‘Size it and Fix it’: Pulsatile Abdomen and Presyncope Post Pacemaker Implantation
A 69-year-old obese man who had undergone permanent pacemaker implantation (VVIR, Medtronic) 3 weeks prior presented with a one-day history of experiencing continued, forceful pulsations in his abdomen followed by presyncope. Examination revealed him to be conscious and oriented with a pulse rate of 35 bpm and blood pressure of 150/60 mmHg. Pulsatile right hypochondrium and liver was observed (Video). Cardiac auscultation revealed no murmurs. Electrocardiogram (ECG) and chest X-ray (Figure 1) were taken.
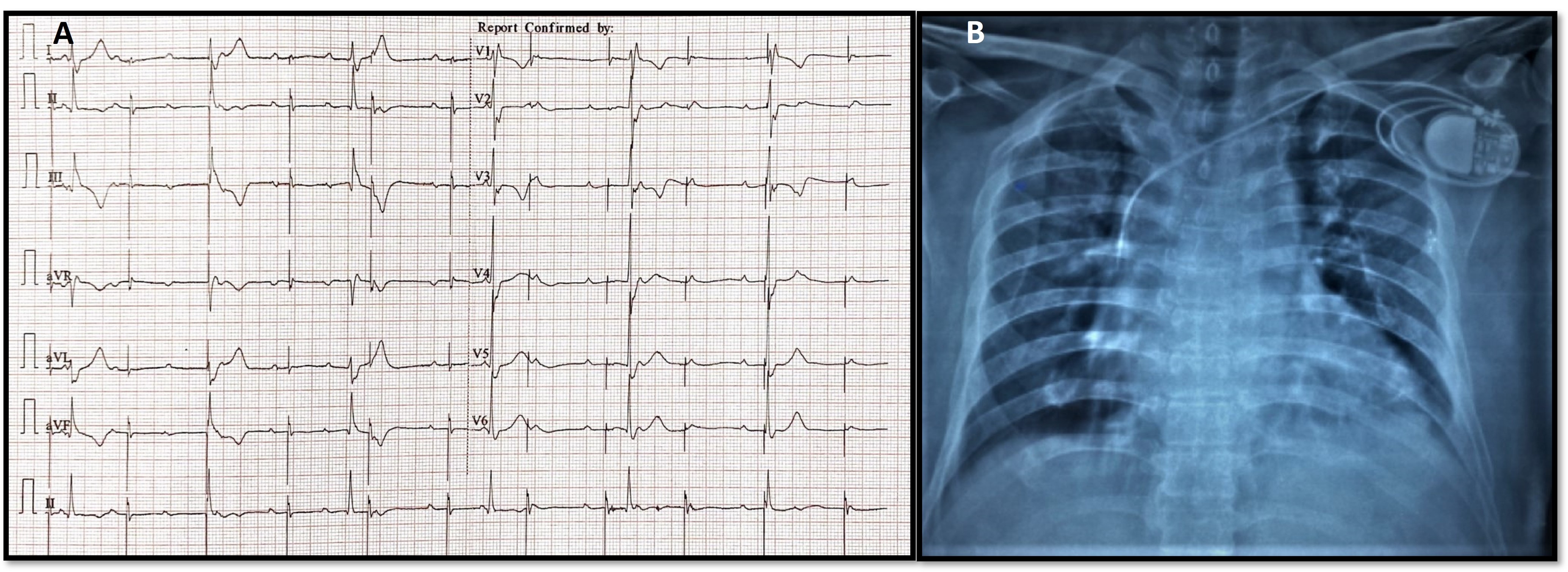
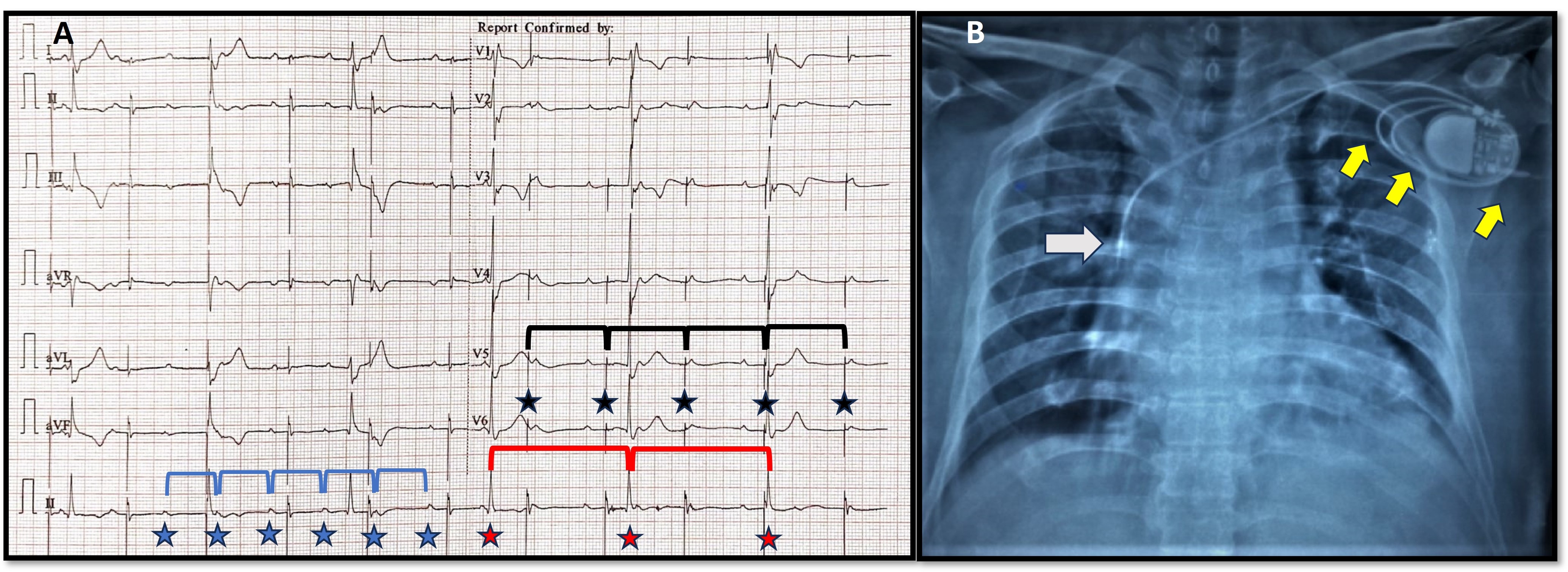
ECG analysis (Figure 2A) showed baseline atrioventricular (AV) dissociation with an atrial rate of 100 bpm. Pacemaker stimulus artifact was noted at regular intervals of 66/min (lower set rate of the VVIR pacemaker) but was not followed by a P wave or QRS complex (capture failure). Intrinsic ventricular escape rhythm was wide (QRS duration 0.16 sec) at a rate of 36 bpm and was not sensed (sensing failure). Chest X-ray (Figure 2B) revealed macro-dislodgement of ventricular lead with tip placed along the superior vena cava-right atrial (SVC-RA) junction, and coiling of leads around the pacemaker generator in its spacious pocket. No obvious lead fracture or insulation breaks were evident. The pacemaker pocket was reopened, and leads were uncoiled, repositioned, and connected to the same generator. Reduction of pocket size to snugly fit the pulse generator, tight suture sleeve fixation of the lead, and extra reinforcement suture fixation of the generator to the pectoral muscle were done.
Our patient was diagnosed with Reel syndrome, one among the 3 rare variants of lead macro dislodgement syndromes causing device malfunction. Generally, it is seen within a month due to rotation of the generator on its transverse axis with resultant reeling of the electrode around it. Contrary to Twiddler’s syndrome, lead damage is unlikely in Reel, hence the same lead can be repositioned. Obesity, large pocket size, and self-manipulation were some probable risk factors, and right phrenic nerve stimulation by the displaced lead led to rhythmic contractions of the diaphragm in our case. Timely diagnosis is essential to avoid catastrophic consequences like syncope or arrhythmias in device-dependent patients. Chest X-ray is a simple, important imaging modality in differentiating these syndromes. Female gender, obesity, and psychiatric illnesses are factors responsible for lead dislodgement. Dictum of optimal pocket size and tight fixation of lead and generator should be meticulously followed during device implantations.
Affiliations and Disclosures
From the 1Department of Cardiology, SRM Medical College and Research Centre, Potheri, Chengalpattu, Tamil Nadu, India; and the 2Department of Cardiology, Al-Dhannah hospital, Aldhannah, Abu Dhabi, UAE
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Author for correspondence: Dr. Sriram Veeraraghavan, Department of Cardiology, SRM Medical College Hospital and Research Centre, SRM Nagar, Potheri , Chengalpattu , TN, India 603203; Email: srivats.007.2003@gmail.com