


Drug-Eluting Stent, Drug-Coated Balloon, or Conventional Angioplasty for In-Stent Coronary Restenosis: An Updated Meta-Analysis of Randomized Trials
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
Abstract
Objectives. The SELUTION SLR 014 In-stent Restenosis (SELUTION4ISR) trial showed noninferiority of drug-coated balloons (DCB) for the outcome of target lesion failure (TLF) when compared with standard of care (80% drug-eluting stent [DES] and 20% plain old balloon angioplasty [POBA]). It was notable that in the DCB vs DES subgroup analysis there was a numerically higher rate of TLF with DCB (15.3% vs 7.1%). The authors aimed to re-evaluate the outcomes of DES, DCB, or POBA in patients with coronary in-stent restenosis (ISR).
Methods. The authors searched PubMed and EMBASE databases for randomized clinical trials (RCTs) that compared these 3 percutaneous revascularization strategies for ISR until March 15, 2026. Outcomes included major adverse cardiovascular events (MACE), target lesion revascularization (TLR), all-cause mortality, cardiovascular mortality, and stent thrombosis.
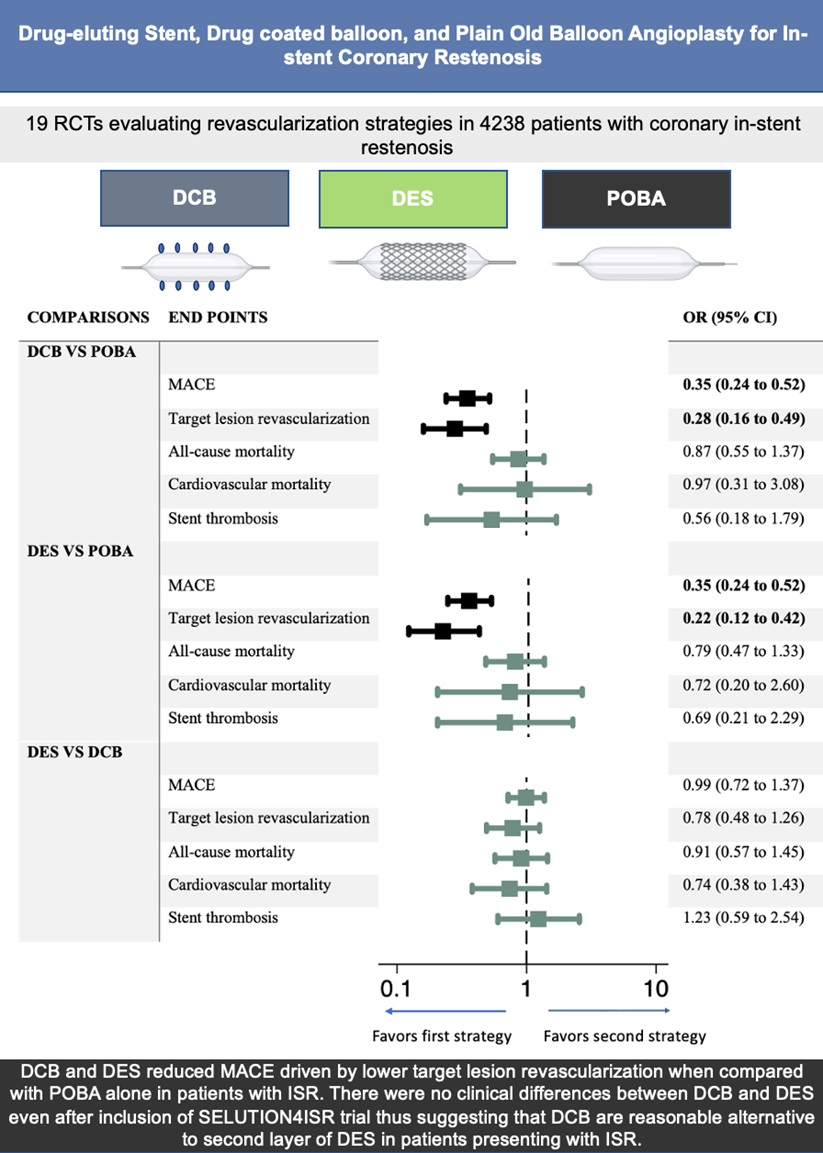
Results. From 19 RCTs that randomized 4238 patients with ISR at mean follow-up of 19.6 months, there was a significant reduction in MACE and TLR with both DCB (OR, 0.35; 95% CI, 0.24-0.52 and OR, 0.28; 95% CI, 0.16-0.49, respectively) and DES (OR, 0.35; 95% CI, 0.24-0.52 and OR, 0.22; 95% CI, 0.12-0.42, respectively) when compared with POBA. There were no significant differences in clinical outcomes between DCB and DES.
Conclusions. In patients with ISR, DCB reduced MACE/TLR when compared with POBA. There were no clinical differences between DCB and DES even after inclusion of the SELUTION4ISR trial, thus suggesting that DCB are a reasonable alternative to repeat stenting in patients presenting with ISR.
Introduction
The 2024 European Society of Cardiology guidelines downgraded drug-coated balloons (DCB) in preference for drug-eluting stents (DES) for DES in-stent coronary restenosis (ISR) (Class I and level of evidence A).1 Our recent network meta-analysis comparing DCB, DES, and plain old balloon angioplasty (POBA) for ISR did not show any difference in clinical outcomes between DCB and DES.2 However, since the publication of our analysis, the SELUTION SLR 014 In-stent Restenosis (SELUTION4ISR) trial was presented and showed noninferiority of DCB for the outcome of target lesion failure (TLF, defined as composite of cardiovascular mortality, target vessel myocardial infarction [MI], and target lesion revascularization [TLR]) when compared with standard of care (80% DES and 20% POBA). It was notable that in the DCB vs DES subgroup analysis there was a numerically higher rate of TLF with DCB (15.3% vs 7.1%).3
The aim of this study was to perform an updated meta-analysis of randomized controlled trials (RCT) to examine the efficacy of DCB when compared with DES and POBA in patients with coronary ISR, incorporating the SELUTION4ISR results and the recently presented long-term results of the AGENT IDE trial.4
Methods
A time limited search until March 15, 2026, was conducted using PubMed (National Institutes of Health) and EMBASE (Elsevier) databases. We used the following Medical Education Subject Headings for searching eligible studies: coronary artery disease, drug-coated balloon, drug-eluting stents, efficacy, in-stent restenosis, and plain old balloon angioplasty. The inclusion criteria were RCTs that compared the effect of DCB, DES, or POBA. Single-arm studies, observational studies, editorials, letters, and review articles were excluded. The co-primary outcomes of interest were major adverse cardiovascular events (MACE) and TLR. Secondary outcomes were all-cause mortality, cardiovascular mortality, and stent thrombosis. The revascularization strategies were categorized into 3 groups: 1) DCB; 2) DES; and 3) POBA (reference treatment arm).
Adverse events using odds ratios (OR) and 95% confidence intervals (CI) were calculated using the random-effects model with the DerSimonian and Laird method. Frequentist estimation of network meta-analysis models was used for DCB, DES, and POBA (reference). Finally, a network funnel plot was used to estimate publication bias and small study effects.
Results
Of 1400 studies, 19 RCTs were included in the final analysis, including 4238 patients. Sixteen trials evaluated DCB with 1926 patients, 14 trials evaluated DES with 1561 patients, and 9 trials evaluated POBA with 751 patients (Supplemental Figures 1-5, panel A). The mean age of participants was 67 years, and 75% were men. The mean duration of follow-up was 19.6 months. The majority of the DCB used were paclitaxel-coated balloons, except in the SELUTION4ISR trial, where sirolimus-coated balloons were used. 3
There was a significant reduction in MACE and TLR with DCB (OR, 0.35; 95% CI, 0.24-0.52 and OR, 0.28; 95% CI, 0.16-0.49, respectively) and DES (OR, 0.35; 95% CI, 0.24-0.52 and OR, 0.22; 95% CI, 0.12-0.42, respectively) when compared with POBA (Figure). There were no significant differences in other clinical outcomes. Further, there was no difference in any clinical outcomes of DCB vs DES. There was no evidence of publication bias (Supplemental Figures 1-5, panel B) or inconsistency in the network meta-analysis (P > .05) (Supplemental Table). There was no significant difference in overall outcome, with exclusion of the trial testing sirolimus-eluting balloon for DCB vs POBA (MACE: OR, 0.33; 95% CI, 0.24-0.47 and TLR: OR, 0.27; 95%, CI 0.16-0.46).2
Discussion
The results of this updated network meta-analysis using 19 RCTs after the addition of the SELUTION4ISR trial and long-term (3 years) follow-up of the AGENT IDE trial showed results consistent with those of our recently published meta-analysis. In summary, there was a significant reduction in MACE and TLR with DCB and DES when compared with POBA. There was no difference in any clinical outcome of DCB vs DES.
The SELUTION4ISR trial showed noninferiority of DCB for the outcome of TLF when compared with standard of care. The standard of care in this trial included 80% DES and 20% POBA. However, the major limitation of the trial was a wide noninferiority margin (10%). Moreover, in the DCB vs DES subgroup analysis, there was numerically higher TLF with DCB when compared with DES (15.3% vs 7.1%).3 This subgroup analysis once again sparked the debate as to whether DCB is a reasonable alternative to repeat DES, as is standard. It is notable that this trial had 97.5% use of intracoronary imaging, significantly higher than 73.8% in the AGENT IDE trial5 and 58.7% in the RESTORE trial.6 The results of our network analysis are consistent with our recently published analysis showing no significant difference in clinical outcomes between DCB and DES. Given the totality of the evidence, DCB is a reasonable alternative to DES with the added advantage of no additional metallic implant.
A notable limitation of our analysis is that it is a trial-level meta-analysis; hence, granular details could not be evaluated and many trials did not specify the number of stent layers.
Conclusions
In summary, DCB and DES reduced MACE driven by lower TLR when compared with POBA alone in patients with ISR. There were no clinical differences between DCB and DES even after inclusion of the SELUTION4ISR trial, thus suggesting that DCB are a reasonable alternative to repeat stenting in patients presenting with ISR.
Affiliations and Disclosures
M. Haisum Maqsood, MD, MS1; Robert S. Zhang, MD2; Sripal Bangalore, MD, MHA3
From the 1Department of Cardiology, DeBakey Heart and Vascular Center, Houston Methodist Hospital, Houston, Texas; 2Division of Cardiology, Department of Medicine, New York Presbyterian Hospital, Weill Cornell Medicine, New York, New York; 3Department of Medicine, Leon H. Charney Division of Cardiology, NYU Grossman School of Medicine, New York.
Meta-analysis registration number at PROSPERO: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024598433
Disclosures: Dr Bangalore is on the advisory board for Abbott Vascular, Boston Scientific, Shockwave, Imperative Care, AngioDynamics, Zoll, and Stryker. The remaining authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Sripal Bangalore, MD, MHA, Division of Cardiovascular Medicine, New York University Grossman School of Medicine, New York, NY, USA. Email: sripalbangalore@gmail.com; X: @sripalbangalore
References
1. Vrints C, Andreotti F, Koskinas KC, et al; ESC Scientific Document Group. 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415-3537. doi:10.1093/eurheartj/ehae177
2. Maqsood MH, Zhang RS, Rawal N, Sella G, Kleiman NS, Bangalore S. Drug-eluting stent, drug-coated balloon, or plain old balloon angioplasty for in-stent coronary restenosis: insights from a mixed treatment comparison meta-analysis of randomized trials. Circ Cardiovasc Interv. 2025;18(12):e015161. doi:10.1161/CIRCINTERVENTIONS.125.015161
3. Cutlip DE. Randomized Trial of a Sirolimus Eluting Balloon versus Repeat Drug-Eluting Stenting or Balloon Angioplasty for Coronary In-stent Restenosis. Late breaking presented at: Transcatheter Cardiovascular Therapeutics Conference (TCT); October 28-31, 2025; San Francisco, CA.
4. Yeh R. Paclitaxel-Coated versus Uncoated Balloon for Coronary In-Stent Restenosis – Three-year Outcomes of the AGENT IDE Trial. Late breaking presented at: Cardiovascular Research Technologies (CRT); March 6-9, 2026; Washington, DC.
5. Yeh RW, Shlofmitz R, Moses J, et al; AGENT IDE Investigators. Paclitaxel-coated balloon vs uncoated balloon for coronary in-stent restenosis: the AGENT IDE randomized clinical trial. JAMA. 2024;331(12):1015-1024. doi:10.1001/jama.2024.1361
6. Wong YTA, Kang DY, Lee JB, et al. Comparison of drug-eluting stents and drug-coated balloon for the treatment of drug-eluting coronary stent restenosis: a randomized RESTORE trial. Am Heart J. 2018;197:35-42. doi:10.1016/j.ahj.2017.11.008














