


When Gout Meets Diabetes: A Metabolic Red Flag for Podiatrists
In patients with diabetes, gout should never be viewed as an isolated joint problem. This article argues that concurrent gout and diabetes signal a broader state of insulin resistance, cardiovascular risk, and kidney dysfunction—while also demanding heightened diagnostic caution, since infection in the diabetic foot can closely mimic a gout flare.
Key Takeaways
1. Gout in a patient with diabetes is a metabolic warning sign, not just a rheumatologic event. The article emphasizes that hyperuricemia and type 2 diabetes are linked through insulin resistance in a bidirectional cycle: elevated uric acid can worsen insulin signaling, while insulin resistance can increase urate reabsorption and push uric acid higher. For podiatrists, that means gout may be an important clue to broader cardiometabolic instability rather than a standalone diagnosis.
2. In the diabetic foot, the biggest danger is mistaking infection for gout. A hot, swollen, erythematous foot in a patient with diabetes should not be reflexively labeled as a gout flare. Because cellulitis, septic arthritis, osteomyelitis, and other serious infections can present similarly (and may coexist with gout) the article urges clinicians to maintain a low threshold for infection work-up, aspiration, imaging, referral, and hospital-level care when red flags are present.
3. Podiatrists have an important front-line role in both systemic risk screening and limb preservation. The article frames podiatrists as key clinicians for identifying uncontrolled diabetes, hypertension, dyslipidemia, kidney disease, neuropathy, and prior foot complications in patients presenting with gout. By combining metabolic screening, careful foot evaluation, and coordinated referral, podiatrists can help prevent both cardiovascular complications and devastating limb-threatening outcomes.
A 64-year-old male with obesity and type 2 diabetes presents with acute pain, swelling, and warmth in the left first toe. He has hypertension, dyslipidemia, and suffered a previous myocardial infarction. His HbA1c is 8.2%, and his blood pressure is 158/92 mmHg. In a typical visit for presumed gout, it is tempting to assume this is "just another flare," prescribe colchicine or another non-steroidal anti-inflammatory drug (NSAID), and consider urate-lowering therapy. Yet this patient represents something far more complex: a constellation of cardiometabolic disease in which gout is not merely an incidental finding but a marker of dangerous, multisystem metabolic derangement, superimposed on a foot at high risk for infection and limb loss.1-6
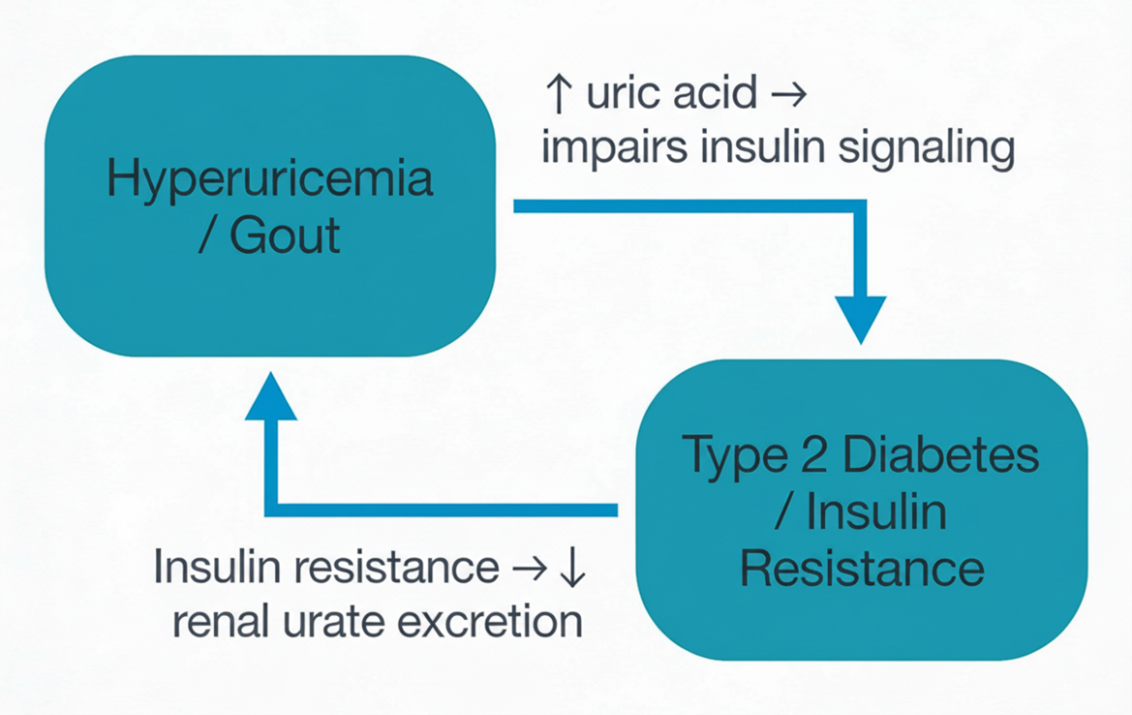
A growing body of evidence supports a bidirectional relationship between hyperuricemia and diabetes: elevated serum uric acid predicts incident type 2 diabetes in longitudinal cohorts, while existing insulin resistance and hyperinsulinemia, in turn, promote renal urate reabsorption and higher uric acid levels (Figure 1). In practical terms, this means that a patient with gout who does not have diabetes may be on the path toward that diagnosis, with rising uric acid signaling worsening insulin resistance and cardiometabolic risk.1,2,4,6,7
For podiatrists managing patients with gout and diabetes, recognizing this metabolic nexus is essential—but so is resisting the urge to reflexively label every hot, swollen diabetic foot as "gout" without rigorously excluding infection. Gout and type 2 diabetes share common pathophysiologic roots, and their coexistence signals exceptionally high risk for cardiovascular events, progressive kidney disease, and foot complications including neuropathy, ulceration, infection, and amputation.1,2,5,6 This article explores the metabolic links between gout and diabetes, emphasizes the critical need to distinguish gout flares from infection in the diabetic foot, and outlines a practical framework for systemic risk stratification and diagnostic safety.
The Insulin Resistance Hub: Why Gout and Diabetes Cluster Together
Hyperuricemia and type 2 diabetes are tightly intertwined through insulin resistance. Elevated serum uric acid (SUA) independently predicts the future development of type 2 diabetes in prospective cohorts.1,2,7 Mechanistically, uric acid impairs insulin signaling through multiple pathways: it suppresses phosphorylation of insulin receptor substrate-1 (IRS-1), reduces glucose transporter-4 (GLUT4) translocation, and generates oxidative stress in insulin-sensitive tissues including adipose and skeletal muscle.1-3
Conversely, insulin resistance and hyperinsulinemia reduce renal urate clearance by increasing proximal tubular urate reabsorption via URAT1 activation, pushing SUA higher.1,3,4 Recent analyses of insulin resistance indices, such as the metabolic score for insulin resistance and the triglyceride-glucose index, demonstrate strong dose-response relationships between worsening insulin resistance and both hyperuricemia and non-alcoholic fatty liver disease (NAFLD), supporting the concept that uric acid sits centrally within a broader hepatic–metabolic–renal network of dysfunction.4,5
For podiatrists, this means that gout in a patient with prediabetes or established diabetes should be interpreted as a clinical clue to significant underlying insulin resistance and cardiometabolic instability, not simply as a stand-alone rheumatologic problem.1,2,5
In a patient presenting with gout who does not report a history of diabetes, the podiatrist should still actively consider this as a potential concomitant diagnosis, as cohort data suggest that diabetes mellitus is present in roughly 16% of individuals with gout, indicating that many either already have diabetes or are at risk for developing it.7 This supports asking about classic and subtle diabetes symptoms (polyuria, polydipsia, unexplained weight change, fatigue, prior gestational diabetes), asking about a family history of type 2 diabetes or metabolic syndrome, and considering point-of-care or laboratory testing (fasting glucose and hemoglobin A1c).
The Diabetic Foot With Concurrent Gout: Multiplied Risk
Patients with diabetes and gout face compounded metabolic and limb-threatening risks. A podiatric patient presenting with gout, central obesity, elevated blood pressure, and abnormal glucose tolerance (or overt diabetes) is broadcasting an exceptionally high cardiometabolic risk state that demands early recognition and aggressive intervention.1,2,5
For older patients with diabetes and foot complications such as neuropathy, ulceration, or prior amputation, the presence of concurrent gout adds another layer of metabolic instability and substantially elevates overall mortality risk.5,6 Both gout and diabetes promote oxidative stress, vascular inflammation, and endothelial dysfunction, amplifying macrovascular disease (peripheral arterial disease) and microvascular complications that directly impact wound healing and limb preservation.2,5,6
At the same time, neuropathy and impaired immune response in diabetes mean that infection may present subtly—sometimes mimicking or coexisting with gout—placing the podiatrist in a critical diagnostic position.
Gout Flare or Infection? Diagnostic Caution in the Diabetic Foot
One of the most dangerous pitfalls in this population is assuming that a hot, swollen joint is "just gout." Patients with diabetes are at high risk for serious infection, including cellulitis, septic arthritis, osteomyelitis, and necrotizing soft tissue infection, and these entities can present with warmth, erythema, swelling, and pain that overlap with gout.5,6
In an individual with diabetes and known hyperuricemia or gout, it is easy (and dangerous) to anchor on that diagnosis. A missed or delayed diagnosis of infection in such a patient can result in rapid progression to sepsis or amputation. Clinically, several features should raise concern for infection rather than (or in addition to) gout: systemic signs (fever, chills, malaise), rapidly spreading erythema, skin breakdown or ulceration, purulence, foul odor, lymphangitic streaking, severe tenderness out of proportion to prior gout flares, or pain extending beyond a single joint.5,6
From a diagnostic standpoint, inflammatory markers (erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), white blood cell count) can be elevated in both gout and infection, but markedly elevated values, systemic toxicity, or hemodynamic instability should lower the threshold for urgent hospital admission.5,6 Intra-articular aspiration with crystal analysis and culture remains the gold standard when septic arthritis is a concern; in the diabetic foot, aspiration or biopsy may be critical when clinical findings are ambiguous. When in doubt, especially in a neuropathic or immunocompromised patient, it is often safest to assume infection until it is convincingly excluded, rather than the reverse.
Clinical Screening and Risk Stratification in the Podiatry Office
History assessment. A focused history should document the patient's HbA1c, frequency and character of prior gout flares, and presence of hypertension, dyslipidemia, chronic kidney disease, or prior cardiovascular events.1,2,5 Critically, any history of foot ulcers, prior infections, or amputations substantially raises the risk of serious infection in any new episode of foot swelling or warmth and must inform the differential diagnosis.5,6
Physical examination. Vital signs and body mass index should be recorded. Assessment for diabetic neuropathy and peripheral pulses is essential. Careful inspection for skin breaks, ulcers, purulence, crepitus, rapidly spreading erythema, lymphangitic streaking, or foul odor must take place; these findings indicate infection rather than gout.5,6
Laboratory screening. Generally, the podiatrist should order serum uric acid, fasting glucose, hemoglobin A1c, a lipid panel, a basic metabolic panel with creatinine and estimated glomerular filtration rate (GFR), and a urinalysis.8 When infection is suspected, order ESR, CRP, and complete blood count, recognizing that normal values do not exclude deep infection in patients with diabetes.5,6 Plain radiographs should be obtained; magnetic resonance imaging (MRI) or ultrasound may be needed if one suspects osteomyelitis or deep abscess.
Red flag scenarios requiring urgent attention. While acute gout typically peaks within 24–48 hours and begins to improve over several days, with most untreated flares resolving over about 7–10 days, persistent or worsening erythema, edema, and pain beyond this expected trajectory should shift clinical suspicion more strongly toward infection rather than uncomplicated gout, especially in a patient with diabetes.5,6,9 Assuming gout in such a patient and delaying antibiotics or infection work-up could result in a limb- or life-threatening situation.
Lifestyle and pharmacologic management. For patients with diabetes and gout, weight loss of 5–10 percent reduces serum uric acid (SUA), improves glucose control, and lowers blood pressure.1,8,9 Dietary reduction of fructose and sugar-sweetened beverages, along with emphasis on lower-glycemic carbohydrates and moderate alcohol restriction, supports both gout control and metabolic health.1,9 Urate-lowering therapy—typically allopurinol—should be dosed carefully for kidney function and titrated to target SUA below 6 mg/dL.9,11 In patients with chronic kidney disease (CKD), renal function monitoring is essential. Intensive glycemic control reduces diabetic foot complications, infection risk, and cardiovascular events, requiring close coordination with endocrinology or primary care.9 When managing acute flares, avoid corticosteroids and NSAIDs in favor of low-dose colchicine when renal function permits.11
The Podiatrist's Role as Metabolic and Infectious Risk Screener
Podiatrists who see patients with diabetes and gout are uniquely positioned to serve as front-line assessors of both metabolic and infectious risk. By asking targeted questions about blood sugar control, blood pressure, lipids, cardiovascular symptoms, and infection warning signs—and by documenting concerns about concurrent gout, diabetes, and metabolic syndrome in clear, actionable language—podiatrists can prompt earlier and more aggressive intervention by the broader medical team.1,2,5,6
Equally, by refusing to assume that every hot, swollen diabetic foot is "just gout" and maintaining a low threshold for evaluating and treating infection, podiatrists can prevent devastating delays in the diagnosis of cellulitis, septic arthritis, or osteomyelitis. Early recognition of this high-risk phenotype, coupled with coordinated care and diagnostic caution, can meaningfully reduce both systemic complications and limb loss.
Conclusion
Gout in a patient with diabetes is never "just gout." It is a window into a deeper cardiometabolic derangement and, in the foot, a setting where infection can masquerade as gout or coexist with it. By recognizing gout as a marker of insulin resistance, metabolic syndrome, and amplified diabetic risk—and by rigorously excluding infection in any hot, swollen diabetic foot—podiatrists can transform the office visit into an opportunity for comprehensive risk stratification, safe diagnosis, and coordinated prevention. The inflamed foot, in the context of diabetes, speaks to what the entire body is struggling with and underscores the need to treat both the joint and the patient's systemic and infectious risks before irreversible damage occurs.1,2,5,6,8-10
Dr. Nirenberg is a podiatric physician and forensic podiatrist in practice for over 33 years. He is President of the American Society of Forensic Podiatry, serves on the Education Committee of the American College of Podiatric Medicine, and his state's Board of Podiatric Medicine.
The author has no financial, commercial, or proprietary interests, and no relevant non-financial relationships to disclose for this content. The author did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
References
- Singh JA, Gaffo A. Gout epidemiology and comorbidities. Semin Arthritis Rheum. 2020;50(3):S11-S16.
- Kuwabara M, Niwa K, Hisatome I, et al. Hyperuricemia and its related diseases: mechanisms and advances in management. Signal Transduct Target Ther. 2024;9(1):212.
- Chino Y, Samukawa Y, Sakai S, et al. Insulin stimulates uric acid reabsorption via regulating urate transporters in the kidney. Am J Physiol Renal Physiol. 2017;313(3):F826-F834.
- Shu Y, Huang G, Mao Y. The metabolic score for insulin resistance index is superior to the triglyceride and glucose index in identifying nonalcoholic fatty liver disease in hyperuricemia subjects. Diabetes Metab Syndr Obes. 2023;16:4235-4246. Published December 28, 2023.
- Jain R, Gupta A, Verma S, et al. Association of hyperuricemia with cardiovascular diseases: an updated review. Curr Med Res Opin. 2023;39(3):391-402.
- Xie H, et al. Associations of elevated cardiac biomarkers with hyperuricemia and mortality in US adults without prevalent cardiovascular disease. Front Endocrinol (Lausanne). 2024;15:1432200.
- Zhao R, Wang Y, Fu T, Zhou W, Ge X, Sha X, et al. Gout and risk of diabetes mellitus: meta-analysis of observational studies. Psychol Health Med. 2020;25(8):917-930.
- Çakir O, Yıldırım B, Öztürk K, et al. Association between vitamin D and uric acid in adults: a systematic review and meta-analysis. Nutrients. 2020;12(10):3150.
- Collier A, Stirling A, Cameron L, Hair M, Crosbie D. Gout and diabetes: a common combination. Postgrad Med J. 2016;92(1089):372-378.
- FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020;72(6):744-760.
- American College of Rheumatology. Press release: ACR releases gout management guideline with emphasis on treat-to-target strategy for urate-lowering therapy. Published May 11, 2020. Accessed April 24, 2026. Available at https://rheumatology.org/press-releases/acr-releases-gout-management-guideline-with-emphasis-on-treat-to-target-strategy-for-urate-lowering-therapy.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






