


Quantification of Myocardial Mass Using Coronary Computed Tomography Angiography in Bifurcation Percutaneous Coronary Intervention and Association With Outcomes
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Objectives. To determine if quantification of the myocardial mass supplied by a side branch (SB) could be predictive of bifurcation percutaneous coronary intervention (PCI) outcomes.
Methods. The authors examined the characteristics and outcomes of 73 patients (81 lesions) who underwent bifurcation PCI and had coronary computed tomography angiography (CCTA)-based computed flow-based calculation of myocardial mass at risk within 6 months prior.
Results. The lesions analyzed were complex with high V-RESOLVE scores (12.0, 95%, interquartile range [IQR]: 9.0, 13.5). Provisional stenting was used in 67.9%, 2-stent techniques in 32.1%, and conversion from provisional to 2-stent stenting was performed in 11.1% of the lesions. The main vessel (MV) supplied 30.0% (IQR: 24.0%, 36.0%) and the SB supplied 10.0% (IQR: 7.0%, 13.0%) of the myocardium. Technical success was 94.9%. Major adverse cardiovascular events (MACE) occurred in 5.5% of the patients and SB occlusion (SBO) in 12.3% of the lesions. The ratio of SB to MV myocardial mass supply (SB/MV) was not associated with technical success (odds ratio [OR], 11.00; 95% confidence interval [CI], 0.01, 18.79; P = .500) or MACE (OR, 0.02; 95% CI, 0.00, 18.20; P = .300), but was associated with SBO (OR, 6.02*10-6; 95% CI, 2.42*10-10, 0.15; P = .020). SB/MV was normally distributed (W = 0.99, P = .467) with a mean of 0.35 (95% CI, 0.31, 0.38). In lesions where SBO occurred, V-RESOLVE scores were higher (16.0 vs 12.0, P = .017) and the SB/MV ratio was lower (0.22 vs 0.35, P = .007).
Conclusions. Myocardial mass derived from CT analysis can help assess the risk of SBO after bifurcation PCI.
Introduction
Determining the significance of a side branch (SB) is the first step in planning bifurcation percutaneous coronary intervention (PCI).1 Both the European Bifurcation Club and the Bifurcation Academic Research Consortium consider significant any SB perfusing greater than 10% of the myocardium.2,3 Coronary computed tomography angiography (CCTA) can provide information on stenoses, plaque characteristics, fractional flow reserve, and computed flow-based percentage of myocardium supplied by a SB.4,5 The percentage of myocardium supplied by specific coronary vessels has previously been validated against invasive measurement.6 The association of percentage of myocardium supplied with outcomes of bifurcation PCI has not been studied.
Methods
We analyzed the clinical and procedural data of 73 patients (81 lesions) who underwent bifurcation PCI at our center and had CCTA-based computed flow-based calculation of myocardial mass at risk of per-vessel subtended myocardium (Heartflow, Inc.) within 6 months prior. Pearson’s chi-square test was used to compare categorical variables. Continuous variables were presented as mean ± standard deviation or as median (interquartile range [IQR]) and compared using the independent-samples t-test for normally distributed variables and the Mann-Whitney U test for non-parametric variables. We performed univariable logistic regression to assess the association of percentage of myocardium supplied with technical success, major adverse cardiovascular events (MACE) and SB occlusion (SBO). We also performed multivariable analyses after adjusting for SB diameter. R Statistical Software, version 4.4.0 (R Foundation for Statistical Computing) was used for analyses, and a P-value of less than 0.05 was classified as statistically significant.
Results
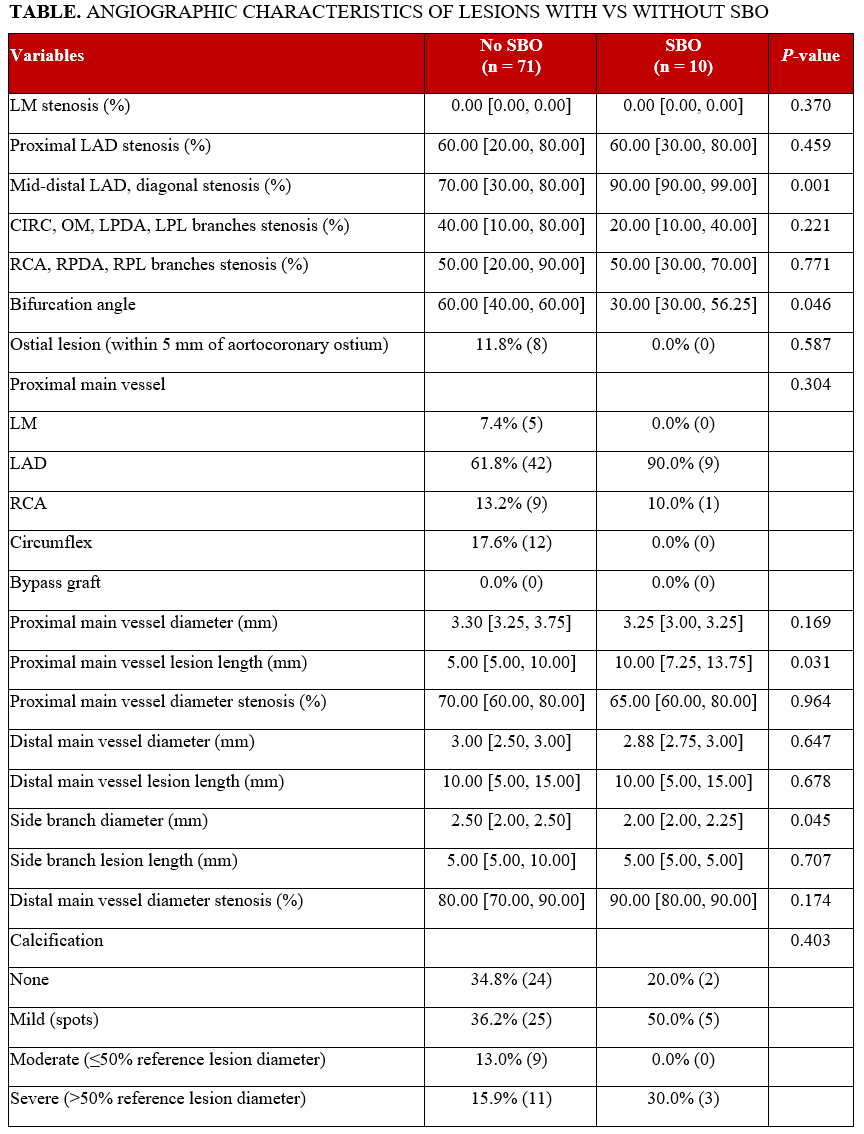
The median age of the patients was 67 years; 65.8% were male and had multiple comorbidities, including hypertension (67.1%), dyslipidemia (83.6%), prior PCI (13.7%) and prior myocardial infarction (16.4%). Of the lesions analyzed, 65.4% were bifurcations involving the left anterior descending artery (LAD), 53.2% were Medina 1,1,1, and 29.1% had moderate/severe proximal main vessel (MV) calcification. Median proximal MV diameter stenosis was 70.0%, distal was 80.0%, and the median V-RESOLVE score was 12.00. Lesions where SBO occurred had higher angiographic complexity with more acute bifurcation angles (30.0° vs 60.0°, P = .046) and smaller SB diameters (2.0 mm vs 2.5 mm, P = .045) (Table). Provisional stenting was used in 67.9%, 2-stent techniques in 32.1%, and 11.1% converted from provisional to 2-stent techniques. The SB was protected in 32.1% of the lesions and SBO occurred in 12.3%. SBO lesions had higher use of provisional stenting (100.0% vs 63.4%, P = .026) compared with no-SBO lesions, but similar 2-stent technique use (20.0% vs 33.8%, P = .488) and conversion from provisional to 2-stent techniques (20.0% vs 9.9%, P = .307). MACE occurred in 5.5%.
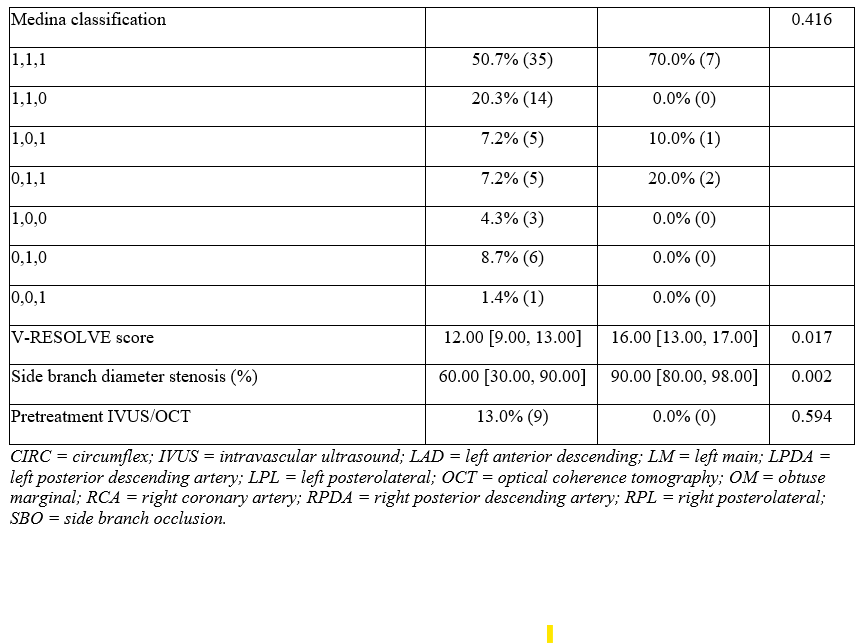
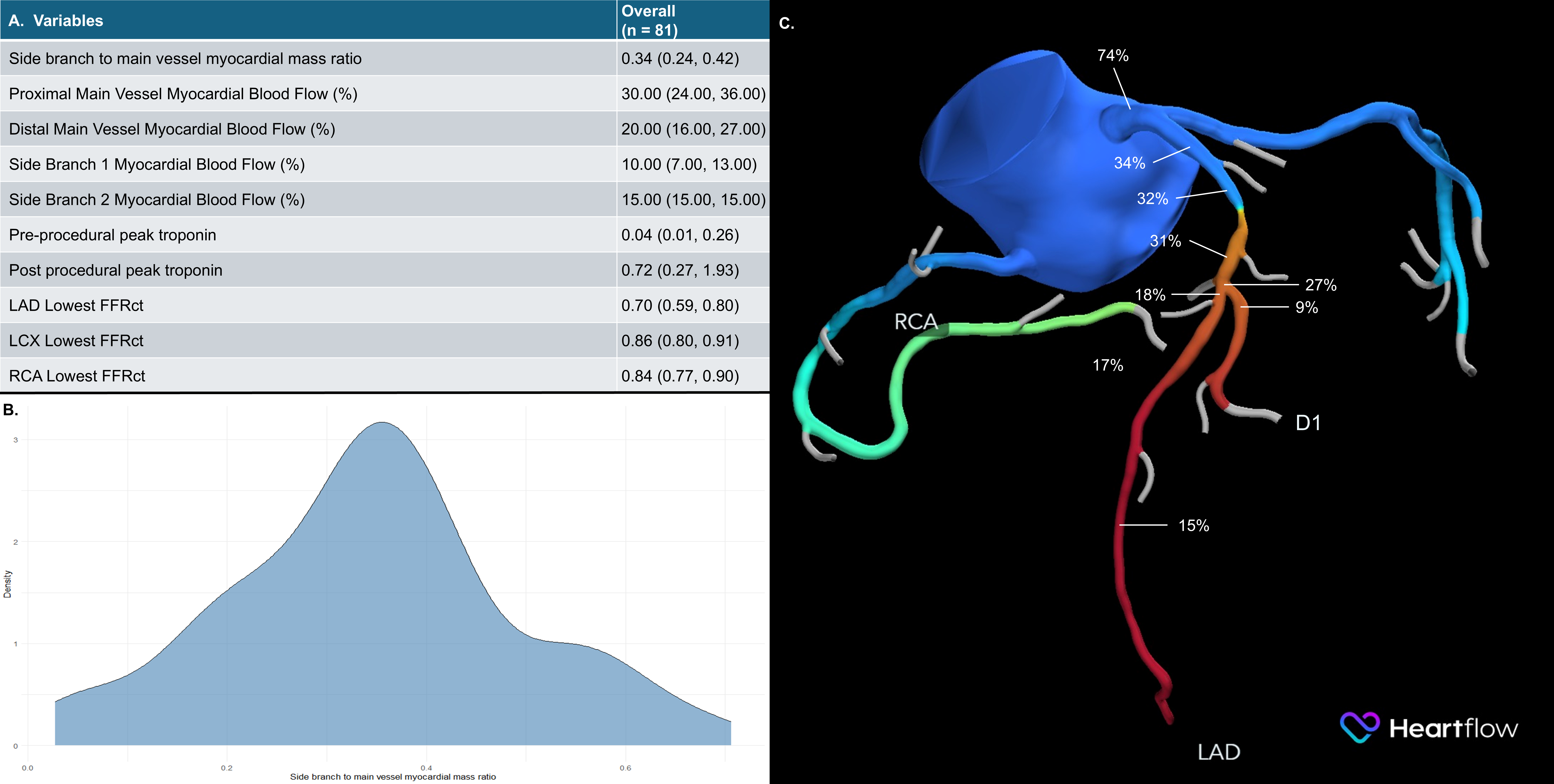
The MV supplied 30.0% (IQR: 24.0%, 36.0%) and the SB supplied 10.0% (IQR: 7.0%, 13.0%) of the myocardium (Figure A). The ratio of SB to MV myocardial mass supply (SB/MV) was normally distributed (W = 0.99, P = .467) with a mean of 0.35 (95% confidence interval [CI], 0.31, 0.38) (Figure B). SB/MV ratio was not associated with technical success (odds ratio [OR], 11.00; 95% CI, 0.01, 18.79; P = .500) or MACE (OR, 0.02; 95% CI, 0.00, 18.20; P = .300) but was associated with SBO (OR, 6.02*10-6; 95% CI, 2.42*10-10, 0.15; P = .020) after adjusting for SB diameter. In lesions where SBO occurred, V-RESOLVE scores were higher (16.0 vs 12.0, P = .017) and the SB/MV ratio was lower (0.22 vs 0.35, P = .007). Lesions with higher SB/MV (> 0.3) where SBO occurred were all in the LAD, had higher V-RESOLVE scores (17.0 vs 12.0, P = .044), and higher low attenuation plaque volume in the LAD (21.0 mm3 vs 8.0 mm3, P = .033) compared with cases without SBO. There were no differences in provisional stenting (100.0% vs 60.8%, P = .287) or 2-stent technique use (33.3% vs 37.3%, P > .999).
Discussion
Our results demonstrate that CCTA-derived subtended myocardium is a useful metric in assessing the risk of SBO during bifurcation PCI (Figure C). Lower SB/MV ratio means higher risk of SBO. In such cases, an upfront 2-stent technique might be useful or, if provisional stenting is planned, inserting a SB guidewire may reduce the risk of SB closure. Further validation of this metric is required to explore its clinical utility.
Limitations
Our study has limitations. The study sample size was small and there was no independent adjudication of clinical events or core laboratory analysis of the study’s angiograms and CCTA. Our center is specialized in complex PCI, potentially limiting the external validity of our results. The impact of the percentage of myocardial supply derived from CCTA on complex PCI has not been validated in large studies.
Conclusions
CCTA-derived subtended SB and MV myocardium may help predict SBO during bifurcation PCI.
Affiliations and Disclosures
Dimitrios Strepkos, MD; Michaella Alexandrou, MD; Pedro E.P. Carvalho, MD; Eleni Kladou, MD; Nick Williford, MD; Olga Mastrodemos, BA; Bavana V. Rangan, BDS, MPH; Yader Sandoval, MD; Emmanouil S. Brilakis, MD, PhD
From the Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, Minnesota.
Part of the data in this manuscript was previously presented at the Transcatheter Cardiovascular Therapeutics (TCT) 2025 conference (Strepkos, D, Alexandrou, M, Mutlu, D. et al. TCT-382 Quantification of myocardial mass supplied by the side branch and main vessel of patients undergoing bifurcation PCI using the Heartflow analysis of coronary computed tomography angiography and association with clinical outcomes. JACC. 2025;86(17_Supplement):B168. doi:10.1016/j.jacc.2025.09.493)
Disclosures: Dr Sandoval is a consultant for and serves on the advisory board of Abbott; is a consultant for, serves on the advisory board of, and is a speaker for Roche Diagnostics; is a consultant for, serves on the advisory board of, and is a speaker for Philips; serves on the advisory board of Zoll; is a consultant for and serves on the advisory board of GE Healthcare; is a consultant for CathWorks; is a speaker for HeartFlow, Inc.; is a speaker for and has received a research grant from Cleerly Health; is an associate editor for JACC Advances; and he and others hold patent 20210401347. Dr Brilakis receives consulting/speaker honoraria from Abbott Vascular, the American Heart Association (associate editor, Circulation), Boston Scientific, Cardiovascular Innovations Foundation (Board of Directors), Cordis, Elsevier, GE Healthcare, IMDS, Medtronic, SIS Medical, Teleflex, and Terumo; research support from Boston Scientific, GE Healthcare; is the owner of Hippocrates LLC; and is a shareholder in Cleerly Health, LifeLens Technologies, Inc., MHI Ventures, Stallion Medical, and TrueVue, Inc. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, Minneapolis Heart Institute, 920 E 28th Street #300, Minneapolis, MN 55407, USA. Email: esbrilakis@gmail.com
References
1. Brilakis E. Bifurcations. In: Brilakis E, ed. Manual of Percutaneous Coronary Interventions: A Step-by-Step Approach. Academic Press;2021:267-301. doi:10.1016/B978-0-12-819367-9.00016-0
2. Lunardi M, Louvard Y, Lefèvre T, et al. Definitions and standardized endpoints for treatment of coronary bifurcations. EuroIntervention. 2023;19(10):e807-e831. doi:10.4244/EIJ-E-22-00018
3. Pan M, Lassen JF, Burzotta F, et al. The 17th expert consensus document of the European Bifurcation Club - techniques to preserve access to the side branch during stepwise provisional stenting. EuroIntervention. 2023;19(1):26-36. doi:10.4244/EIJ-D-23-00124
4. Morris MF, Chandrasekhar M, Gudi H, et al. A study to measure the ability of AI-CSQ to suppoRt The busy CCTA reader: SMART-CT. J Cardiovasc Comput Tomogr. 2024;18(2):213-214. doi:10.1016/j.jcct.2023.09.006
5. Narula J, Stuckey TD, Nakazawa G, et al. Prospective deep learning-based quantitative assessment of coronary plaque by computed tomography angiography compared with intravascular ultrasound: the REVEALPLAQUE study. Eur Heart J Cardiovasc Imaging. 2024;25(9):1287-1295. doi:10.1093/ehjci/jeae115
6. Keulards DCJ, Fournier S, van 't Veer M, et al. Computed tomographic myocardial mass compared with invasive myocardial perfusion measurement. Heart. 2020;106(19):1489-1494. doi:10.1136/heartjnl-2020-316689











