This is the final article of a series on billing and coding for dermatologists. This article will discuss proper coding and documentation for inpatient dermatology and basic coding for interpreting pathology slides.
 Dermatopathology
Dermatopathology
Many private practice physicians read their own dermatopathology slides, thereby requiring a working knowledge of the appropriate pathology codes. Pathology slides have 2 basic components: a technical component (TC) and a professional component (PC). The TC billing includes the transportation and preparation of the slides, while the PC billing includes interpreting the slide and providing a diagnosis. Pathology codes may be billed globally as a single code, or the 2 components may be billed separately with the appropriate modifiers. The TC and PC components do not have to be performed at the same location.
The 2 most common PC Current Procedural Terminology (CPT) codes used in dermatopathology are 88304 and 88305. The code 88304 is used to bill for the diagnosis of cysts, skin tags, lipomas, and debridement materials. The code 88305 is used to bill for almost all other specimens, including biopsies  and excisions. The code 88307 is used for billing lymph node dissections or sentinel lymph node slides. Evaluation of pathologic specimens using frozen section histology is billed using 88331 or 88332. Frozen section margin control intrinsic to Mohs surgery is included in the Mohs surgery base codes and should not be reported separately. For multiple biopsies in the same container, the pathologist can only code 1 professional CPT. For multiple biopsies in different containers from the same patient, the pathologist should list these as A, B, C, etc. and each one will receive its own PC code. Coding for dermatopathology stains and for consultation slides are delineated in Table 1 and Table 2, respectively.
and excisions. The code 88307 is used for billing lymph node dissections or sentinel lymph node slides. Evaluation of pathologic specimens using frozen section histology is billed using 88331 or 88332. Frozen section margin control intrinsic to Mohs surgery is included in the Mohs surgery base codes and should not be reported separately. For multiple biopsies in the same container, the pathologist can only code 1 professional CPT. For multiple biopsies in different containers from the same patient, the pathologist should list these as A, B, C, etc. and each one will receive its own PC code. Coding for dermatopathology stains and for consultation slides are delineated in Table 1 and Table 2, respectively.
Inpatient Coding and Documentation
Dermatology has traditionally been an outpatient specialty, but with recent emphasis on quality of care and cost savings, dermatologists may become an increasingly utilized specialty within inpatient medicine. Due to the difference in billing and coding between outpatient and inpatient services, the dermatologist should have a basic working knowledge of inpatient coding in order to be properly reimbursed for their service. There are 2 basic scenarios for dermatology documentation within the hospital setting: managing a primary dermatology inpatient or performing a consultation on an inpatient.
Hospitals may have a dermatology service where patients are primarily managed by dermatologists. For these patients, the physician needs to understand how to document and bill for hospital admissions, daily progress notes, and discharges. Hospital admissions can be performed in the outpatient or inpatient setting. If a patient is seen in clinic with plans to directly admit to the hospital, a 99215 comprehensive outpatient visit can be submitted in place of a hospital admission code. For review, a 99215 would require 2 of the following: history (4+ elements, complete review of systems, 2+ past history elements), physical exam (at least 2 bullet points from 9 different organ systems), or medical decision-making (severe complexity). If a patient admission is performed in a hospital setting, a different set of Evaluation/Management (E/M) codes are used (Table 3). For these admission codes, all 3 components must be met to code at a certain level, as opposed to return outpatient E/M codes.
 Daily progress notes for inpatients have their own coding series and similar to follow-up office visits only require 2 of the 3 components to be met in order to justify the level of billing. These codes should be used for patient encounters beginning the day after admission. Providers should be wary of under-coding progress notes as these notes do not require extensive documentation. Table 4 includes E/M codes for inpatient progress notes.
Daily progress notes for inpatients have their own coding series and similar to follow-up office visits only require 2 of the 3 components to be met in order to justify the level of billing. These codes should be used for patient encounters beginning the day after admission. Providers should be wary of under-coding progress notes as these notes do not require extensive documentation. Table 4 includes E/M codes for inpatient progress notes.
Hospital Discharge Day Management Services codes are used to report the total amount of time spent by the physician for final discharge of a patient. These codes, as appropriate, include final examination of the patient, discussion of the hospital stay even if the time spent is not continuous, instructions for continuing care to all relevant caregivers, and preparation of discharge records, prescriptions, and referral forms. The provider must document the time spent on the discharge to justify the appropriate code. The E/M code for a hospital discharge less than 30 minutes is 99238, and 99239 is the code for a discharge requiring more than 30 minutes.
Article continues on page 2
{{pagebreak}}
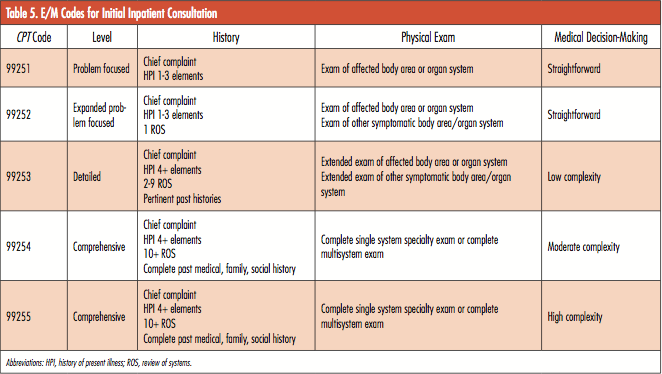
Initial inpatient consultation codes are used for the initial patient consult visit and require all 3 visit components at the same level to justify a higher level of billing (Table 5). This is similar to hospital admissions and new outpatient office visits. Follow-up inpatient consultation codes (99262, 99263) are only used either when concluding initial consultative services or when subsequent requests are made by the attending physician for further consultative visits during the same inpatient stay. The 2005 CPT manual states, “If the physician consultant has initiated treatment at the [time of the] initial consultation, and participates thereafter in the patient’s management, the codes for subsequent hospital care should be used (99231-99233).” Medicare does not reimburse for inpatient or outpatient consultation codes. If a provider is seeing a Medicare patient as a consult, the provider should use the new or established patient E/M codes for inpatients or outpatients to be reimbursed for services.
If a teaching physician is supervising a resident performing the consultation service, the teaching physician should sign the written report and a personal notation made on the report concerning the teaching physician’s participation in the 3 key components of the consultation (ie, history, physical examination, and medical decision-making). The resident’s note should reflect that the teaching physician was present and participated in the key components of the consultation.
If a patient is seen in the emergency department (ED) as a consult, the coding differs as to whether they are insured by Medicare or a private agency. If the patient is insured by Medicare, the provider should use consult codes specific to the ED (99281-99285). If the patient is non-Medicare, the provider should use the outpatient consultation code series (99241-99245).
Conclusion
Providers need to possess knowledge of E/M codes, procedure codes, and the necessary documentation to support their coding practices. Learning the nuances of this process and mastering the many rules of appropriate billing and coding can be intimidating. Frequent review of the rules, performing self-audits, and keeping updated on new coding issues will all serve to increase provider confidence and avoid external audits while maximizing revenue.
This coding series is meant to serve as a quick reference for dermatologists to help providers understand basic concepts of dermatology billing, coding, and documentation. It is not meant to be a comprehensive coding resource but rather to focus on the issues commonly encountered within dermatology.
There are many existing resources that provide more comprehensive billing and coding rules. Providers can find complete listings of the different coding systems on the Centers for Medicare & Medicaid Services website (www.cms.gov/Medicare/Medicare.html). The American Medical Association also publishes a coding resource which providers can purchase, and has multiple online resources (www.ama-assn.org). The American Academy of Dermatology publishes paperback books, e-books, and online modules dedicated to billing and coding (www.aad.org).
This is the final article of a series on billing and coding for dermatologists. This article will discuss proper coding and documentation for inpatient dermatology and basic coding for interpreting pathology slides.
 Dermatopathology
Dermatopathology
Many private practice physicians read their own dermatopathology slides, thereby requiring a working knowledge of the appropriate pathology codes. Pathology slides have 2 basic components: a technical component (TC) and a professional component (PC). The TC billing includes the transportation and preparation of the slides, while the PC billing includes interpreting the slide and providing a diagnosis. Pathology codes may be billed globally as a single code, or the 2 components may be billed separately with the appropriate modifiers. The TC and PC components do not have to be performed at the same location.
The 2 most common PC Current Procedural Terminology (CPT) codes used in dermatopathology are 88304 and 88305. The code 88304 is used to bill for the diagnosis of cysts, skin tags, lipomas, and debridement materials. The code 88305 is used to bill for almost all other specimens, including biopsies  and excisions. The code 88307 is used for billing lymph node dissections or sentinel lymph node slides. Evaluation of pathologic specimens using frozen section histology is billed using 88331 or 88332. Frozen section margin control intrinsic to Mohs surgery is included in the Mohs surgery base codes and should not be reported separately. For multiple biopsies in the same container, the pathologist can only code 1 professional CPT. For multiple biopsies in different containers from the same patient, the pathologist should list these as A, B, C, etc. and each one will receive its own PC code. Coding for dermatopathology stains and for consultation slides are delineated in Table 1 and Table 2, respectively.
and excisions. The code 88307 is used for billing lymph node dissections or sentinel lymph node slides. Evaluation of pathologic specimens using frozen section histology is billed using 88331 or 88332. Frozen section margin control intrinsic to Mohs surgery is included in the Mohs surgery base codes and should not be reported separately. For multiple biopsies in the same container, the pathologist can only code 1 professional CPT. For multiple biopsies in different containers from the same patient, the pathologist should list these as A, B, C, etc. and each one will receive its own PC code. Coding for dermatopathology stains and for consultation slides are delineated in Table 1 and Table 2, respectively.
Inpatient Coding and Documentation
Dermatology has traditionally been an outpatient specialty, but with recent emphasis on quality of care and cost savings, dermatologists may become an increasingly utilized specialty within inpatient medicine. Due to the difference in billing and coding between outpatient and inpatient services, the dermatologist should have a basic working knowledge of inpatient coding in order to be properly reimbursed for their service. There are 2 basic scenarios for dermatology documentation within the hospital setting: managing a primary dermatology inpatient or performing a consultation on an inpatient.
Hospitals may have a dermatology service where patients are primarily managed by dermatologists. For these patients, the physician needs to understand how to document and bill for hospital admissions, daily progress notes, and discharges. Hospital admissions can be performed in the outpatient or inpatient setting. If a patient is seen in clinic with plans to directly admit to the hospital, a 99215 comprehensive outpatient visit can be submitted in place of a hospital admission code. For review, a 99215 would require 2 of the following: history (4+ elements, complete review of systems, 2+ past history elements), physical exam (at least 2 bullet points from 9 different organ systems), or medical decision-making (severe complexity). If a patient admission is performed in a hospital setting, a different set of Evaluation/Management (E/M) codes are used (Table 3). For these admission codes, all 3 components must be met to code at a certain level, as opposed to return outpatient E/M codes.
 Daily progress notes for inpatients have their own coding series and similar to follow-up office visits only require 2 of the 3 components to be met in order to justify the level of billing. These codes should be used for patient encounters beginning the day after admission. Providers should be wary of under-coding progress notes as these notes do not require extensive documentation. Table 4 includes E/M codes for inpatient progress notes.
Daily progress notes for inpatients have their own coding series and similar to follow-up office visits only require 2 of the 3 components to be met in order to justify the level of billing. These codes should be used for patient encounters beginning the day after admission. Providers should be wary of under-coding progress notes as these notes do not require extensive documentation. Table 4 includes E/M codes for inpatient progress notes.
Hospital Discharge Day Management Services codes are used to report the total amount of time spent by the physician for final discharge of a patient. These codes, as appropriate, include final examination of the patient, discussion of the hospital stay even if the time spent is not continuous, instructions for continuing care to all relevant caregivers, and preparation of discharge records, prescriptions, and referral forms. The provider must document the time spent on the discharge to justify the appropriate code. The E/M code for a hospital discharge less than 30 minutes is 99238, and 99239 is the code for a discharge requiring more than 30 minutes.
Article continues on page 2
{{pagebreak}}
Initial inpatient consultation codes are used for the initial patient consult visit and require all 3 visit components at the same level to justify a higher level of billing (Table 5). This is similar to hospital admissions and new outpatient office visits. Follow-up inpatient consultation codes (99262, 99263) are only used either when concluding initial consultative services or when subsequent requests are made by the attending physician for further consultative visits during the same inpatient stay. The 2005 CPT manual states, “If the physician consultant has initiated treatment at the [time of the] initial consultation, and participates thereafter in the patient’s management, the codes for subsequent hospital care should be used (99231-99233).” Medicare does not reimburse for inpatient or outpatient consultation codes. If a provider is seeing a Medicare patient as a consult, the provider should use the new or established patient E/M codes for inpatients or outpatients to be reimbursed for services.
If a teaching physician is supervising a resident performing the consultation service, the teaching physician should sign the written report and a personal notation made on the report concerning the teaching physician’s participation in the 3 key components of the consultation (ie, history, physical examination, and medical decision-making). The resident’s note should reflect that the teaching physician was present and participated in the key components of the consultation.
If a patient is seen in the emergency department (ED) as a consult, the coding differs as to whether they are insured by Medicare or a private agency. If the patient is insured by Medicare, the provider should use consult codes specific to the ED (99281-99285). If the patient is non-Medicare, the provider should use the outpatient consultation code series (99241-99245).
Conclusion
Providers need to possess knowledge of E/M codes, procedure codes, and the necessary documentation to support their coding practices. Learning the nuances of this process and mastering the many rules of appropriate billing and coding can be intimidating. Frequent review of the rules, performing self-audits, and keeping updated on new coding issues will all serve to increase provider confidence and avoid external audits while maximizing revenue.
This coding series is meant to serve as a quick reference for dermatologists to help providers understand basic concepts of dermatology billing, coding, and documentation. It is not meant to be a comprehensive coding resource but rather to focus on the issues commonly encountered within dermatology.
There are many existing resources that provide more comprehensive billing and coding rules. Providers can find complete listings of the different coding systems on the Centers for Medicare & Medicaid Services website (www.cms.gov/Medicare/Medicare.html). The American Medical Association also publishes a coding resource which providers can purchase, and has multiple online resources (www.ama-assn.org). The American Academy of Dermatology publishes paperback books, e-books, and online modules dedicated to billing and coding (www.aad.org).

This is the final article of a series on billing and coding for dermatologists. This article will discuss proper coding and documentation for inpatient dermatology and basic coding for interpreting pathology slides.
Dermatopathology
Many private practice physicians read their own dermatopathology slides, thereby requiring a working knowledge of the appropriate pathology codes. Pathology slides have 2 basic components: a technical component (TC) and a professional component (PC). The TC billing includes the transportation and preparation of the slides, while the PC billing includes interpreting the slide and providing a diagnosis. Pathology codes may be billed globally as a single code, or the 2 components may be billed separately with the appropriate modifiers. The TC and PC components do not have to be performed at the same location.
The 2 most common PC Current Procedural Terminology (CPT) codes used in dermatopathology are 88304 and 88305. The code 88304 is used to bill for the diagnosis of cysts, skin tags, lipomas, and debridement materials. The code 88305 is used to bill for almost all other specimens, including biopsies and excisions. The code 88307 is used for billing lymph node dissections or sentinel lymph node slides. Evaluation of pathologic specimens using frozen section histology is billed using 88331 or 88332. Frozen section margin control intrinsic to Mohs surgery is included in the Mohs surgery base codes and should not be reported separately. For multiple biopsies in the same container, the pathologist can only code 1 professional CPT. For multiple biopsies in different containers from the same patient, the pathologist should list these as A, B, C, etc. and each one will receive its own PC code. Coding for dermatopathology stains and for consultation slides are delineated in Table 1 and Table 2, respectively.
Inpatient Coding and Documentation
Dermatology has traditionally been an outpatient specialty, but with recent emphasis on quality of care and cost savings, dermatologists may become an increasingly utilized specialty within inpatient medicine. Due to the difference in billing and coding between outpatient and inpatient services, the dermatologist should have a basic working knowledge of inpatient coding in order to be properly reimbursed for their service. There are 2 basic scenarios for dermatology documentation within the hospital setting: managing a primary dermatology inpatient or performing a consultation on an inpatient.
Hospitals may have a dermatology service where patients are primarily managed by dermatologists. For these patients, the physician needs to understand how to document and bill for hospital admissions, daily progress notes, and discharges. Hospital admissions can be performed in the outpatient or inpatient setting. If a patient is seen in clinic with plans to directly admit to the hospital, a 99215 comprehensive outpatient visit can be submitted in place of a hospital admission code. For review, a 99215 would require 2 of the following: history (4+ elements, complete review of systems, 2+ past history elements), physical exam (at least 2 bullet points from 9 different organ systems), or medical decision-making (severe complexity). If a patient admission is performed in a hospital setting, a different set of Evaluation/Management (E/M) codes are used (Table 3). For these admission codes, all 3 components must be met to code at a certain level, as opposed to return outpatient E/M codes.
Daily progress notes for inpatients have their own coding series and similar to follow-up office visits only require 2 of the 3 components to be met in order to justify the level of billing. These codes should be used for patient encounters beginning the day after admission. Providers should be wary of under-coding progress notes as these notes do not require extensive documentation. Table 4 includes E/M codes for inpatient progress notes.
Hospital Discharge Day Management Services codes are used to report the total amount of time spent by the physician for final discharge of a patient. These codes, as appropriate, include final examination of the patient, discussion of the hospital stay even if the time spent is not continuous, instructions for continuing care to all relevant caregivers, and preparation of discharge records, prescriptions, and referral forms. The provider must document the time spent on the discharge to justify the appropriate code. The E/M code for a hospital discharge less than 30 minutes is 99238, and 99239 is the code for a discharge requiring more than 30 minutes.
Article continues on page 2
{{pagebreak}}
Initial inpatient consultation codes are used for the initial patient consult visit and require all 3 visit components at the same level to justify a higher level of billing (Table 5). This is similar to hospital admissions and new outpatient office visits. Follow-up inpatient consultation codes (99262, 99263) are only used either when concluding initial consultative services or when subsequent requests are made by the attending physician for further consultative visits during the same inpatient stay. The 2005 CPT manual states, “If the physician consultant has initiated treatment at the [time of the] initial consultation, and participates thereafter in the patient’s management, the codes for subsequent hospital care should be used (99231-99233).” Medicare does not reimburse for inpatient or outpatient consultation codes. If a provider is seeing a Medicare patient as a consult, the provider should use the new or established patient E/M codes for inpatients or outpatients to be reimbursed for services.
If a teaching physician is supervising a resident performing the consultation service, the teaching physician should sign the written report and a personal notation made on the report concerning the teaching physician’s participation in the 3 key components of the consultation (ie, history, physical examination, and medical decision-making). The resident’s note should reflect that the teaching physician was present and participated in the key components of the consultation.
If a patient is seen in the emergency department (ED) as a consult, the coding differs as to whether they are insured by Medicare or a private agency. If the patient is insured by Medicare, the provider should use consult codes specific to the ED (99281-99285). If the patient is non-Medicare, the provider should use the outpatient consultation code series (99241-99245).
Conclusion
Providers need to possess knowledge of E/M codes, procedure codes, and the necessary documentation to support their coding practices. Learning the nuances of this process and mastering the many rules of appropriate billing and coding can be intimidating. Frequent review of the rules, performing self-audits, and keeping updated on new coding issues will all serve to increase provider confidence and avoid external audits while maximizing revenue.
This coding series is meant to serve as a quick reference for dermatologists to help providers understand basic concepts of dermatology billing, coding, and documentation. It is not meant to be a comprehensive coding resource but rather to focus on the issues commonly encountered within dermatology.
There are many existing resources that provide more comprehensive billing and coding rules. Providers can find complete listings of the different coding systems on the Centers for Medicare & Medicaid Services website (www.cms.gov/Medicare/Medicare.html). The American Medical Association also publishes a coding resource which providers can purchase, and has multiple online resources (www.ama-assn.org). The American Academy of Dermatology publishes paperback books, e-books, and online modules dedicated to billing and coding (www.aad.org).