


Updated Melanoma Guidelines: What Dermatologists Need to Know
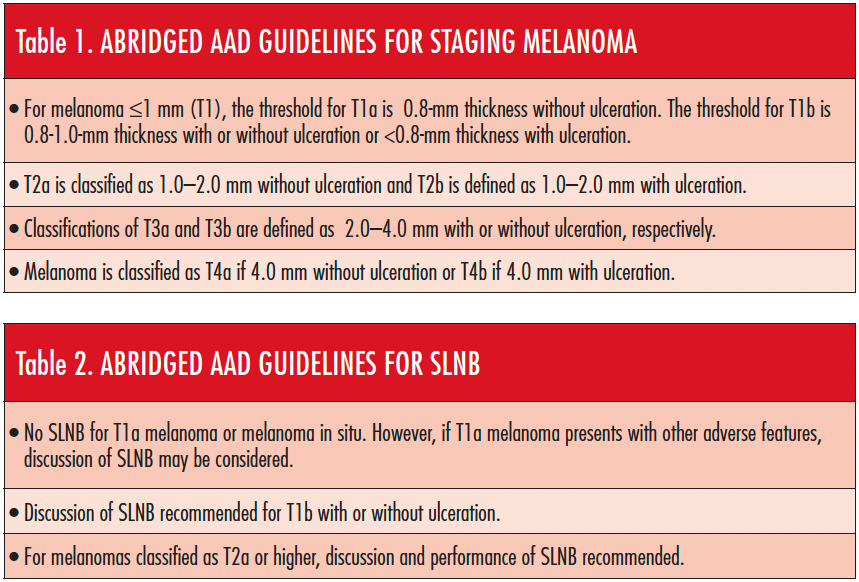
In the past decade, advances in the understanding of melanoma have led to new therapeutic options and treatment strategies. In response, late last year the American Academy of Dermatology (AAD) released updated guidelines on the management of primary cutaneous melanoma.1 The guidelines were last updated in 2011, and the new recommendations reflect changes made in the American Joint Committee on Cancer 8th edition for staging of cutaneous melanoma (Tables 1 and 2). They were developed based on the latest evidence in the field and address new areas of interest, including the management of melanoma among pregnant patients, considerations for genetic testing for hereditary risk, and managing cutaneous adverse events to novel immunotherapies and targeted agents.
The Dermatologist spoke with Susan M. Swetter, MD, chair of the work group that updated the guidelines and David Leffell, MD, about these changes and how they might impact practicing dermatologists. Dr Swetter is a professor of dermatology and director of the Pigmented Lesion and Melanoma Program and Cutaneous Oncology at Stanford University Medical Center and Cancer Institute in Stanford, California. Dr Leffell is the David Paige Smith Professor of dermatology and surgery and chief of the section of dermatologic surgery and cutaneous oncology in the department of dermatology at Yale School of Medicine in New Haven, Connecticut.
UPDATING THE GUIDELINES
“For the 2018 melanoma guidelines, our multidisciplinary work group identified key questions that are frequently encountered in clinical practice, including melanoma in pregnancy and management of dermatologic toxicities related to novel systemic immunotherapies and targeted agents,” said Dr Swetter. “We hoped to provide guidance for practitioners and patients alike, based on the available worldwide evidence.”
The multidisciplinary work group chaired by Dr Swetter included academic melanoma specialists in cutaneous, medical and surgical oncology, dermatopathology, Mohs micrographic surgery, and cutaneous surgery, as well as representatives from private practice and a patient advocacy organization. Together, they evaluated the current evidence and determined the strength of each recommendation, using expert opinion and medical consensus in cases where data were inconsistent or limited.
“The guidelines emphasize the advantages of multidisciplinary collaboration among dermatologists, surgeons, and medical oncologists, particularly for those patients at higher risk of disease recurrence,” said Dr Swetter.
WHAT STAYED THE SAME
Surgery continues to be the cornerstone of melanoma treatment. “Mohs micrographic surgery and other staged excision techniques can provide exhaustive peripheral margin histologic assessment for melanoma in situ, lentigo maligna type and tissue sparing in anatomically constrained sites,” said Dr Swetter. Data remain insufficient, however, to recommend Mohs surgery for invasive cutaneous melanoma, where the use of surgical margins less than 1 cm has not been adequately studied, she added.
In addition, Dr Swetter recommended that nonsurgical approaches, including the use of imiquimod and traditional forms of radiation therapy, should generally only be considered if surgery is impractical or contraindicated, and limited to melanoma in situ, lentigo maligna type, because cure rates are lower. “The bottom line is that these modalities require further investigation,” she said.
MANAGING MELANOMA IN PREGNANT PATIENTS
Pregnancy does not appear to negatively affect the risk or prognosis of cutaneous melanoma, according to the evidence-based guidelines.
“In the past, many women with a history of cutaneous melanoma were told to wait before becoming pregnant, due to concerns for a worse outcome,” said Dr Swetter. “Data from around the world, however, show no association between pregnancy and melanoma incidence, and pregnancy is not associated with adverse outcomes for cutaneous and metastatic melanoma. Additionally, the accurate staging of melanoma using sentinel lymph node biopsy (SLNB) and significantly improved therapies for advanced melanoma have made the rationale to delay becoming pregnant following a melanoma diagnosis less of a concern,” noted Dr Swetter.
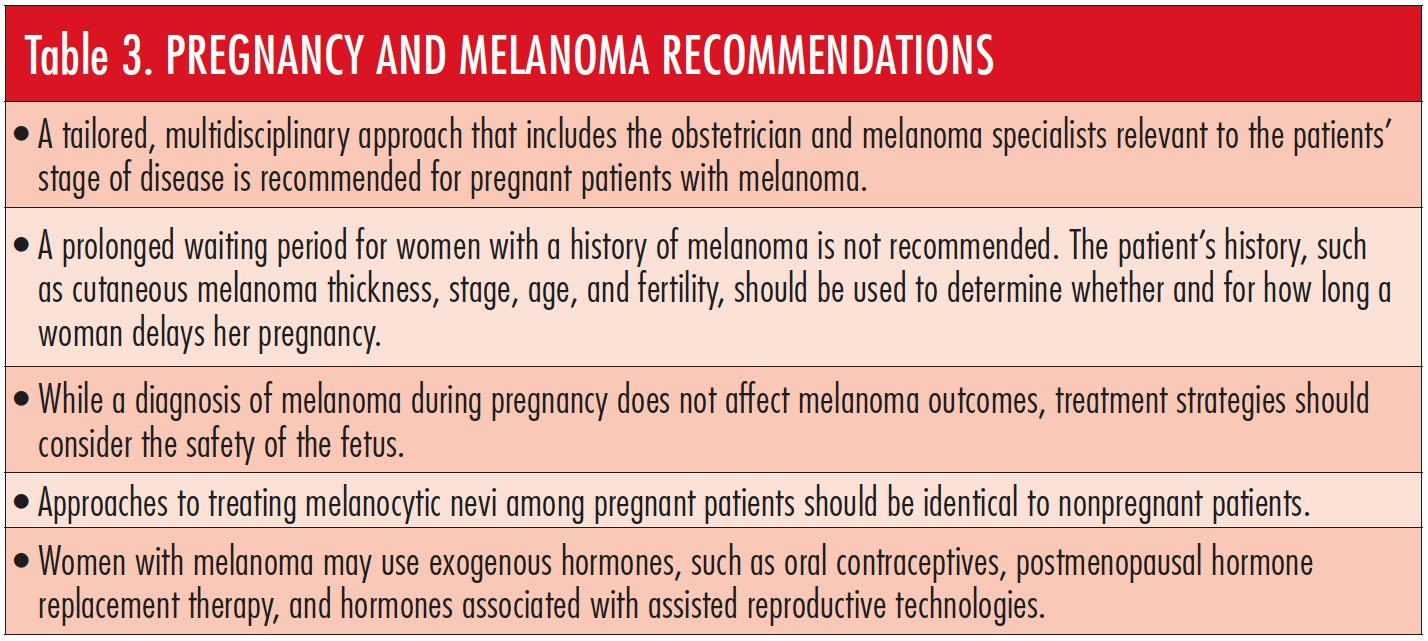
The authors of the new guidelines recommend that women receive a tailored, multidisciplinary approach to care, which includes the patient and her family, the obstetrician, and other melanoma specialists in decisions regarding treatment and family planning goals, Dr Swetter emphasized.
In addition, Dr Leffell found that “the guidelines serve to dispel a number of misconceptions about melanoma in pregnancy and provide a better, more rational basis for management.” The safety of exogenous hormones is one example. According to the work group, there is no evidence that exogenous hormones, oral contraceptives, other contraceptive devices/implants, or hormones associated with assisted reproductive technology affect the prognosis of women with a history of melanoma or increase the risk of new primary melanoma. Table 3 includes recommendations for pregnant patients.
ADDRESSING CUTANEOUS ADVERSE EVENTS
As more immunotherapies and targeted agents are developed and approved to treat various cancers, providers will need to be able to recognize common and rare cutaneous adverse effects among patients treated with these drugs. “It was important that we addressed these toxicities,” Dr Swetter said. “Dermatologists and other practitioners will not only see patients with a melanoma diagnosis on these agents, but also be asked to treat patients across the cancer spectrum.”
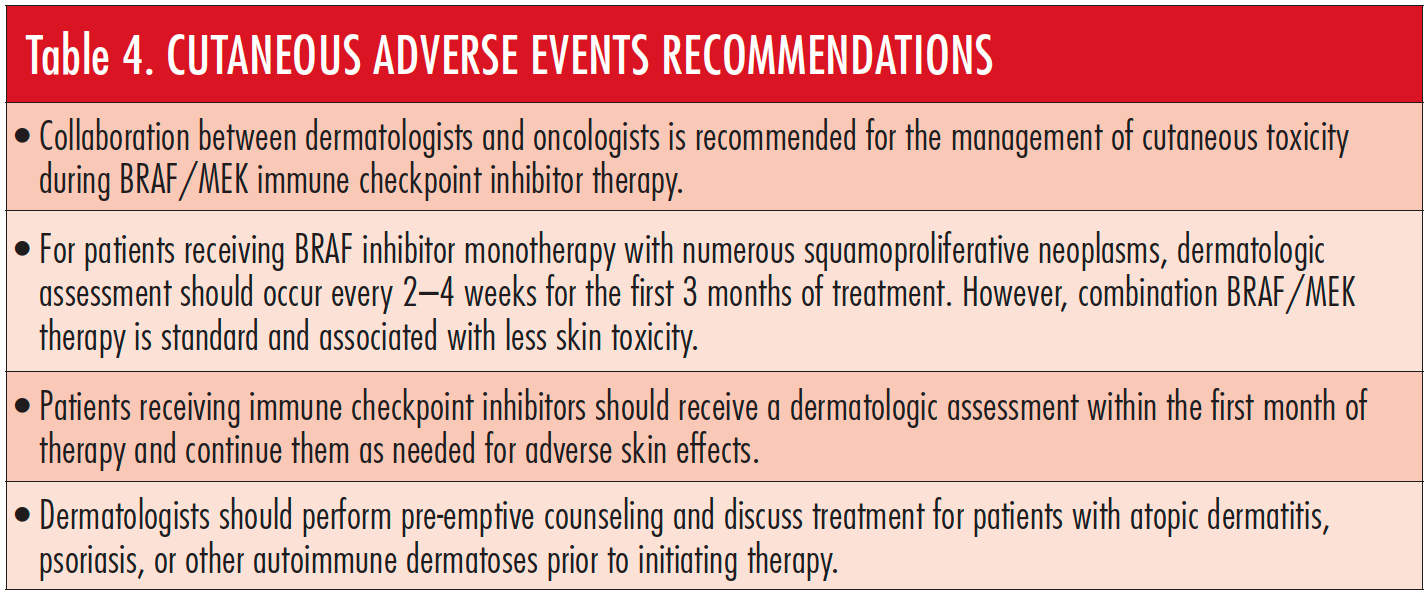
The updated guidelines include a new section on the management of dermatologic toxicities associated with these newer therapies, including BRAF and MEK inhibitors (Table 4) and immune checkpoint inhibitors. For example, common dermatologic toxicities associated with checkpoint inhibitors such as anti-programmed cell death protein 1 agents include nonspecific morbilliform dermatitis with or without pruritus, pruritus with or without dermatitis, vitiligo, and lichenoid skin eruptions, as well as unmasking of autoimmune conditions, including atopic dermatitis, psoriasis, and bullous disorders. These conditions can significantly impact a patient’s quality of life, as well as lead to discontinuation of potentially lifesaving therapy. “Understanding how to manage cutaneous adverse effects is critical to allowing patients to maintain cancerfighting treatment and to improve their quality of life while on therapy,” Dr Swetter said.
CONSIDERING GENETIC TESTING
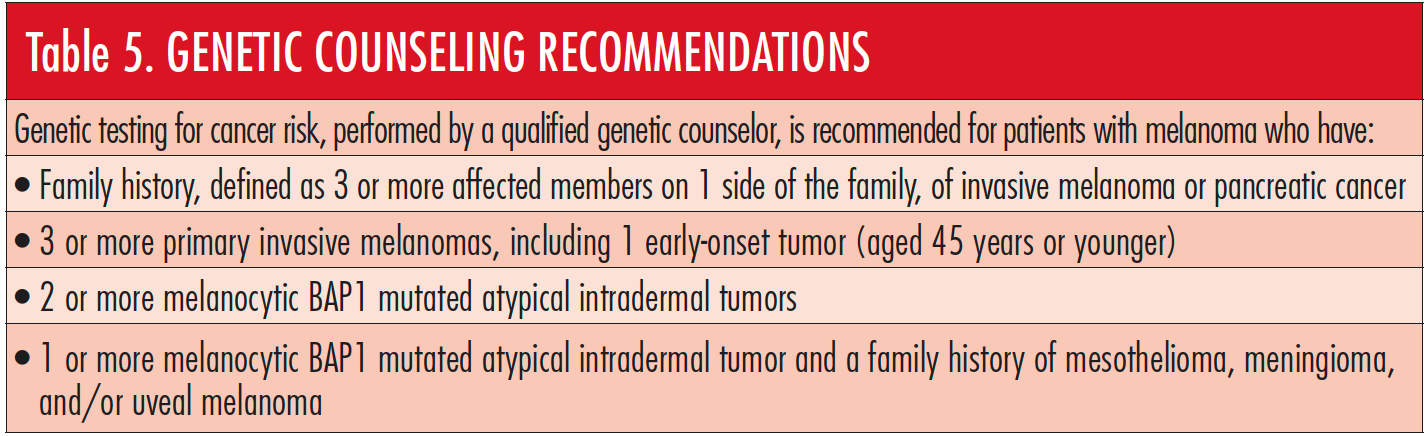
Although familial melanoma related to gene mutations is relatively uncommon, questions regarding genetic risk are frequently encountered by dermatologists, said Dr Swetter. Recommendations for genetic counseling are in Table 5.
“Because the disease can be so devastating, the role of genetic counseling is important and well-defined in the new guidelines,” said Dr Leffell. Information on genetics is also key due to the association of certain mutations with other forms of cancer,” he said.
The highest yield for specific gene testing for familial melanoma (for the CDKN2A/p16 mutation) occurs when 3 or more invasive cutaneous melanomas are found in an individual or family, particularly on the same side of the family, or when both pancreatic cancer and melanoma are found in the patient and/or family, according to Dr Swetter. “Asking a patient with melanoma about his or her family history of other cancers is equally important. For example, testing for BRCA mutations may be warranted if a patient has a strong family history of breast or ovarian cancer along with melanoma,” said Dr Swetter. The work group recommends that patients be referred to a qualified cancer genetics counselor to ensure verification of personal and family cancer pedigrees and to discuss genetic testing, when appropriate. “This is definitely an area that will be revised as further advances are made in understanding the genetic underpinnings of cancer and molecularly targeted therapy,” said Dr Swetter.
AREAS OF FUTURE RESEARCH
Due to continuous advancements in melanoma research, the recommendations and inclusion of newer technologies and therapies in guidelines continue to change. “Remember that the original idea of ‘wide excision’ involved 5 cm around the melanoma,” said Dr Leffell. “Most people do not know that that was based on a single autopsy case in the early 1900s, and margins were never really revisited until the 1980s.”
“In addition to the need for more research on the use of nonsurgical approaches to melanoma, other areas for future research include novel molecular techniques for melanoma prognostication in order to determine which patients should be treated and followed more intensively,” said Dr Swetter. “These techniques require ongoing prospective validation studies to determine their predictive value, how well they compare with and add to known histopathologic factors, and how best to incorporate them into clinical practice,” she said. “This is an exciting area that dermatologist can look forward to in the future.”
Other areas of investigation include the merits of melanoma screening and the use of prediagnostic imaging modalities and molecular techniques to aid in the biopsy of appropriate skin lesions (such as gene expression profiling with adhesive tape stripping); these were not included in the guidelines but could affect how we diagnosis cutaneous melanoma in the future, said Dr Swetter. “Additional challenging issues include the need for improved diagnosis of atypical Spitz tumors (which typically occur in the pediatric and adolescent population), as well as optimal management for clinically atypical/histologically dysplastic nevi,” she said.
According to Dr Leffell, one area that needs more research is the management of melanoma in situ and its biological behavior. “Melanoma in situ is becoming more common among the aging population and occurs primarily on sun-exposed areas of the skin that are cosmetically challenging” he said. Dr Leffell considers the best approach to be surgical but topical therapy can be used in appropriate circumstances. Although the guidelines mention Mohs surgery as an option, Dr Leffell believes there can be technical challenges in treating melanoma in situ with Mohs surgery.
Ongoing investigation into molecular and diagnostic imaging should provide evidence to establish guidelines for these topics in the future, said Dr Swetter. “Our hope is that these modalities will reduce unnecessary skin biopsies and help select patients for certain types of treatment or surveillance based on the molecular profile of their tumor,” she said.
USING THE GUIDELINES IN YOUR PRACTICE
“The updated melanoma guidelines accurately reflect current practices, which themselves represent ongoing evolution in our understanding and thinking about melanoma,” said Dr Leffell. Ultimately, however, he pointed out, they are only general recommendations, and physicians need to do what is best for each particular patient. “Margins of excision, for example, are an excellent guide, but in certain cases the standard excision is not practical,” he said. “We encourage dermatologists and other practitioners who treat melanoma to refer to the guidelines as diagnostic and clinical questions arise in practice,” said Dr Swetter. “For example, the frequency and intensity of cutaneous melanoma follow-up, including surveillance imaging, depends on the stage of disease, risk for recurrence, and risk of new primary melanoma.”
One other challenge, according to Dr Leffell, is ensuring that physicians are aware of the new guidelines. He recalls being contacted about a very elderly patient with dementia and an advanced melanoma on the scalp. The patient underwent excision with grafting and sentinel lymph node mapping and biopsy. “The guidelines advise against SLNB in the elderly when comorbid conditions exist and emphasize the importance of pursuing this on a case-by-case basis,” he said.
LOOKING AHEAD
“Treatment options for melanoma have improved significantly over the past decade, and there has been an explosion of data regarding melanoma pathogenesis and treatment,” said Dr Swetter. Although the work group’s main focus in updating the existing guidelines was on novel therapies for advanced disease, there will soon be trials that assess the efficacy and safety of immunotherapies for patients with cutaneous melanoma.
“Only in the last year have effective, more tolerable adjuvant therapies been FDA approved for patients with resected stage III melanoma, including patients with regional lymph node disease detected via SLNB” she said. “The hope is that less invasive procedures for melanoma will be performed in the future and replaced by better drugs and novel techniques that reduce morbidity and save lives.”
References:
- Swetter SM, Tsao H, Bichakjian CK, et al. Guidelines of care for the management of primary cutaneous melanoma [published online October 29, 2018]. J Am Acad Dermatol. doi:10.1016/j. jaad.2018.08.055








