Spesolimab Shows Potential in Treating GPP With Palmoplantar Pustulosis
Spesolimab, an interleukin-36 (IL-36) receptor antagonist, may offer an effective treatment option for patients with generalized pustular psoriasis (GPP) complicated by palmoplantar pustulosis (PPP), according to a case report evaluating its clinical use in this rare overlap presentation. The findings add to growing evidence supporting IL-36–targeted therapy in pustular psoriasis variants.
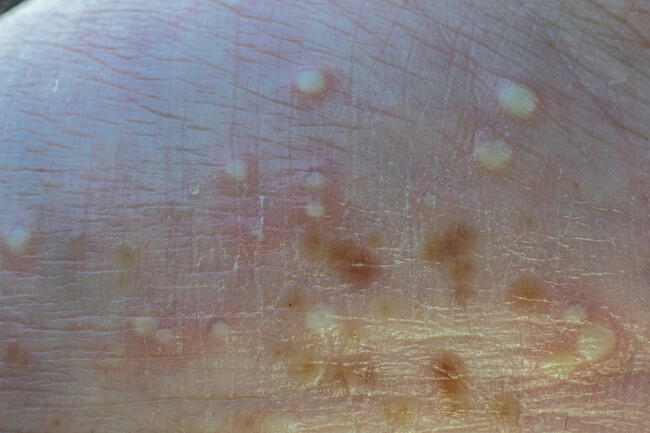
GPP is a severe, potentially life-threatening inflammatory skin condition driven by dysregulated IL-36 signaling. While spesolimab has demonstrated efficacy in GPP, data on its use in patients with concurrent PPP remain limited. PPP is characterized by chronic pustular lesions on the palms and soles and may represent a distinct or overlapping inflammatory pathway.
In this report, a patient with GPP and PPP was treated with spesolimab and experienced significant clinical improvement. Skin lesions improved substantially following treatment, with no reported safety concerns during the observation period. The authors noted that “spesolimab has good clinical efficacy in treating GPP combined with PPP,” supporting its potential use in complex disease presentations.
However, the presence of PPP appeared to influence response dynamics. The authors observed that “the presence of PPP may have delayed the rapid and complete clearance of the skin lesions,” suggesting that overlapping disease mechanisms may affect treatment kinetics.
No significant adverse effects were reported, reinforcing the tolerability of IL-36 inhibition in this case. While limited by its single-patient design, the report highlights an area of unmet need in managing patients with combined pustular phenotypes.
The authors concluded that “spesolimab provides a new treatment option for patients with GPP combined with PPP.”
Reference
Tan H, Zhang Y, Zhang B, et al. IL-36 receptor antagonist spesolimab for generalized pustular psoriasis combined with palmoplantar pustulosis: a case report. Clin Cosmet Investig Dermatol. 2026;19:568455. doi:10.2147/CCID.S568455