The landscape of eczema research and treatment is vastly changing and potential new therapies are in development, according to Robert Sidbury, MD, MPH, associate professor, department of pediatrics, chief, division of dermatology, Seattle Children’s Hospital and University of Washington School of Medicine in Seattle, WA.
In 2000 there were only a handful of clinical trials for eczema and tacrolimus, pimecrolimus were poised for release. Now in 2015, 124 clinical trials are underway and potential new therapies are in development. The future appears promising with exciting new non-steroidal topical and systemic therapies in the pipeline, said Dr. Sidbury, who spoke on the topic at a session at the Summer 2015 American Academy of Dermatology meeting. He noted that much research has been done in the last few years and even the most recently published 2014 Atopic Dermatitis (AD) Guidelines,1-4 which were published in 4 parts, do not include this new research because the literature search used for the guidelines ended in 2012 and since 2013 more than 3,000 papers have been published.
New Treatment Pipeline
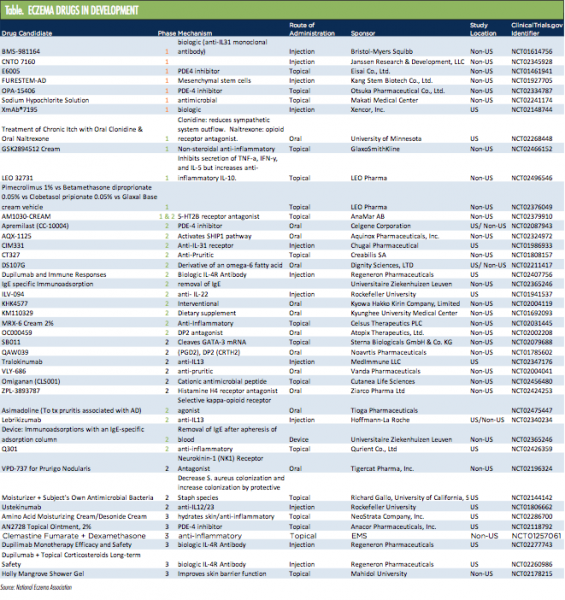
A Table from the National Eczema Association lists eczema and atopic dermatitis therapies that are in the development pipeline. The products range from Phase I to Phase III. “There’s a significant number of therapies in Phase III trials and these range from topicals to injections to orals, so they run the gamut and it is just an extraordinary list,” said Dr. Sidbury, who discussed numerous potential therapies, including AN2728 (now called Crisaborole Topical Ointment, 2%, Anacor Pharmaceuticals, Inc.), dupilumab (Sanofi/Regeneron Pharmaceuticals, Inc.) and tofacitinib (Xeljanz, Pfizer Inc.).
Dr. Sidbury noted that a practice gap exists in dermatology today with regard to eczema treatment. “Topical steroid fear is greatest in relation to younger children; however, most effective non-steroidal agents are not approved in younger children,” he said.
However, some possible alternatives are in the pipeline. Crisabarole, the AN2728-small molecule phosophodiesterase 4 (PDE-4) inhibitor with anti-inflammatory properties, is a boron-based small molecule (251 Da). Boron is essential for anti-inflammatory activity. The agent inhibits PDE-4 and reduces production of multiple inflammatory cytokines. Results from 2 Phase III, double-blind, vehicle-controlled studies were recently released. Each trial included 750 mild-to-moderate eczema patients (age 2-18 years old).
The primary study endpoint was clear or almost clear at day 29. In 1 trial, the results demonstrated that 32.8% in the Crisaborole arm and 25.4% in the vehicle arm reached the primary endpoint. The other trial has similar results, he said.
“Crisaborole was faster and more effective than the vehicle (statistically significant) and it was well-tolerated. There were some application site reactions but not dramatic numbers, and no serious side effects occurred,” he said.
At the time that the 2014 Atopic Dermatitis Guidelines1-4 were completed, 4 systemic therapy agents had been shown in the literature to be safe and effective in the treatment of severe AD: cyclosporine, mycophenolate, methotrexate and azathioprine. “I tend to use cyclosporine the most, but mainly because it works quicker, not because it is necessarily any better. There is a study that showed that mycophenolate doesn’t work as quickly, but it actually maybe has a more sustained benefit than cyclosporine. So I tend to try and induce remission with cyclosporine and then transition to one of the other drugs,” Dr. Sidbury said, noting dermatologists have their own preferences on which to use.
Several biologics are now being investigated for treatment of AD. They include interleukin (IL)-31 receptor (CIM331, Chugai Pharmaceutical), IL-22 (ILV-094, Rockefeller University), IL-13 (tralokinumab, MedImmune LLC), IL-12/IL-23 (ustekinumab, Rockefeller University) and IL-4 receptor dupilumab. Only once-weekly injection dupilumab is in Phase III.
Beck et al5 reported on blinded trials in adults with moderate-to-severe AD. “The trials both looked at biomarkers but also easy scales with really nice drops in the Eczema Area and Severity Index scores, really nice drops in the Investigator’s Global Assessment scores and beautiful drops in the itch scores,” he said, adding that anecdotal reports from adult study participants has been very positive.
Dupilumab seems as effective if not more and safer than more current systemic options, Dr. Sidbury said. “It may affect staph attachment in addition to treating specific AD inflammatory state. However, injection is not ideal for some, including most children,” he said.
 Other Therapies
Other Therapies
Other therapies, deeper in the pipeline that pose possibilities for eczema treatment include Janus kinase (JAK) inhibitors. The JAK inhibitor tofacitinib is FDA approved for the treatment of adult patients with moderately to severely active rheumatoid arthritis who had an inadequate response or intolerance to methotrexate and carries a black box warning. It is also used in hematology/oncology to treat refractory solid tumors and myelofibrosis, he explained.
Levy et al6 demonstrated that the oral JAK inhibitor tofacitinib citrate may be beneficial in the treatment of moderate-to-severe AD. The small study, evaluated 6 consecutive patients with moderate-to-severe AD who had failed standard treatment and were treated with tofacitinib citrate. Response to treatment was assessed using the Scoring of AD index. Decreased body suface area involvement of dermatitis and decreased erythema, edema/papulation, lichenification and excoriation were observed in all patients. The Scoring of AD index decreased by 66.6% from 36.5 to 12.2 (P<.05) during 8 to 29 weeks of treatment. There were no adverse events. Limitations of the study included the small sample size, lack of placebo control group and the possibility of bias.
Another JAK inhibitor, oclacitinib7,8 (Apoquel, Zoetis) is used to treat AD in dogs and seems to be a very effective treatment, he added.
These exciting new non-steroidal topical and systemic therapies in pipeline pose great potential for the treatment of eczema and atopic dermatitis, he concluded. “Julie Block, the head of the National Eczema Association, calls this the decade of eczema, and I think there’s a lot to that right now,” he said.
Disclosure: Dr. Sidbury was a site investigator in Anacor’s Phase III trial of a non-steroidal topical product for atopic dermatitis.
References
1. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351.
2. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116-132.
3. Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327-349.
4. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjunctive therapies and approaches.
J Am Acad Dermatol. 2014;71(6):1218-1233.
5. Beck LA, Thaçi D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Eng J Med. 2014; 371(2):130-139.
6. Levy LL, Urban J, King BA. Treatment of recalcitrant atopic dermatitis with the oral Janus kinase inhibitor tofacitinib citrate. J Am Acad Dermatol. 2015;73(3):395-399.
7. Cosgrove SB, Cleaver DM, King VL, et al. Long-term compassionate use of oclacitinib in dogs with atopic and allergic skin disease: safety, efficacy and quality of life. Vet Dermatol. 2015;26(3):171-179, e35.
8. Fukuyama T, Ehling S, Cook E, Bäumer W. Topically administered Janus-kinase inhibitors tofacitinib and oclacitinib display impressive antipruritic and anti-inflammatory responses in a model of allergic dermatitis. J Pharmacol Exp Ther. 2015;354(3):394-405.
The landscape of eczema research and treatment is vastly changing and potential new therapies are in development, according to Robert Sidbury, MD, MPH, associate professor, department of pediatrics, chief, division of dermatology, Seattle Children’s Hospital and University of Washington School of Medicine in Seattle, WA.
In 2000 there were only a handful of clinical trials for eczema and tacrolimus, pimecrolimus were poised for release. Now in 2015, 124 clinical trials are underway and potential new therapies are in development. The future appears promising with exciting new non-steroidal topical and systemic therapies in the pipeline, said Dr. Sidbury, who spoke on the topic at a session at the Summer 2015 American Academy of Dermatology meeting. He noted that much research has been done in the last few years and even the most recently published 2014 Atopic Dermatitis (AD) Guidelines,1-4 which were published in 4 parts, do not include this new research because the literature search used for the guidelines ended in 2012 and since 2013 more than 3,000 papers have been published.

New Treatment Pipeline
A Table from the National Eczema Association lists eczema and atopic dermatitis therapies that are in the development pipeline. The products range from Phase I to Phase III. “There’s a significant number of therapies in Phase III trials and these range from topicals to injections to orals, so they run the gamut and it is just an extraordinary list,” said Dr. Sidbury, who discussed numerous potential therapies, including AN2728 (now called Crisaborole Topical Ointment, 2%, Anacor Pharmaceuticals, Inc.), dupilumab (Sanofi/Regeneron Pharmaceuticals, Inc.) and tofacitinib (Xeljanz, Pfizer Inc.).
Dr. Sidbury noted that a practice gap exists in dermatology today with regard to eczema treatment. “Topical steroid fear is greatest in relation to younger children; however, most effective non-steroidal agents are not approved in younger children,” he said.
However, some possible alternatives are in the pipeline. Crisabarole, the AN2728-small molecule phosophodiesterase 4 (PDE-4) inhibitor with anti-inflammatory properties, is a boron-based small molecule (251 Da). Boron is essential for anti-inflammatory activity. The agent inhibits PDE-4 and reduces production of multiple inflammatory cytokines. Results from 2 Phase III, double-blind, vehicle-controlled studies were recently released. Each trial included 750 mild-to-moderate eczema patients (age 2-18 years old).
The primary study endpoint was clear or almost clear at day 29. In 1 trial, the results demonstrated that 32.8% in the Crisaborole arm and 25.4% in the vehicle arm reached the primary endpoint. The other trial has similar results, he said.
“Crisaborole was faster and more effective than the vehicle (statistically significant) and it was well-tolerated. There were some application site reactions but not dramatic numbers, and no serious side effects occurred,” he said.
At the time that the 2014 Atopic Dermatitis Guidelines1-4 were completed, 4 systemic therapy agents had been shown in the literature to be safe and effective in the treatment of severe AD: cyclosporine, mycophenolate, methotrexate and azathioprine. “I tend to use cyclosporine the most, but mainly because it works quicker, not because it is necessarily any better. There is a study that showed that mycophenolate doesn’t work as quickly, but it actually maybe has a more sustained benefit than cyclosporine. So I tend to try and induce remission with cyclosporine and then transition to one of the other drugs,” Dr. Sidbury said, noting dermatologists have their own preferences on which to use.
Several biologics are now being investigated for treatment of AD. They include interleukin (IL)-31 receptor (CIM331, Chugai Pharmaceutical), IL-22 (ILV-094, Rockefeller University), IL-13 (tralokinumab, MedImmune LLC), IL-12/IL-23 (ustekinumab, Rockefeller University) and IL-4 receptor dupilumab. Only once-weekly injection dupilumab is in Phase III.
Beck et al5 reported on blinded trials in adults with moderate-to-severe AD. “The trials both looked at biomarkers but also easy scales with really nice drops in the Eczema Area and Severity Index scores, really nice drops in the Investigator’s Global Assessment scores and beautiful drops in the itch scores,” he said, adding that anecdotal reports from adult study participants has been very positive.
Dupilumab seems as effective if not more and safer than more current systemic options, Dr. Sidbury said. “It may affect staph attachment in addition to treating specific AD inflammatory state. However, injection is not ideal for some, including most children,” he said.
 Other Therapies
Other Therapies
Other therapies, deeper in the pipeline that pose possibilities for eczema treatment include Janus kinase (JAK) inhibitors. The JAK inhibitor tofacitinib is FDA approved for the treatment of adult patients with moderately to severely active rheumatoid arthritis who had an inadequate response or intolerance to methotrexate and carries a black box warning. It is also used in hematology/oncology to treat refractory solid tumors and myelofibrosis, he explained.
Levy et al6 demonstrated that the oral JAK inhibitor tofacitinib citrate may be beneficial in the treatment of moderate-to-severe AD. The small study, evaluated 6 consecutive patients with moderate-to-severe AD who had failed standard treatment and were treated with tofacitinib citrate. Response to treatment was assessed using the Scoring of AD index. Decreased body suface area involvement of dermatitis and decreased erythema, edema/papulation, lichenification and excoriation were observed in all patients. The Scoring of AD index decreased by 66.6% from 36.5 to 12.2 (P<.05) during 8 to 29 weeks of treatment. There were no adverse events. Limitations of the study included the small sample size, lack of placebo control group and the possibility of bias.
Another JAK inhibitor, oclacitinib7,8 (Apoquel, Zoetis) is used to treat AD in dogs and seems to be a very effective treatment, he added.
These exciting new non-steroidal topical and systemic therapies in pipeline pose great potential for the treatment of eczema and atopic dermatitis, he concluded. “Julie Block, the head of the National Eczema Association, calls this the decade of eczema, and I think there’s a lot to that right now,” he said.
Disclosure: Dr. Sidbury was a site investigator in Anacor’s Phase III trial of a non-steroidal topical product for atopic dermatitis.
References
1. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351.
2. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116-132.
3. Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327-349.
4. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjunctive therapies and approaches.
J Am Acad Dermatol. 2014;71(6):1218-1233.
5. Beck LA, Thaçi D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Eng J Med. 2014; 371(2):130-139.
6. Levy LL, Urban J, King BA. Treatment of recalcitrant atopic dermatitis with the oral Janus kinase inhibitor tofacitinib citrate. J Am Acad Dermatol. 2015;73(3):395-399.
7. Cosgrove SB, Cleaver DM, King VL, et al. Long-term compassionate use of oclacitinib in dogs with atopic and allergic skin disease: safety, efficacy and quality of life. Vet Dermatol. 2015;26(3):171-179, e35.
8. Fukuyama T, Ehling S, Cook E, Bäumer W. Topically administered Janus-kinase inhibitors tofacitinib and oclacitinib display impressive antipruritic and anti-inflammatory responses in a model of allergic dermatitis. J Pharmacol Exp Ther. 2015;354(3):394-405.
The landscape of eczema research and treatment is vastly changing and potential new therapies are in development, according to Robert Sidbury, MD, MPH, associate professor, department of pediatrics, chief, division of dermatology, Seattle Children’s Hospital and University of Washington School of Medicine in Seattle, WA.
In 2000 there were only a handful of clinical trials for eczema and tacrolimus, pimecrolimus were poised for release. Now in 2015, 124 clinical trials are underway and potential new therapies are in development. The future appears promising with exciting new non-steroidal topical and systemic therapies in the pipeline, said Dr. Sidbury, who spoke on the topic at a session at the Summer 2015 American Academy of Dermatology meeting. He noted that much research has been done in the last few years and even the most recently published 2014 Atopic Dermatitis (AD) Guidelines,1-4 which were published in 4 parts, do not include this new research because the literature search used for the guidelines ended in 2012 and since 2013 more than 3,000 papers have been published.
New Treatment Pipeline
A Table from the National Eczema Association lists eczema and atopic dermatitis therapies that are in the development pipeline. The products range from Phase I to Phase III. “There’s a significant number of therapies in Phase III trials and these range from topicals to injections to orals, so they run the gamut and it is just an extraordinary list,” said Dr. Sidbury, who discussed numerous potential therapies, including AN2728 (now called Crisaborole Topical Ointment, 2%, Anacor Pharmaceuticals, Inc.), dupilumab (Sanofi/Regeneron Pharmaceuticals, Inc.) and tofacitinib (Xeljanz, Pfizer Inc.).
Dr. Sidbury noted that a practice gap exists in dermatology today with regard to eczema treatment. “Topical steroid fear is greatest in relation to younger children; however, most effective non-steroidal agents are not approved in younger children,” he said.
However, some possible alternatives are in the pipeline. Crisabarole, the AN2728-small molecule phosophodiesterase 4 (PDE-4) inhibitor with anti-inflammatory properties, is a boron-based small molecule (251 Da). Boron is essential for anti-inflammatory activity. The agent inhibits PDE-4 and reduces production of multiple inflammatory cytokines. Results from 2 Phase III, double-blind, vehicle-controlled studies were recently released. Each trial included 750 mild-to-moderate eczema patients (age 2-18 years old).
The primary study endpoint was clear or almost clear at day 29. In 1 trial, the results demonstrated that 32.8% in the Crisaborole arm and 25.4% in the vehicle arm reached the primary endpoint. The other trial has similar results, he said.
“Crisaborole was faster and more effective than the vehicle (statistically significant) and it was well-tolerated. There were some application site reactions but not dramatic numbers, and no serious side effects occurred,” he said.
At the time that the 2014 Atopic Dermatitis Guidelines1-4 were completed, 4 systemic therapy agents had been shown in the literature to be safe and effective in the treatment of severe AD: cyclosporine, mycophenolate, methotrexate and azathioprine. “I tend to use cyclosporine the most, but mainly because it works quicker, not because it is necessarily any better. There is a study that showed that mycophenolate doesn’t work as quickly, but it actually maybe has a more sustained benefit than cyclosporine. So I tend to try and induce remission with cyclosporine and then transition to one of the other drugs,” Dr. Sidbury said, noting dermatologists have their own preferences on which to use.
Several biologics are now being investigated for treatment of AD. They include interleukin (IL)-31 receptor (CIM331, Chugai Pharmaceutical), IL-22 (ILV-094, Rockefeller University), IL-13 (tralokinumab, MedImmune LLC), IL-12/IL-23 (ustekinumab, Rockefeller University) and IL-4 receptor dupilumab. Only once-weekly injection dupilumab is in Phase III.
Beck et al5 reported on blinded trials in adults with moderate-to-severe AD. “The trials both looked at biomarkers but also easy scales with really nice drops in the Eczema Area and Severity Index scores, really nice drops in the Investigator’s Global Assessment scores and beautiful drops in the itch scores,” he said, adding that anecdotal reports from adult study participants has been very positive.
Dupilumab seems as effective if not more and safer than more current systemic options, Dr. Sidbury said. “It may affect staph attachment in addition to treating specific AD inflammatory state. However, injection is not ideal for some, including most children,” he said.
Other Therapies
Other therapies, deeper in the pipeline that pose possibilities for eczema treatment include Janus kinase (JAK) inhibitors. The JAK inhibitor tofacitinib is FDA approved for the treatment of adult patients with moderately to severely active rheumatoid arthritis who had an inadequate response or intolerance to methotrexate and carries a black box warning. It is also used in hematology/oncology to treat refractory solid tumors and myelofibrosis, he explained.
Levy et al6 demonstrated that the oral JAK inhibitor tofacitinib citrate may be beneficial in the treatment of moderate-to-severe AD. The small study, evaluated 6 consecutive patients with moderate-to-severe AD who had failed standard treatment and were treated with tofacitinib citrate. Response to treatment was assessed using the Scoring of AD index. Decreased body suface area involvement of dermatitis and decreased erythema, edema/papulation, lichenification and excoriation were observed in all patients. The Scoring of AD index decreased by 66.6% from 36.5 to 12.2 (P<.05) during 8 to 29 weeks of treatment. There were no adverse events. Limitations of the study included the small sample size, lack of placebo control group and the possibility of bias.
Another JAK inhibitor, oclacitinib7,8 (Apoquel, Zoetis) is used to treat AD in dogs and seems to be a very effective treatment, he added.
These exciting new non-steroidal topical and systemic therapies in pipeline pose great potential for the treatment of eczema and atopic dermatitis, he concluded. “Julie Block, the head of the National Eczema Association, calls this the decade of eczema, and I think there’s a lot to that right now,” he said.
Disclosure: Dr. Sidbury was a site investigator in Anacor’s Phase III trial of a non-steroidal topical product for atopic dermatitis.
References
1. Eichenfield LF, Tom WL, Chamlin SL, et al. Guidelines of care for the management of atopic dermatitis: section 1. Diagnosis and assessment of atopic dermatitis. J Am Acad Dermatol. 2014;70(2):338-351.
2. Eichenfield LF, Tom WL, Berger TG, et al. Guidelines of care for the management of atopic dermatitis: section 2. Management and treatment of atopic dermatitis with topical therapies. J Am Acad Dermatol. 2014;71(1):116-132.
3. Sidbury R, Davis DM, Cohen DE, et al. Guidelines of care for the management of atopic dermatitis: section 3. Management and treatment with phototherapy and systemic agents. J Am Acad Dermatol. 2014;71(2):327-349.
4. Sidbury R, Tom WL, Bergman JN, et al. Guidelines of care for the management of atopic dermatitis: Section 4. Prevention of disease flares and use of adjunctive therapies and approaches.
J Am Acad Dermatol. 2014;71(6):1218-1233.
5. Beck LA, Thaçi D, Hamilton JD, et al. Dupilumab treatment in adults with moderate-to-severe atopic dermatitis. N Eng J Med. 2014; 371(2):130-139.
6. Levy LL, Urban J, King BA. Treatment of recalcitrant atopic dermatitis with the oral Janus kinase inhibitor tofacitinib citrate. J Am Acad Dermatol. 2015;73(3):395-399.
7. Cosgrove SB, Cleaver DM, King VL, et al. Long-term compassionate use of oclacitinib in dogs with atopic and allergic skin disease: safety, efficacy and quality of life. Vet Dermatol. 2015;26(3):171-179, e35.
8. Fukuyama T, Ehling S, Cook E, Bäumer W. Topically administered Janus-kinase inhibitors tofacitinib and oclacitinib display impressive antipruritic and anti-inflammatory responses in a model of allergic dermatitis. J Pharmacol Exp Ther. 2015;354(3):394-405.











