
A 68-year-old male presented for evaluation of an itchy rash on his back. The rash began 1 year ago and has spread to his buttocks and thighs. He has been using topical triamcinolone 0.1%, which has helped. He has no prior history of eczema. He began taking simvastatin and metformin approximately 1 year ago.
On physical examination, there were several well-demarcated, oval patches and thin plaques with overlying desquamative scale (Figure 1). The lesions ranged from 2 cm to 8 cm in size and blue-brown in color. They were distributed over the patient’s lower back, buttocks, and thighs (Figure 2). There were no plaques present on his face, arms, lower legs, or hands. A biopsy was performed.
What's Your Diagnosis?
Answer on page 2
{{pagebreak}}
Diagnosis: Patch-phase Mycosis Fungoides
Mycosis fungoides (MF) is characterized by patches, plaques, and tumors involving photoprotected areas such as the trunk and buttocks (Figures 1 and 2). MF generally has an indolent course and good prognosis in the early stages.1-3
The patch phase involves a thin, yellowish-red, brownish, or violaceous eczema-like rash. There can be thin scaling with slight atrophy. Lesions are irregular in shape and symmetric in distribution. The differential diagnosis for  these patch-stage lesions includes psoriasis, contact dermatitis, atopic dermatitis, ashy dermatosis, and parapsoriasis. The clinical appearance of psoriasis will also have well-demarcated patches and plaques albeit with thicker, silvery scale, frequent nail involvement, and a distribution favoring the scalp, knee, elbow, and intergluteal cleft. Atopic and contact dermatitis morphology can sometimes include well-demarcated lichenified plaques with thin scale. Ashy dermatosis patients will present with well-demarcated macules and patches of varying shape on the face, neck, and trunk, but these will be gray in color. It more frequently affects darker-skinned individuals. Parapsoriasis, characterized by salmon-colored patches with slight scale, is considered by many to be a precursor to MF. These lesions may evolve to become indurated, elevated, and pruritic.1-4
these patch-stage lesions includes psoriasis, contact dermatitis, atopic dermatitis, ashy dermatosis, and parapsoriasis. The clinical appearance of psoriasis will also have well-demarcated patches and plaques albeit with thicker, silvery scale, frequent nail involvement, and a distribution favoring the scalp, knee, elbow, and intergluteal cleft. Atopic and contact dermatitis morphology can sometimes include well-demarcated lichenified plaques with thin scale. Ashy dermatosis patients will present with well-demarcated macules and patches of varying shape on the face, neck, and trunk, but these will be gray in color. It more frequently affects darker-skinned individuals. Parapsoriasis, characterized by salmon-colored patches with slight scale, is considered by many to be a precursor to MF. These lesions may evolve to become indurated, elevated, and pruritic.1-4
On histopathology, patch stage lesions classically demonstrate epidermotropism of cerebriform lymphocytes and a lymphocytic infiltrate at the edges of the basal layer. Many inflammatory dermatoses share histopathological features with early stage MF including scattered epidermal lymphocytes and papillary dermal fibrosis. This can make early diagnosis difficult. Clonal rearrangements of the T-cell receptor (TCR) gene detected by polymerase chain reaction or Southern blot analysis provide additional support for MF diagnosis.1,3,5,6
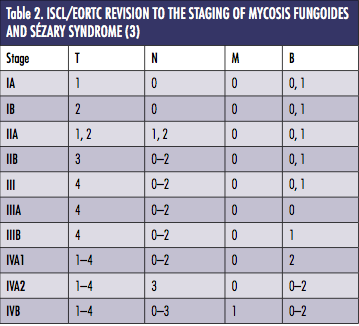
The classification and staging of MF as a result of the International Society for Cutaneous Lymphomas/European Organization of Research and Treatment of Cancer discussions is shown in Tables 1 and 2. The case presented is classified as stage IA (T1a N0 M0 B0) based on this system.7
 Epidemiology
Epidemiology
MF is the most common type of cutaneous T-cell lymphoma and accounts for approximately 54% of cases. In the United States, the incidence is 0.36 cases/100,000 inhabitants and is higher in black population than in the White population. In an National Health Service study of 1500 MF patients from 1990 to 2009, the median age of diagnosis was 54 years with a male to female ratio of 1.6:1. Of the patients, 71% had T1 or T2 stage at diagnosis. Two-thirds (295/443) of T1 stage patients had only T1a disease.3,6
Treatment
Options for treatment of early-stage MF include topical corticosteroids and psoralen–UVA (PUVA) or UVB for more widely distributed disease. In patients with limited patch-stage disease as presented in this case, topical steroids alone can control the eruption. There is a 63% complete response rate using topical steroids in patients with T1 stage disease and a 31% partial response rate. PUVA is similarly effective, with complete and overall response rates reaching 58% to 83% and 95%, respectively. PUVA is well tolerated, but long-term side effects include actinic damage and increased rate of skin malignancies. UVB radiation has a lower response rate than PUVA, but it is more widely available and does not require the use of psoralen.8,9
Topical nitrogen mustard is another option, with response rates comparable to topical steroids and PUVA for T1 stage disease. Patients frequently experience contact dermatitis while being treated with topical nitrogen mustard and, rarely, nonmelanoma skin cancer. Electron beam therapy is also highly effective for early-stage MF, with overall response rates reaching 100% and complete clinical response occurring in 75% of T2 stage disease patients. Most patients receiving electron beam therapy experience radiation-induced nail dystrophy, alopecia, dermatitis, and xerosis.10,11
Our Patient
Two 4 mm punch biopsies were performed from plaques on the patient’s right flank and left thigh. Both specimens showed interface dermatitis, epidermotropism, and a superficial perivascular lymphocytic infiltrate. TCR gene rearrangement test via polymerase chain reaction demonstrated a dominant monoclonal rearrangement from one tissue block. The patient was prescribed topical fluocinonide 0.05% ointment to be used twice daily. Follow-up at 4 months revealed modest improvement in existing lesions and no new lesions.
Conclusion
Early-stage MF can present as patches on the buttocks and thighs as highlighted in this case. The diagnosis and staging of MF can be complex and challenging, but is necessary in order to initiate safe, appropriate, and effective therapy.
Mr. Zubair is a student at Georgetown University School of Medicine in Washington, DC.
Dr. Aziz is staff dermatologist at Washington DC Veterans Affairs Medical Center and assistant professor of dermatology at Howard University in Washington, DC.
Disclosure: Mr. Zubair reports no relevant financial relationships.
Dr. Aziz is employed by Howard University College of Medicine and Washington DC Veterans Affairs Medical Center.
References
1. Knapp CF, Mathew R, Messina JL, Lien MH. CD4/CD8 dual-positive mycosis fungoides: a previously unrecognized variant. Am J Dermatopathol. 2012;34(3):e37-39.
2. Schmidt C. Cutaneous T-cell lymphoma’s confounding nature. J Natl Cancer Inst. 2012;104(11):806-808.
3. Yamashita T, Abbade LP, Marques ME, Marques SA. Mycosis fungoides and Sézary syndrome: clinical, histopathological and immunohistochemical review and update. An Bras Dermatol. 2012;87(6):817-828.
4. Marks JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 5th ed. Philadelphia. PA: Elsevier Saunders; 2013.
5. Dalton SR, Chandler WM, Abuzeid M, et al. Eosinophils in mycosis fungoides: an uncommon finding in the patch and plaque stages. Am J Dermatopathol. 2012;34(6):586-591.
6. Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J Clin Oncol. 2010;28(31):4730-4739.
7. Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713-1722.
8. Prince HM, Whittaker S, Hoppe RT. How I treat mycosis fungoides and Sézary syndrome. Blood. 2009;114(20):4337-4353.
9. Zackheim HS, Kashani-Sabet M, Amin S. Topical corticosteroids for mycosis fungoides. Experience in 79 patients. Arch Dermatol. 1998;134(8):949-954.
10. Navi D, Riaz N, Levin YS, Sullivan NC, Kim YH, Hoppe RT. The Stanford University experience with conventional-dose, total skin electron-beam therapy in the treatment of generalized patch or plaque (T2) and tumor (T3) mycosis fungoides. Arch Dermatol. 2011;147(5):561-567.
11. Lindahl LM, Fenger-Gron M, Iversen L. Topical nitrogen mustard therapy in patients with mycosis fungoides or parapsoriasis. J Eur Acad Dermatol Venereol. 2013;27(2):163-168.

A 68-year-old male presented for evaluation of an itchy rash on his back. The rash began 1 year ago and has spread to his buttocks and thighs. He has been using topical triamcinolone 0.1%, which has helped. He has no prior history of eczema. He began taking simvastatin and metformin approximately 1 year ago.
On physical examination, there were several well-demarcated, oval patches and thin plaques with overlying desquamative scale (Figure 1). The lesions ranged from 2 cm to 8 cm in size and blue-brown in color. They were distributed over the patient’s lower back, buttocks, and thighs (Figure 2). There were no plaques present on his face, arms, lower legs, or hands. A biopsy was performed.
What's Your Diagnosis?
Answer on page 2
{{pagebreak}}
Diagnosis: Patch-phase Mycosis Fungoides
Mycosis fungoides (MF) is characterized by patches, plaques, and tumors involving photoprotected areas such as the trunk and buttocks (Figures 1 and 2). MF generally has an indolent course and good prognosis in the early stages.1-3
The patch phase involves a thin, yellowish-red, brownish, or violaceous eczema-like rash. There can be thin scaling with slight atrophy. Lesions are irregular in shape and symmetric in distribution. The differential diagnosis for  these patch-stage lesions includes psoriasis, contact dermatitis, atopic dermatitis, ashy dermatosis, and parapsoriasis. The clinical appearance of psoriasis will also have well-demarcated patches and plaques albeit with thicker, silvery scale, frequent nail involvement, and a distribution favoring the scalp, knee, elbow, and intergluteal cleft. Atopic and contact dermatitis morphology can sometimes include well-demarcated lichenified plaques with thin scale. Ashy dermatosis patients will present with well-demarcated macules and patches of varying shape on the face, neck, and trunk, but these will be gray in color. It more frequently affects darker-skinned individuals. Parapsoriasis, characterized by salmon-colored patches with slight scale, is considered by many to be a precursor to MF. These lesions may evolve to become indurated, elevated, and pruritic.1-4
these patch-stage lesions includes psoriasis, contact dermatitis, atopic dermatitis, ashy dermatosis, and parapsoriasis. The clinical appearance of psoriasis will also have well-demarcated patches and plaques albeit with thicker, silvery scale, frequent nail involvement, and a distribution favoring the scalp, knee, elbow, and intergluteal cleft. Atopic and contact dermatitis morphology can sometimes include well-demarcated lichenified plaques with thin scale. Ashy dermatosis patients will present with well-demarcated macules and patches of varying shape on the face, neck, and trunk, but these will be gray in color. It more frequently affects darker-skinned individuals. Parapsoriasis, characterized by salmon-colored patches with slight scale, is considered by many to be a precursor to MF. These lesions may evolve to become indurated, elevated, and pruritic.1-4
On histopathology, patch stage lesions classically demonstrate epidermotropism of cerebriform lymphocytes and a lymphocytic infiltrate at the edges of the basal layer. Many inflammatory dermatoses share histopathological features with early stage MF including scattered epidermal lymphocytes and papillary dermal fibrosis. This can make early diagnosis difficult. Clonal rearrangements of the T-cell receptor (TCR) gene detected by polymerase chain reaction or Southern blot analysis provide additional support for MF diagnosis.1,3,5,6
The classification and staging of MF as a result of the International Society for Cutaneous Lymphomas/European Organization of Research and Treatment of Cancer discussions is shown in Tables 1 and 2. The case presented is classified as stage IA (T1a N0 M0 B0) based on this system.7
 Epidemiology
Epidemiology
MF is the most common type of cutaneous T-cell lymphoma and accounts for approximately 54% of cases. In the United States, the incidence is 0.36 cases/100,000 inhabitants and is higher in black population than in the White population. In an National Health Service study of 1500 MF patients from 1990 to 2009, the median age of diagnosis was 54 years with a male to female ratio of 1.6:1. Of the patients, 71% had T1 or T2 stage at diagnosis. Two-thirds (295/443) of T1 stage patients had only T1a disease.3,6
Treatment
Options for treatment of early-stage MF include topical corticosteroids and psoralen–UVA (PUVA) or UVB for more widely distributed disease. In patients with limited patch-stage disease as presented in this case, topical steroids alone can control the eruption. There is a 63% complete response rate using topical steroids in patients with T1 stage disease and a 31% partial response rate. PUVA is similarly effective, with complete and overall response rates reaching 58% to 83% and 95%, respectively. PUVA is well tolerated, but long-term side effects include actinic damage and increased rate of skin malignancies. UVB radiation has a lower response rate than PUVA, but it is more widely available and does not require the use of psoralen.8,9
Topical nitrogen mustard is another option, with response rates comparable to topical steroids and PUVA for T1 stage disease. Patients frequently experience contact dermatitis while being treated with topical nitrogen mustard and, rarely, nonmelanoma skin cancer. Electron beam therapy is also highly effective for early-stage MF, with overall response rates reaching 100% and complete clinical response occurring in 75% of T2 stage disease patients. Most patients receiving electron beam therapy experience radiation-induced nail dystrophy, alopecia, dermatitis, and xerosis.10,11
Our Patient
Two 4 mm punch biopsies were performed from plaques on the patient’s right flank and left thigh. Both specimens showed interface dermatitis, epidermotropism, and a superficial perivascular lymphocytic infiltrate. TCR gene rearrangement test via polymerase chain reaction demonstrated a dominant monoclonal rearrangement from one tissue block. The patient was prescribed topical fluocinonide 0.05% ointment to be used twice daily. Follow-up at 4 months revealed modest improvement in existing lesions and no new lesions.
Conclusion
Early-stage MF can present as patches on the buttocks and thighs as highlighted in this case. The diagnosis and staging of MF can be complex and challenging, but is necessary in order to initiate safe, appropriate, and effective therapy.

Mr. Zubair is a student at Georgetown University School of Medicine in Washington, DC.
Dr. Aziz is staff dermatologist at Washington DC Veterans Affairs Medical Center and assistant professor of dermatology at Howard University in Washington, DC.
Disclosure: Mr. Zubair reports no relevant financial relationships.
Dr. Aziz is employed by Howard University College of Medicine and Washington DC Veterans Affairs Medical Center.
References
1. Knapp CF, Mathew R, Messina JL, Lien MH. CD4/CD8 dual-positive mycosis fungoides: a previously unrecognized variant. Am J Dermatopathol. 2012;34(3):e37-39.
2. Schmidt C. Cutaneous T-cell lymphoma’s confounding nature. J Natl Cancer Inst. 2012;104(11):806-808.
3. Yamashita T, Abbade LP, Marques ME, Marques SA. Mycosis fungoides and Sézary syndrome: clinical, histopathological and immunohistochemical review and update. An Bras Dermatol. 2012;87(6):817-828.
4. Marks JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 5th ed. Philadelphia. PA: Elsevier Saunders; 2013.
5. Dalton SR, Chandler WM, Abuzeid M, et al. Eosinophils in mycosis fungoides: an uncommon finding in the patch and plaque stages. Am J Dermatopathol. 2012;34(6):586-591.
6. Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J Clin Oncol. 2010;28(31):4730-4739.
7. Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713-1722.
8. Prince HM, Whittaker S, Hoppe RT. How I treat mycosis fungoides and Sézary syndrome. Blood. 2009;114(20):4337-4353.
9. Zackheim HS, Kashani-Sabet M, Amin S. Topical corticosteroids for mycosis fungoides. Experience in 79 patients. Arch Dermatol. 1998;134(8):949-954.
10. Navi D, Riaz N, Levin YS, Sullivan NC, Kim YH, Hoppe RT. The Stanford University experience with conventional-dose, total skin electron-beam therapy in the treatment of generalized patch or plaque (T2) and tumor (T3) mycosis fungoides. Arch Dermatol. 2011;147(5):561-567.
11. Lindahl LM, Fenger-Gron M, Iversen L. Topical nitrogen mustard therapy in patients with mycosis fungoides or parapsoriasis. J Eur Acad Dermatol Venereol. 2013;27(2):163-168.
A 68-year-old male presented for evaluation of an itchy rash on his back. The rash began 1 year ago and has spread to his buttocks and thighs. He has been using topical triamcinolone 0.1%, which has helped. He has no prior history of eczema. He began taking simvastatin and metformin approximately 1 year ago.
On physical examination, there were several well-demarcated, oval patches and thin plaques with overlying desquamative scale (Figure 1). The lesions ranged from 2 cm to 8 cm in size and blue-brown in color. They were distributed over the patient’s lower back, buttocks, and thighs (Figure 2). There were no plaques present on his face, arms, lower legs, or hands. A biopsy was performed.
What's Your Diagnosis?
Answer on page 2
{{pagebreak}}
Diagnosis: Patch-phase Mycosis Fungoides
Mycosis fungoides (MF) is characterized by patches, plaques, and tumors involving photoprotected areas such as the trunk and buttocks (Figures 1 and 2). MF generally has an indolent course and good prognosis in the early stages.1-3
The patch phase involves a thin, yellowish-red, brownish, or violaceous eczema-like rash. There can be thin scaling with slight atrophy. Lesions are irregular in shape and symmetric in distribution. The differential diagnosis for these patch-stage lesions includes psoriasis, contact dermatitis, atopic dermatitis, ashy dermatosis, and parapsoriasis. The clinical appearance of psoriasis will also have well-demarcated patches and plaques albeit with thicker, silvery scale, frequent nail involvement, and a distribution favoring the scalp, knee, elbow, and intergluteal cleft. Atopic and contact dermatitis morphology can sometimes include well-demarcated lichenified plaques with thin scale. Ashy dermatosis patients will present with well-demarcated macules and patches of varying shape on the face, neck, and trunk, but these will be gray in color. It more frequently affects darker-skinned individuals. Parapsoriasis, characterized by salmon-colored patches with slight scale, is considered by many to be a precursor to MF. These lesions may evolve to become indurated, elevated, and pruritic.1-4
On histopathology, patch stage lesions classically demonstrate epidermotropism of cerebriform lymphocytes and a lymphocytic infiltrate at the edges of the basal layer. Many inflammatory dermatoses share histopathological features with early stage MF including scattered epidermal lymphocytes and papillary dermal fibrosis. This can make early diagnosis difficult. Clonal rearrangements of the T-cell receptor (TCR) gene detected by polymerase chain reaction or Southern blot analysis provide additional support for MF diagnosis.1,3,5,6
The classification and staging of MF as a result of the International Society for Cutaneous Lymphomas/European Organization of Research and Treatment of Cancer discussions is shown in Tables 1 and 2. The case presented is classified as stage IA (T1a N0 M0 B0) based on this system.7
Epidemiology
MF is the most common type of cutaneous T-cell lymphoma and accounts for approximately 54% of cases. In the United States, the incidence is 0.36 cases/100,000 inhabitants and is higher in black population than in the White population. In an National Health Service study of 1500 MF patients from 1990 to 2009, the median age of diagnosis was 54 years with a male to female ratio of 1.6:1. Of the patients, 71% had T1 or T2 stage at diagnosis. Two-thirds (295/443) of T1 stage patients had only T1a disease.3,6
Treatment
Options for treatment of early-stage MF include topical corticosteroids and psoralen–UVA (PUVA) or UVB for more widely distributed disease. In patients with limited patch-stage disease as presented in this case, topical steroids alone can control the eruption. There is a 63% complete response rate using topical steroids in patients with T1 stage disease and a 31% partial response rate. PUVA is similarly effective, with complete and overall response rates reaching 58% to 83% and 95%, respectively. PUVA is well tolerated, but long-term side effects include actinic damage and increased rate of skin malignancies. UVB radiation has a lower response rate than PUVA, but it is more widely available and does not require the use of psoralen.8,9
Topical nitrogen mustard is another option, with response rates comparable to topical steroids and PUVA for T1 stage disease. Patients frequently experience contact dermatitis while being treated with topical nitrogen mustard and, rarely, nonmelanoma skin cancer. Electron beam therapy is also highly effective for early-stage MF, with overall response rates reaching 100% and complete clinical response occurring in 75% of T2 stage disease patients. Most patients receiving electron beam therapy experience radiation-induced nail dystrophy, alopecia, dermatitis, and xerosis.10,11
Our Patient
Two 4 mm punch biopsies were performed from plaques on the patient’s right flank and left thigh. Both specimens showed interface dermatitis, epidermotropism, and a superficial perivascular lymphocytic infiltrate. TCR gene rearrangement test via polymerase chain reaction demonstrated a dominant monoclonal rearrangement from one tissue block. The patient was prescribed topical fluocinonide 0.05% ointment to be used twice daily. Follow-up at 4 months revealed modest improvement in existing lesions and no new lesions.
Conclusion
Early-stage MF can present as patches on the buttocks and thighs as highlighted in this case. The diagnosis and staging of MF can be complex and challenging, but is necessary in order to initiate safe, appropriate, and effective therapy.
Mr. Zubair is a student at Georgetown University School of Medicine in Washington, DC.
Dr. Aziz is staff dermatologist at Washington DC Veterans Affairs Medical Center and assistant professor of dermatology at Howard University in Washington, DC.
Disclosure: Mr. Zubair reports no relevant financial relationships.
Dr. Aziz is employed by Howard University College of Medicine and Washington DC Veterans Affairs Medical Center.
References
1. Knapp CF, Mathew R, Messina JL, Lien MH. CD4/CD8 dual-positive mycosis fungoides: a previously unrecognized variant. Am J Dermatopathol. 2012;34(3):e37-39.
2. Schmidt C. Cutaneous T-cell lymphoma’s confounding nature. J Natl Cancer Inst. 2012;104(11):806-808.
3. Yamashita T, Abbade LP, Marques ME, Marques SA. Mycosis fungoides and Sézary syndrome: clinical, histopathological and immunohistochemical review and update. An Bras Dermatol. 2012;87(6):817-828.
4. Marks JG, Miller JJ. Lookingbill and Marks’ Principles of Dermatology. 5th ed. Philadelphia. PA: Elsevier Saunders; 2013.
5. Dalton SR, Chandler WM, Abuzeid M, et al. Eosinophils in mycosis fungoides: an uncommon finding in the patch and plaque stages. Am J Dermatopathol. 2012;34(6):586-591.
6. Agar NS, Wedgeworth E, Crichton S, et al. Survival outcomes and prognostic factors in mycosis fungoides/Sézary syndrome: validation of the revised International Society for Cutaneous Lymphomas/European Organisation for Research and Treatment of Cancer staging proposal. J Clin Oncol. 2010;28(31):4730-4739.
7. Olsen E, Vonderheid E, Pimpinelli N, et al. Revisions to the staging and classification of mycosis fungoides and Sézary syndrome: a proposal of the International Society for Cutaneous Lymphomas (ISCL) and the cutaneous lymphoma task force of the European Organization of Research and Treatment of Cancer (EORTC). Blood. 2007;110(6):1713-1722.
8. Prince HM, Whittaker S, Hoppe RT. How I treat mycosis fungoides and Sézary syndrome. Blood. 2009;114(20):4337-4353.
9. Zackheim HS, Kashani-Sabet M, Amin S. Topical corticosteroids for mycosis fungoides. Experience in 79 patients. Arch Dermatol. 1998;134(8):949-954.
10. Navi D, Riaz N, Levin YS, Sullivan NC, Kim YH, Hoppe RT. The Stanford University experience with conventional-dose, total skin electron-beam therapy in the treatment of generalized patch or plaque (T2) and tumor (T3) mycosis fungoides. Arch Dermatol. 2011;147(5):561-567.
11. Lindahl LM, Fenger-Gron M, Iversen L. Topical nitrogen mustard therapy in patients with mycosis fungoides or parapsoriasis. J Eur Acad Dermatol Venereol. 2013;27(2):163-168.












