts of the proximal nail fold: A surgical approach. J Dermatol Surg Oncol.1984;10(1):35–39.
10. Kivanc-Altunay I, Kumbasar E, Gokdemir G, Koslu A, Tekkesin M, Basak T. Unusual localization of multiple myxoid (mucous) cysts of toes. Dermatol Online J. 2004;10(1):23.
11. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: The ganglion type. Int J Dermatol. 1999;38(7):533–535.
12. Epstein E. A simple technique for managing digital mucous cysts. Arch Dermatol. 1979;115(11):1315-6.
13. Bureau NJ, Kaplan PA, Dussault RG. Lumbar facet joint synovial cyst: Percutaneous treatment with steroid injections and distention--clinical and imaging follow-up in 12 patients. Radiology. 2001;221(1):179–85.
14. Hsu KY, Zucherman JF, Shea WJ, Jeffrey RA. Lumbar intraspinal synovial and ganglion cysts (facet cysts). Ten-year experience in evaluation and treatment. Spine (Phila Pa 1976).1995;20(1):80–89.
15. Magee TH, Rowedder AM, Degnan GG. Intraosseous ganglia of the wrist. Radiology. 1995;195(2):517–520.
16. Bittner JG, Kang R, Stern PJ. Management of flexor tendon sheath ganglions: A cost analysis. J Hand Surg Am. 2002;27(4):586–90.
17. Hagen T, Daschner H, Lensch T. [Juxta-facet cysts: magnetic resonance tomography diagnosis]. Radiologe. 2001;41(12):1056–1062.
PATIENT PRESENTATION
 A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Digital Mucous Cyst
Benign growths form the majority of tumors of the hand. A digital mucous cyst is a common, benign cystic growth of the hand.1 They are often found on the dorsal aspect of the distal interphalangeal (DIP) joint, at the proximal nail fold and, rarely, under the nail matrix. They are filled with mucin and considered to result from focal degeneration of connective tissue and overproduction of hyaluronic acid.2
Epidemiology
Digital mucous cysts are seen among young adults and elderly people. They are 2-3 times more common in women than in men.
Clinical Presentation
Digital mucous cysts are usually clinically asymptomatic. Swelling can appear suddenly or over time. Patients may seek medical help after a recent increase in size or after trauma, which can cause pain.3 Pain can also result from an enlarging cyst and, depending on its location, nerve compression. Patients may complain of impaired joint movement or interference with function.4
Digital mucous cysts appear as round to oval, flesh-colored, dome-shaped papulonodules. They have a smooth and shiny surface. On palpation they can be firm to fluctuant with a cystic consistency and may show transillumination. They contain a viscous, gelatinous fluid, which may be clear or yellow-tinged. On the finger, they are frequently found on the dorsolateral aspect between the DIP and proximal nail fold. Less commonly, they can be found between the proximal nail fold and the nail plate or beneath the nail matrix. They may often cause grooving or pitting of the adjacent nail.
Differential Diagnosis
Digital mucous cysts may appear clinically similar to ganglion cysts and synovial cysts. Other entities in the differential diagnosis include Heberden’s nodes, tophi, herpetic whitlow, granuloma annulare, molluscum contagiosum, rheumatoid nodules, sarcoidosis and nodules associated with repetitive trauma.5
Histology
The digital mucous cyst is a pseudocyst. The wall of the cyst is formed by fibrous tissue and contains omorphous, often myxoid material. The cyst fluid is made up of hyaluronic acid, which is the predominate mucopolysaccharide within the cyst’s cavity.6
Management
The diagnosis of digital mucous cyst is usually clinical and straightforward. Regular X-rays may reveal non-specific soft tissue density with underlying arthritis in the adjacent joint and the presence of loose bodies in the joint. Ultrasound may demonstrate a rounded mass with a hypoechoic appearance and can be used for needle-guided aspiration of cysts in larger joints. On MRI, a homogenous mass can be seen with occasional intracystic septa, satellite cysts, cyst pedicles, osteoarthritis of joint, subungual cyst and many flattened cysts. Physicians may occasionally use it preoperatively.7
 The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
Some cysts resolve spontaneously and require only observation. Physicians may recommend aspiration and multiple perforations with a 25 gauge, but the recurrence and infection rates are quite high.12 Aspiration of the cyst can be followed by injection with cortisone or hyaluronic acid.13,14 These techniques may result in skin hypopigmentation, subcutaneous fat necrosis, injury to adjacent structures and recurrence.
Cryosurgery with liquid nitrogen can be used to unroof the cyst and drain it. Cure rate is said to be around 85% after a single treatment. Complications may include proximal nail fold notching.
Surgical excision with an open or orthoscopic procedure can be indicated in cases with pain, functional disability, cosmetic disfigurement and recurrence of cyst.14-17 Excision is done with local infiltration of anesthetics or with a local digital nerve block. Complications are rare but may include neurovascular injury, recurrence and scarring.
Our Patient
The cyst was excised and sent for histopathology. The pathology revealed cup-shaped invagination of the epidermis containing abundant myxonatous granular material with few scattered stellate cells. The mucinous contents were basophilic when stained with acid mucopolysaccharides with alcian blue stain, confirming digital mucous cyst. On a 2-week follow up visit, the patient was asymptomatic and no recurrence was noticed.
Conclusion
Digital mucous cysts are benign swellings most commonly found over the DIP. They are filled with mucin and are commonly asymptomatic. The most common presentation is due to disfigurement or rupture due to trauma. They can be aspirated but are most commonly excised to reduce the incidence of recurrence.
Dr. Mohamed is a research fellow at Saint Luke’s Roosevelt Hospital in New York, NY.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Angelides AC. Ganglions of the hand and wrist. In: Green DP, editor. Operative hand surgery, vol. 2. New York: Churchill Livingstone; 1993. p. 2171–83.
2. Steiner E, Steinbach LS, Schnarkowski P, Tirman PF, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am.1996;34(2):395-425.
3. Pope TL, Fechner RE, Keats TE. Intraosseous ganglion. Report of four cases and review of the literature. Skeletal Radiol.1989;18(3):185–187.
4. Schrank C, Meirer R, Stäbler A, Nerlich A, Reiser M, Putz R. Morphology and topography of intraosseous ganglion cysts in the carpus: An anatomic, histopathologic, and Magnetic Resonance Imaging correlation study. J Hand Surg. 2003;28(1):52–61.
5. Vasani SS, Demetriades AK, Joshi SM, Yeh J, Ellamushi H. Traumatic intraspinal extradural ganglion cyst in a teenager: Case report and review of the literature. Clin Neurol Neurosurg. 2007;109(1):88–91.
6. Soren A. Pathogenesis and treatment of ganglion. Clin Orthop Relat Res. Sep-Oct 1966;48:173-79.
7. Drape JL, Idy-Peretti I, Goettmann S, et al. MR imaging of digital mucoid cysts. Radiology. 1996;200(2):531-36.
8. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: the ganglion type. Int J Dermatol. 1999;38(7):533–535.
9. Salasche SJ. Myxoid cysts of the proximal nail fold: A surgical approach. J Dermatol Surg Oncol.1984;10(1):35–39.
10. Kivanc-Altunay I, Kumbasar E, Gokdemir G, Koslu A, Tekkesin M, Basak T. Unusual localization of multiple myxoid (mucous) cysts of toes. Dermatol Online J. 2004;10(1):23.
11. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: The ganglion type. Int J Dermatol. 1999;38(7):533–535.
12. Epstein E. A simple technique for managing digital mucous cysts. Arch Dermatol. 1979;115(11):1315-6.
13. Bureau NJ, Kaplan PA, Dussault RG. Lumbar facet joint synovial cyst: Percutaneous treatment with steroid injections and distention--clinical and imaging follow-up in 12 patients. Radiology. 2001;221(1):179–85.
14. Hsu KY, Zucherman JF, Shea WJ, Jeffrey RA. Lumbar intraspinal synovial and ganglion cysts (facet cysts). Ten-year experience in evaluation and treatment. Spine (Phila Pa 1976).1995;20(1):80–89.
15. Magee TH, Rowedder AM, Degnan GG. Intraosseous ganglia of the wrist. Radiology. 1995;195(2):517–520.
16. Bittner JG, Kang R, Stern PJ. Management of flexor tendon sheath ganglions: A cost analysis. J Hand Surg Am. 2002;27(4):586–90.
17. Hagen T, Daschner H, Lensch T. [Juxta-facet cysts: magnetic resonance tomography diagnosis]. Radiologe. 2001;41(12):1056–1062.
PATIENT PRESENTATION
A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Digital Mucous Cyst
Benign growths form the majority of tumors of the hand. A digital mucous cyst is a common, benign cystic growth of the hand.1 They are often found on the dorsal aspect of the distal interphalangeal (DIP) joint, at the proximal nail fold and, rarely, under the nail matrix. They are filled with mucin and considered to result from focal degeneration of connective tissue and overproduction of hyaluronic acid.2
Epidemiology
Digital mucous cysts are seen among young adults and elderly people. They are 2-3 times more common in women than in men.
Clinical Presentation
Digital mucous cysts are usually clinically asymptomatic. Swelling can appear suddenly or over time. Patients may seek medical help after a recent increase in size or after trauma, which can cause pain.3 Pain can also result from an enlarging cyst and, depending on its location, nerve compression. Patients may complain of impaired joint movement or interference with function.4
Digital mucous cysts appear as round to oval, flesh-colored, dome-shaped papulonodules. They have a smooth and shiny surface. On palpation they can be firm to fluctuant with a cystic consistency and may show transillumination. They contain a viscous, gelatinous fluid, which may be clear or yellow-tinged. On the finger, they are frequently found on the dorsolateral aspect between the DIP and proximal nail fold. Less commonly, they can be found between the proximal nail fold and the nail plate or beneath the nail matrix. They may often cause grooving or pitting of the adjacent nail.
Differential Diagnosis
Digital mucous cysts may appear clinically similar to ganglion cysts and synovial cysts. Other entities in the differential diagnosis include Heberden’s nodes, tophi, herpetic whitlow, granuloma annulare, molluscum contagiosum, rheumatoid nodules, sarcoidosis and nodules associated with repetitive trauma.5
Histology
The digital mucous cyst is a pseudocyst. The wall of the cyst is formed by fibrous tissue and contains omorphous, often myxoid material. The cyst fluid is made up of hyaluronic acid, which is the predominate mucopolysaccharide within the cyst’s cavity.6
Management
The diagnosis of digital mucous cyst is usually clinical and straightforward. Regular X-rays may reveal non-specific soft tissue density with underlying arthritis in the adjacent joint and the presence of loose bodies in the joint. Ultrasound may demonstrate a rounded mass with a hypoechoic appearance and can be used for needle-guided aspiration of cysts in larger joints. On MRI, a homogenous mass can be seen with occasional intracystic septa, satellite cysts, cyst pedicles, osteoarthritis of joint, subungual cyst and many flattened cysts. Physicians may occasionally use it preoperatively.7
The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
Some cysts resolve spontaneously and require only observation. Physicians may recommend aspiration and multiple perforations with a 25 gauge, but the recurrence and infection rates are quite high.12 Aspiration of the cyst can be followed by injection with cortisone or hyaluronic acid.13,14 These techniques may result in skin hypopigmentation, subcutaneous fat necrosis, injury to adjacent structures and recurrence.
Cryosurgery with liquid nitrogen can be used to unroof the cyst and drain it. Cure rate is said to be around 85% after a single treatment. Complications may include proximal nail fold notching.
Surgical excision with an open or orthoscopic procedure can be indicated in cases with pain, functional disability, cosmetic disfigurement and recurrence of cyst.14-17 Excision is done with local infiltration of anesthetics or with a local digital nerve block. Complications are rare but may include neurovascular injury, recurrence and scarring.
Our Patient
The cyst was excised and sent for histopathology. The pathology revealed cup-shaped invagination of the epidermis containing abundant myxonatous granular material with few scattered stellate cells. The mucinous contents were basophilic when stained with acid mucopolysaccharides with alcian blue stain, confirming digital mucous cyst. On a 2-week follow up visit, the patient was asymptomatic and no recurrence was noticed.
Conclusion
Digital mucous cysts are benign swellings most commonly found over the DIP. They are filled with mucin and are commonly asymptomatic. The most common presentation is due to disfigurement or rupture due to trauma. They can be aspirated but are most commonly excised to reduce the incidence of recurrence.
Dr. Mohamed is a research fellow at Saint Luke’s Roosevelt Hospital in New York, NY.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Angelides AC. Ganglions of the hand and wrist. In: Green DP, editor. Operative hand surgery, vol. 2. New York: Churchill Livingstone; 1993. p. 2171–83.
2. Steiner E, Steinbach LS, Schnarkowski P, Tirman PF, Genant HK. Ganglia and cysts around joints. Radiol Clin North Am.1996;34(2):395-425.
3. Pope TL, Fechner RE, Keats TE. Intraosseous ganglion. Report of four cases and review of the literature. Skeletal Radiol.1989;18(3):185–187.
4. Schrank C, Meirer R, Stäbler A, Nerlich A, Reiser M, Putz R. Morphology and topography of intraosseous ganglion cysts in the carpus: An anatomic, histopathologic, and Magnetic Resonance Imaging correlation study. J Hand Surg. 2003;28(1):52–61.
5. Vasani SS, Demetriades AK, Joshi SM, Yeh J, Ellamushi H. Traumatic intraspinal extradural ganglion cyst in a teenager: Case report and review of the literature. Clin Neurol Neurosurg. 2007;109(1):88–91.
6. Soren A. Pathogenesis and treatment of ganglion. Clin Orthop Relat Res. Sep-Oct 1966;48:173-79.
7. Drape JL, Idy-Peretti I, Goettmann S, et al. MR imaging of digital mucoid cysts. Radiology. 1996;200(2):531-36.
8. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: the ganglion type. Int J Dermatol. 1999;38(7):533–535.
9. Salasche SJ. Myxoid cysts of the proximal nail fold: A surgical approach. J Dermatol Surg Oncol.1984;10(1):35–39.
10. Kivanc-Altunay I, Kumbasar E, Gokdemir G, Koslu A, Tekkesin M, Basak T. Unusual localization of multiple myxoid (mucous) cysts of toes. Dermatol Online J. 2004;10(1):23.
11. Hernandez-Lugo AM, Dominguez-Cherit J, Vega-Memije ME. Digital mucoid cyst: The ganglion type. Int J Dermatol. 1999;38(7):533–535.
12. Epstein E. A simple technique for managing digital mucous cysts. Arch Dermatol. 1979;115(11):1315-6.
13. Bureau NJ, Kaplan PA, Dussault RG. Lumbar facet joint synovial cyst: Percutaneous treatment with steroid injections and distention--clinical and imaging follow-up in 12 patients. Radiology. 2001;221(1):179–85.
14. Hsu KY, Zucherman JF, Shea WJ, Jeffrey RA. Lumbar intraspinal synovial and ganglion cysts (facet cysts). Ten-year experience in evaluation and treatment. Spine (Phila Pa 1976).1995;20(1):80–89.
15. Magee TH, Rowedder AM, Degnan GG. Intraosseous ganglia of the wrist. Radiology. 1995;195(2):517–520.
16. Bittner JG, Kang R, Stern PJ. Management of flexor tendon sheath ganglions: A cost analysis. J Hand Surg Am. 2002;27(4):586–90.
17. Hagen T, Daschner H, Lensch T. [Juxta-facet cysts: magnetic resonance tomography diagnosis]. Radiologe. 2001;41(12):1056–1062.




 A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes.
A 49-year-old white female presented with the chief complaint of a small swelling lesion over her right index finger close to her nail. The lesion was present for 2 years and was mildly painful and occasionally accompanied by drainage of a white-yellowish material. The patient admitted that she had tried to drain out the contents by puncturing it. Surgical attempt by a practitioner at an urgent care center was also unsuccessful. On examination, a 6x6 mm slightly tender papule with a shiny lateral surface and fluctuant consistency and a small crust on the top was noted. The papule was overlying the distal intraphalangeal joint on the dorsal aspect of the right index finger. The adjacent nail showed no changes. The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11
The term digital mucous cyst has been interchangeably used along with ganglion cyst and synovial cyst. The subtle differences between these 3 similar-looking tumors are noted in Table 1.8-11






