


The emergence of biologic therapies has changed the way dermatologists treat many chronic cutaneous diseases, leading to improved prognosis, control of symptoms and better quality of life for the millions of individuals affected. Over the past decade, biologics have changed the treatment landscape in the management of moderate-to-severe psoriasis and psoriatic arthritis (PsA). Before the frst biologic was FDA approved for psoriasis, treatment options consisted of topical agents, phototherapy and conventional systemic agents.
The purpose of this article is to discuss biologics for the treatment of psoriasis and PsA, the effcacy and safety of these treatments, the importance of clinician and patient education and new drugs in the pipeline.
Biologics For Psoriasis
Psoriasis, a disease of T-cell dysregulation, is a common, chronic, often debilitating infammatory condition that signifcantly impacts a patients health-related quality of life, psychological well-being and physical and social aspects of daily living.1,2 Recently, the pathogenesis of psoriasis has been further elucidated, implicating a more complex immune cascade and identifying new disease modulators as potential therapeutic targets. Elucidation of the immunologic circuits in the pathogenesis of psoriasis has led to the develop- ment of biologicsprotein-based drugs derived from living cells cultured in a laboratory.1,3
Unlike the traditional systemic drugs that affect the entire immune system, biologics are de- signed to target specifc aspects of the immune system. Biologics used to treat psoriatic diseases block T-cell receptors or block proteins in the immune system, such as tumor necrosis factor-alpha (TNF-α) or interleukins 12 and 23.3
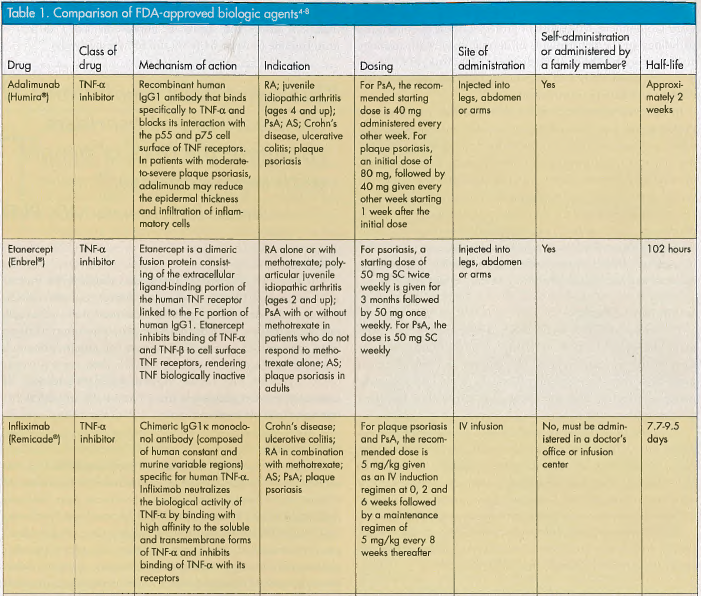
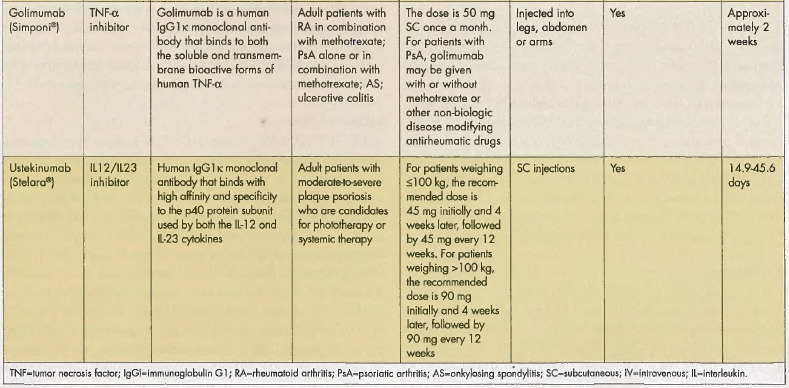
Biologics have revolutionized the treatment of psoriasis, changing the lives of people with severe disease, said Steven R. Feldman, MD, PhD, Center for Dermatology Research and the Departments of Dermatology, Pathology and Public Health Sciences at Wake Forest University School of Medicine in Winston-Salem, NC. Alefacept (Amevive) was the first biologic approved by the FDA in 2003 for the treatment of moderate-to-severe chronic plaque psoriasis. However, in November 2011, Astellas Pharma US, manufacturer of alefacept, announced its decision to cease sales of the drug. There are currently 5 other FDA-approved biologics for psoriasis and PsA: adalimumab (Humira®), etanercept (Enbrel®), golimumab (Simponi®), infiximab (Remicade®) and ustekinumab (Stelara®). Each biologic has a unique mechanism of action, dosing schedule and route of administration (see Table 1).4-8
Psoriasis has become a much easier disease to treat, said Gary Goldenberg, MD, assistant professor of dermatology and pathology in the departments of dermatology and pathology at Mount Sinai School of Medicine in New York, NY. There is a very good chance of improving psoriasis with biologic therapy and having treatment success.
In the past, systemic psoriasis therapies like methotrexate, cyclosporine, acitretin and mycophenolate mofetil were used when psoriasis was too extensive for topical therapy or refractory to topical therapy and phototherapy. However, these medications suppress entire immune function. As a result, clinicians have to do routine laboratory monitoring because of the increased potential for liver and renal toxicity, hematologic conditions (eg, anemia, pancytopenia) and myelosuppression.9,10 Furthermore, systemic therapies are contraindicated in various clinical settings, such as pregnancy and nursing mothers and individuals with liver or kidney disease.9,10


Safety and Effcacy
The advent of biologics has resulted in changes in the treatment and progression of psoriasis.11 Biologics target specifc parts of the immune system. The effcacy and tolerability is more favorable than systemic therapies, providing clinicians with an effective and safe treatment alternative for their patients with psoriasis and PsA.
"The available biologics tend to have greater effcacy and better safety than other systemic medications, perhaps because, in part, they are more targeted to specifc factors," said Dr. Feldman. Another advantage is safety. Biologics are not associated with the renal toxicity, hepatotoxicity and other side effects associated with non-biologic systemic treatments.
The following highlights results from some of the pivotal clinical trials that evaluated the effectiveness and safety of the currently approved biologics for psoriasis and PsA.
Adalimumab
In the Phase III REVEAL (The Randomized Controlled Evaluation of Adalimumab Every Other Week in Moderate to Severe Psoriasis Trial) study, 1,212 patients were randomized to receive adalimumab 40 mg subcutaneously or placebo every other week for 15 weeks. At week 16, 71% of the adalimumab group versus 7% of the placebo group achieved a ≥75% improvement in the Psoriasis Area and Severity Index (PASI) score.1,12 In the recently published open-label extension of the REVEAL trial, patients received adalimumab for 3 years. The patients who initially sustained PASI 75 during REVEAL maintained their improvement after both 100 and 160 weeks of continuous therapy and a PASI 75 was achieved by 83% and 76% of patients, respectively.1,13
Etanercept
The CRYSTEL (Clinical Randomized Year-Long Study Assessing the Safety and Effcacy of Etanercept in Psoriasis) study demonstrated that both continuous and intermittent etanercept treatment regimens improved PASI scores and quality of life. In the 54-week, open-label study of patients with moderate-to-severe plaque psoriasis, the results show both treatment groups had signifcant improvement in PASI scores from baseline to week 54 (68% and 59%, respectively).1,14,15
Infiximab
The Phase III EXPRESS (European Infiximab for Psoriasis [Remicade®] Effcacy and Safety Study) trial assessed the effcacy and safety of continuous treatment with infiximab in patients with moderate-to-severe plaque psoriasis. Patients were randomized to receive infusions of either infiximab 5 mg/kg or placebo at weeks 0, 2 and 6, then every 8weeks
up to week 46. The results showed that 61% and 45% of infiximab-treated patients achieved PASI 75 and PASI 90, respectively, at 50 weeks.
Golimumab
The 24-week effcacy and safety of golimumab in PsA was assessed in the GO-REVEAL (GolimumabA Randomized Evaluation of Safety and Effcacy in Subjects with Psoriatic Arthritis Using a Human Anti-TNF Monoclonal Antibody) trial. In the Phase III, multicenter, randomized, double-blind, placebo-controlled study patients received either placebo, golimumab 50 mg or golimumab 100 mg every 4 weeks through week 20. Among the 74% of patients in whom at least 3% of the body surface area was affected by psoriasis at baseline, the results showed that 40% of those in the golimumab 50 mg group and 58% of those in the golimumab 100 mg group had at least 75% PASI score improvement at week 14 compared with 3% of placebo-treated patients.17
Ustekinumab
The PHOENIX (Phase III, Multicenter, Randomized, Double-blind, Placebo-controlled Trial Evaluating the Effcacy and Safety of CNTO 1275 in the Treatment of Subjects with Moderate to Severe Plaque-type Psoriasis) trials assessed both short- and long-term effcacy and safety in nearly 2,000 patients. In PHOENIX 2, for example, patients were randomly assigned to receive ustekinumab 45 mg or 90 mg at weeks 0 and 4, then every 12 weeks, or placebo. At week 28, partial responders (defned as those achieving a PASI score between 50 and 75) were randomly assigned to continue dosing every 12 weeks or to escalate to dosing every 8 weeks. The results showed that more partial responders at week 28 who received ustekinumab 90 mg every 8 weeks achieved PASI 75 at 1 year than did those who continued to receive the same dose every 12 weeks (68.8% vs 33.3%, respectively).1,18
In terms of safety, biologics have a better safety profle compared with some systemic agents, according to Mark Lebwohl, MD, chairman of the medical board of the National Psoriasis Foundation, New York, NY. The commonly reported adverse events (AEs) with bio- logics were mild and did not result in discontinuation of therapy; these include injection site reactions, respiratory infections and fu-like symptoms. Severe, less common AEs include exacerbation of new-onset congestive heart failure, certain types of cancer, multiple sclerosis, blood disorders, tuberculosis and opportunistic infections.3,9
Because there are AEs associated with biologic therapy, clinicians should prescreen patients before initiation and continue monitoring patients during and after treatments. The FDA and Centers for Disease Control and Prevention, in addition to key consensus statements, have outlined recommendations regarding monitoring.1 The role of biologics in dermatology goes beyond psoriasis and PsA. They have been successfully implemented for off- label use for the treatment of a variety of skin conditions, including auto-immune blistering diseases (eg, pemphigus vulgaris), granulomatous skin diseases (eg, sarcoidosis) and neutrophilic skin diseases (eg, pyoderma gangrenosum).19,20
A potential drawback to biologic therapy is that it has to be given either by injection or intravenous infusion. Infusion can last 2 hours per session (see Table 1). Patients who have not experienced injection therapy tend to prefer a pill, explained Dr. Feldman. In his experience, Dr. Lebwohl said that self-administration of the medication is not a major concern. "Patients are easy to teach," he said
Economic Burden of Biologic Therapy
One disadvantage of biologics is cost to the patient and insurer. Biologic medications tend to be more expensive than topicals or other systemic treatments, said Dr. Feldman. Annual costs of biologics exceed those of other available therapies for psoriasis. The total cost for the frst year of treatment ranged from $23,000 to $33,000. The comparison of annual costs of biologics for psoriasis was $26,862 for etanercept, $23,639 for infiximab, $23,538 for adalimumab and $33,576 for ustekinumab.1,21,22
A study by Bonafede et al analyzed the cost of biologic treatment in patients with rheumatoid arthritis, PsA, psoriasis and ankylosing spondylitis. The researchers used MarketScan Commercial Database to identify patients with ≥1 claim for a biologic between January 1, 2008 and December 31, 2010. The results found that the cost per year for patients with psoriasis ranged from $21,034 for adalimumab to $31,478 for ustekinumab.23
The manufacturers of biologics offer programs to help determine patient eligibility and treatment cost.
Education Is Key
Education is an important component in biologic therapy for both clinicians and patients. Dr. Feldman advises that phy- sicians considering biologic therapy be knowledgeable about all the available options so that you can offer patients all the potential alternatives.
"In my opinion, you have to select the right patient for biologic therapypatients that can beneft from the treatment," added Dr. Goldenberg. "Patients should be educated on how to administer the medication if it is self-administered and the potential side effects." For clinicians, he recommends checking the guidelines for use of biologics in psoriasis. He also encourages physicians who have never prescribed a biologic before to talk with someone who is familiar with prescribing biologics or reach out to a national organization on psoriasis. He said, "They [clinicians] should continue to educate themselves on biologics via medical conferences, lectures or continuing medical education."
Dr. Lebwohl added, "Once you have prescribed biologics for one patient, it is easy."
When deciding on an appropriate biologic therapy, "It is important for physicians to a fnd a biologic they are most comfortable with as a starting point of treatment," said Dr. Goldenberg. Clinicians also need to factor in patient preference and adherence. "It is important that patients are comfortable with the treatment plan. Each patient is different and may have different concerns about a drug. All of these drugs have subtle differences. I think compliance goes way up if they [patients] are part of the decision-making process," added Dr. Goldenberg.

In a study that aimed to better understand the effects of psoriasis treatments on patient satisfaction, patient adherence, healthcare resource utilization and productivity, Raval et al found overall that satisfaction and adherence to biologic therapies appears to be greater compared with traditional therapies.24
An observational study of 2,151 patients with plaque psoriasis demonstrated clinical improvement and treatment satisfaction with biologics compared with other therapies. The results found that more patients receiving biologic therapies improved from severe to moderate or mild psoriasis versus other treatments, as disease severity declined from 70% to 15%.
Biologics in the Pipeline
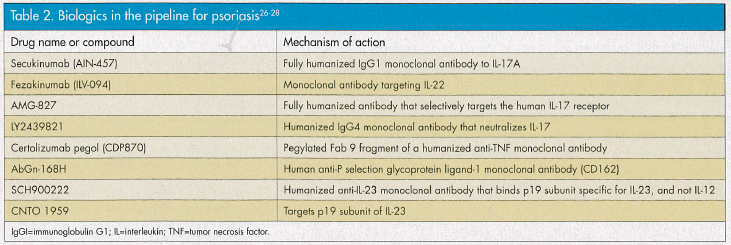
There are still more advances to be made in this feld. Clinical trials are underway evaluating the safety and effcacy of new biologic therapies for the treatment of moderate-to-severe psoriasis and PsA (see Table 2).1,26-28
Conclusion
The development of biologics has changed the landscape of treatment options for patients living with psoriasis and PsA. The proven effcacy and safety of these therapies have added to the arsenal of medications available to help clinicians better treat their patients. As more biologic therapies enter the marketplace, the opportunity for improved prognosis and symptom control will beneft patients and enhance their health-related quality of life.
References
1. Levy LL, Solomon SM, Emer JJ. Biologics in the treatment of psoriasis and emerging new therapies in the pipeline. Psoriasis: Targets and Therapy. 2012;2:29-43.
2. Bhosle MJ, Kulkarni A, Feldman SR, Balkrishnan R. Quality of life in patients with psoriasis. Health Qual Life Outcomes. 2006;4:35.
3. National Psoriasis Foundation. Moderate to Severe Psoriasis: Biologic Drugs. https://www.psoriasis.org/about-psoriasis/treatments/biologics. Accessed July1, 2013.
4. Humira [prescribing information]. North Chicago, IL: AbbVie Inc; 2013.
5. Enbrel [prescribing information]. Thousand Oaks, CA: Amgen Inc; 2012.
6. Remicade [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
7. Simponi [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
8. Stelara [prescribing information]. Horsham, PA: Janssen Biotech Inc; 2013.
9. Menter A, Gottlieb A, Feldman SR, et al. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 1. Overview of psoriasis and guidelines of care for the treatment of psoriasis with biologics. 2008;58(5):826-850.
10. Menter A, Korman NJ, Elmets CA. Guidelines of care for the management of psoriasis and psoriatic arthritis: Section 4. Guidelines of care for the management and treatment of psoriasis with traditional systemic agents. J Am Acad Dermatol. 2009;61(3):451-485.
11. Sánchez-Carazo JL. Present and future biologic therapy in dermatology. Actas Dermostiflogr. 2008;99(2):89-90.
12. Menter A, Tyring SK, Gordon K, et al. Adalimumab therapy for moderate to severe psoriasis: A randomized, controlled phase III trial. J Am Acad Dermatol. 2008;58(1):106-115.
13. Gordon K, Papp K, Poulin Y, et al. Long-term effcacy and safety of adalimumab in patients with moderate to severe psoriasis treated continuously over 3 years: Results from an open-label extension study for patients from REVEAL. J Am Acad Dermatol. 2012;66(2):241-251.
14. Ortonne JP, Griffths C, Daudén E, et al. Effcacy and safety of continuous versus paused etanercept treatment in patients with moderate-to-severe psoriasis over 54 weeks: The CRYSTEL study. Exp Rev Dermatol. 2008;3(6):657-665.
15. Daudén E, Griffths CE, Ortonne JP, et al. Improvements in patient-reported outcomes in moderate-to-severe psoriasis patients receiving continuous or paused etanercept treatment over 54 weeks: The CRYSTEL study. J Eur Acad Dermatol Venereol. 2009;23(12):1374-1382.
16. Reich K, Nestle FO, Papp K, et al. Infiximab induction and maintenance therapy for moderate-to-severe psoriasis: A Phase III, multicentre, double- blind trial. Lancet. 2005;366(9494):1367-1374.
17. Kavanaugh A, McInnes I, Mease P, et al. Golimumab, a new human tumor necrosis factor alpha antibody, administered every four weeks as a subcutaneous injection in psoriatic arthritis: Twenty-four-week effcacy and safety results of a randomized, placebo-controlled study. Arthritis Rheum. 2009;60(4):976-986.
18. Papp KA, Langley RG, Lebwohl M, et al. Effcacy and safety of ustekinumab, a human interleukin-12/23 monoclonal antibody, in patients with psoriasis: 52-week results from a randomised, double-blind, placebo- controlled trial (PHOENIX 2). Lancet. 2008;371(9625):1675-1684.
19. Guhl G, Díaz-Ley B, Fernández-Herrera J. Off-label use of biologic agents in the treatment of dermatosis, part 2: Etanercept, efalizumab, alefacept, rituximab, daclizumab, basiliximab, omalizumab and cetuximab. Actas Dermosifliogr .2008;99(1):5-33.
20. Díaz-Ley B, Guhl G, Fernández-Herrera. Off-label use of biologic agents in the treatment of dermatosis, part 1: Infiximab and adalimumab. Actas Dermosifliogr. 2007;98(10):657-678.
21. Beyer V, Wolverton SE. Recent trends in systemic psoriasis treatment costs. Arch Dermatol. 2010;146(1):46-54.
22. Schafer JA, Kjesbo NK, Gleason PP. Formulary review of 2 new biologic agents: Tocilizumab for rheumatoid arthritis and ustekinumab for plaque psoriasis. J Manag Care Pharm. 2010;16(6):402-416.
23. Bonafede MM, Joseph G, Princic N, Harrison DJ. Cost per treated patient for biologics in rheumatology arthritis, psoriasis and ankylosing spondylitis using claims data. Value in Health. 2013;16(3):A220.
24. Raval K, Lofand JH, Waters H, Piech CT. Disease and treatment burden of psoriasis: Examining the impact of biologics. J Drugs Dermatol. 2011;10(2):189-196.
25. Christophers E, Segaert S, Milligan G, Molta CT, Boggs R. Clinical improvement and satisfaction with biologic therapy in patients with severe plaque psoriasis: Results of a European cross-sectional observational study. J Dermatolog Treat. 2013;24(3):193-198.
26. Clinicaltrials.gov. www.clinicaltrials.gov. Accessed July 1, 2013.
27. Weger W. Current status and new developments in the treatment of psoriasis and psoriatic arthritis with biological agents. Br J Pharmacol. 2010;160(4):810-820.
28. Johnson-Huang LM, Lowes MA, Krueger JG. Putting together the psoriasis puzzle: An update on developing targeted therapies. Dis Model Mech. 2012;5(4):423-433.








