This case study presents an unusual case of a low-grade eccrine carcinoma showing squamous differentiation.
A 75-year-old woman presented with a lesion on the left wrist.
Microscopic Description
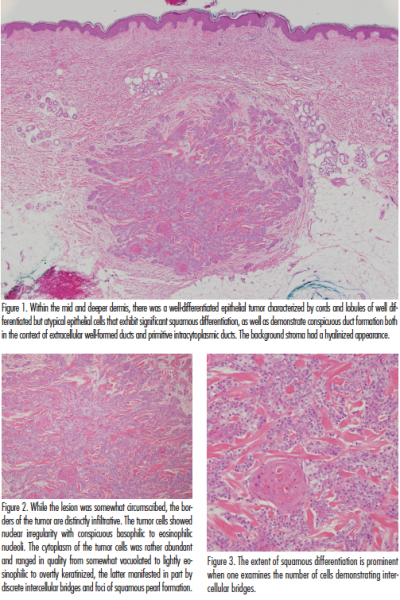
Within the mid and deeper dermis, there was a well-differentiated epithelial tumor characterized by cords and lobules of well differentiated but atypical epithelial cells that show both ductal and squamous differentiation (Figure 1).
The background stroma had a hyalinized appearance. While the lesion was somewhat circumscribed, the borders of the tumor were infiltrative. The tumor cells showed nuclear irregularity with conspicuous basophilic to eosinophilic nucleoli. The cytoplasm of the tumor cells was rather abundant and ranged in quality from somewhat vacuolated to lightly eosinophilic to overtly keratinized, the latter manifested in part by discrete intercellular bridges and foci of squamous pearl formation (Figure 2). In the squamatized areas, the cells exhibited primitive intracytoplasmic ducts lined by distinct cuticles (Figure 3). The less keratinized areas demonstrated well-formed ducts lined by ductal epithelium. There were occasional mitotic figures. There was neither vascular nor perineural infiltration. A broad grenz zone of superficial dermis separated the tumor from the epidermis. There were no areas of continuity of the neoplasm to the epidermis or follicle.
Immunohistochemical Profile
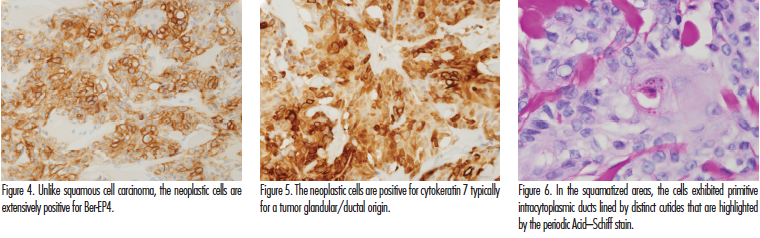
The tumor cells demonstrated striking positivity for cytokeratin 7, Ber-EP4, and P63 (Figures 4 and 5). Focal staining was observed for mammoglobin while the cytokeratin 15 stain was negative. There was periodic Acid–Schiff stain positive diastase resistant mucin found within the neoplastic cells (Figure 6).
The combined light microscopic and phenotypic profile led to a diagnosis of a squamoid eccrine ductal carcinoma (SEDC).
Discussion
This case study presents an unusual case of what we believe is a low-grade eccrine carcinoma showing squamous differentiation. The basis for designating the tumor as malignant is largely due to the deep-seated nature of the tumor exhibiting infiltrative borders along with cytologic atypia. The latter defines a subjective morphologic parameter but the nuclear quality and nuclear heterogeneity suggests a malignant categorization over a benign tumor. The question arises regarding classification. Given its well differentiated but atypical appearance and hybrid squamous and eccrine ductal differentiation, we have elected to designate the case as a SEDC. The purpose of recognizing this entity is to avoid miscategorization as a squamous cell carcinoma (SCC). Furthermore, the distinctive histology confers a more indolent clinical course as seen in our case.
Originally described in 1997, SEDC characterizes eccrine ductal carcinoma that contains squamoid differentiation resembling invasive SCC.1 These tumors usually present in older individuals and are predominantly found on sun-damaged skin, with the face being the most frequently affected site.2 Patients usually present with a nodule or plaque with possible ulceration and necrosis.3 Although SEDC is a rare and poorly documented tumor, a biphasic growth pattern is observed in many cases. The tumor oftentimes and characteristically involves the more superficial aspect of the dermis and is frequently contiguous with the epidermis. It is this superficial aspect of the neoplasm that demonstrates significant and at times exclusive squamous differentiation, while the deeper-seated aspect of the neoplasm shows an infiltrative lesser keratinized morphology and would be more in keeping with a conventional eccrine carcinoma. That being said, there are zones where both the squamoid and eccrine ductal aspects of the neoplasm merge imperceptibly.
Our case is unique because of morphologic features that could be construed as divergent from other reported cases given the lack of epidermal continuity and the absence of a more superficial dermal involvement. The 2 components were also intimately admixed as opposed to being morphologically distinct. Additionally, our case was very well differentiated without overt pleomorphic cytologic features that can occur in these neoplasms.2 Perineural and lymphovascular invasion can also be seen, although it was not seen in this case.4 Despite the aforesaid, the designation of SEDC is a term that would appear to be apropos for the morphology depicted. SEDC is generally considered to be a low-grade malignancy but does have the tendency for local recurrences. SEDC has been described in organ transplant patients.3
The differential diagnosis encompasses a microcystic adnexal carcinoma, which is now categorized as a carcinoma of the folliculosebaceous apocrine unit. Squamous differentiation can occur in the microcystic adnexal carcinoma and indeed one might view cases of the SEDC as a more florid expression of the pattern of squamous differentiation potentially encountered in microcystic adnexal carcinoma. The distinction of SEDC from a porocarcinoma with squamous differentiation or eccrine ductal carcinoma with squamous differentiation can be very difficult. At least with the designation of eccrine ductal carcinoma with squamous differentiation, we would suggest that the 2 terms likely refer to a similar spectrum of carcinomas with a common histogenesis. Eccrine porocarcinoma is sufficiently distinctive in terms of a precursor lesion of poroma and its predilection for distal extremities makes its separation from SEDC reasonable.
The designation of SEDC should likely encompass both the divergent biphasic neoplasms that have been previously reported in the literature, but also include a well differentiation eccrine carcinoma in which there is an intrinsic squamous component within a tumor exhibiting classic features of eccrine ductal carcinoma. Indeed, there are areas captured in images reported on this rare tumor that show infiltrative lobules of an epithelial neoplasm demonstrating both squamous and eccrine differentiation almost reminiscent of a mucoepidermoid carcinoma.
From an ontogeny perspective, the ability of an eccrine carcinoma to exhibit squamous differentiation likely reflects its origin in the keratinizing portion of the acrosyringium.
Dr Magro is the director of dermatopathology at Weill Cornell Medicine in New York, NY.
Disclosure: The author reports no relevant financial relationships.
References
1. Wong TY, Suster S, Mihm MC. Squamoid eccrine ductal carcinoma. Histopathology 197;30(3):288-293.
2. van der Horst MP, Garcia-Herrera A, Markiewicz D, Martin B, Calonje E, Brenn T. Squamoid eccrine ductal carcinoma: A clinicopathologic study of 30 cases [published online January 19, 2016]. Am J Surg Path. doi:10.1097/PAS.0000000000000599.
3. Frouin E, Vignon-Pennamen MD, Balme B, et al. Anatomoclinical study of 30 cases of sclerosing sweat duct carcinomas (microcystic adnexal carcinoma, syringomatous carcinoma and squamoid eccrine ductal carcinoma). J Eur Acad Dermatol Venereol. 2015;29(10):1978-1994.
4. Cardoso JC, Calonje E. Malignant sweat gland tumours: an update. Histopathology. 2015;67(5): 589-606.
This case study presents an unusual case of a low-grade eccrine carcinoma showing squamous differentiation.
A 75-year-old woman presented with a lesion on the left wrist.
Microscopic Description
Within the mid and deeper dermis, there was a well-differentiated epithelial tumor characterized by cords and lobules of well differentiated but atypical epithelial cells that show both ductal and squamous differentiation (Figure 1).
The background stroma had a hyalinized appearance. While the lesion was somewhat circumscribed, the borders of the tumor were infiltrative. The tumor cells showed nuclear irregularity with conspicuous basophilic to eosinophilic nucleoli. The cytoplasm of the tumor cells was rather abundant and ranged in quality from somewhat vacuolated to lightly eosinophilic to overtly keratinized, the latter manifested in part by discrete intercellular bridges and foci of squamous pearl formation (Figure 2). In the squamatized areas, the cells exhibited primitive intracytoplasmic ducts lined by distinct cuticles (Figure 3). The less keratinized areas demonstrated well-formed ducts lined by ductal epithelium. There were occasional mitotic figures. There was neither vascular nor perineural infiltration. A broad grenz zone of superficial dermis separated the tumor from the epidermis. There were no areas of continuity of the neoplasm to the epidermis or follicle.

Immunohistochemical Profile
The tumor cells demonstrated striking positivity for cytokeratin 7, Ber-EP4, and P63 (Figures 4 and 5). Focal staining was observed for mammoglobin while the cytokeratin 15 stain was negative. There was periodic Acid–Schiff stain positive diastase resistant mucin found within the neoplastic cells (Figure 6).
The combined light microscopic and phenotypic profile led to a diagnosis of a squamoid eccrine ductal carcinoma (SEDC).
Discussion
This case study presents an unusual case of what we believe is a low-grade eccrine carcinoma showing squamous differentiation. The basis for designating the tumor as malignant is largely due to the deep-seated nature of the tumor exhibiting infiltrative borders along with cytologic atypia. The latter defines a subjective morphologic parameter but the nuclear quality and nuclear heterogeneity suggests a malignant categorization over a benign tumor. The question arises regarding classification. Given its well differentiated but atypical appearance and hybrid squamous and eccrine ductal differentiation, we have elected to designate the case as a SEDC. The purpose of recognizing this entity is to avoid miscategorization as a squamous cell carcinoma (SCC). Furthermore, the distinctive histology confers a more indolent clinical course as seen in our case.
Originally described in 1997, SEDC characterizes eccrine ductal carcinoma that contains squamoid differentiation resembling invasive SCC.1 These tumors usually present in older individuals and are predominantly found on sun-damaged skin, with the face being the most frequently affected site.2 Patients usually present with a nodule or plaque with possible ulceration and necrosis.3 Although SEDC is a rare and poorly documented tumor, a biphasic growth pattern is observed in many cases. The tumor oftentimes and characteristically involves the more superficial aspect of the dermis and is frequently contiguous with the epidermis. It is this superficial aspect of the neoplasm that demonstrates significant and at times exclusive squamous differentiation, while the deeper-seated aspect of the neoplasm shows an infiltrative lesser keratinized morphology and would be more in keeping with a conventional eccrine carcinoma. That being said, there are zones where both the squamoid and eccrine ductal aspects of the neoplasm merge imperceptibly.
Our case is unique because of morphologic features that could be construed as divergent from other reported cases given the lack of epidermal continuity and the absence of a more superficial dermal involvement. The 2 components were also intimately admixed as opposed to being morphologically distinct. Additionally, our case was very well differentiated without overt pleomorphic cytologic features that can occur in these neoplasms.2 Perineural and lymphovascular invasion can also be seen, although it was not seen in this case.4 Despite the aforesaid, the designation of SEDC is a term that would appear to be apropos for the morphology depicted. SEDC is generally considered to be a low-grade malignancy but does have the tendency for local recurrences. SEDC has been described in organ transplant patients.3

The differential diagnosis encompasses a microcystic adnexal carcinoma, which is now categorized as a carcinoma of the folliculosebaceous apocrine unit. Squamous differentiation can occur in the microcystic adnexal carcinoma and indeed one might view cases of the SEDC as a more florid expression of the pattern of squamous differentiation potentially encountered in microcystic adnexal carcinoma. The distinction of SEDC from a porocarcinoma with squamous differentiation or eccrine ductal carcinoma with squamous differentiation can be very difficult. At least with the designation of eccrine ductal carcinoma with squamous differentiation, we would suggest that the 2 terms likely refer to a similar spectrum of carcinomas with a common histogenesis. Eccrine porocarcinoma is sufficiently distinctive in terms of a precursor lesion of poroma and its predilection for distal extremities makes its separation from SEDC reasonable.
The designation of SEDC should likely encompass both the divergent biphasic neoplasms that have been previously reported in the literature, but also include a well differentiation eccrine carcinoma in which there is an intrinsic squamous component within a tumor exhibiting classic features of eccrine ductal carcinoma. Indeed, there are areas captured in images reported on this rare tumor that show infiltrative lobules of an epithelial neoplasm demonstrating both squamous and eccrine differentiation almost reminiscent of a mucoepidermoid carcinoma.
From an ontogeny perspective, the ability of an eccrine carcinoma to exhibit squamous differentiation likely reflects its origin in the keratinizing portion of the acrosyringium.
Dr Magro is the director of dermatopathology at Weill Cornell Medicine in New York, NY.
Disclosure: The author reports no relevant financial relationships.
References
1. Wong TY, Suster S, Mihm MC. Squamoid eccrine ductal carcinoma. Histopathology 197;30(3):288-293.
2. van der Horst MP, Garcia-Herrera A, Markiewicz D, Martin B, Calonje E, Brenn T. Squamoid eccrine ductal carcinoma: A clinicopathologic study of 30 cases [published online January 19, 2016]. Am J Surg Path. doi:10.1097/PAS.0000000000000599.
3. Frouin E, Vignon-Pennamen MD, Balme B, et al. Anatomoclinical study of 30 cases of sclerosing sweat duct carcinomas (microcystic adnexal carcinoma, syringomatous carcinoma and squamoid eccrine ductal carcinoma). J Eur Acad Dermatol Venereol. 2015;29(10):1978-1994.
4. Cardoso JC, Calonje E. Malignant sweat gland tumours: an update. Histopathology. 2015;67(5): 589-606.
This case study presents an unusual case of a low-grade eccrine carcinoma showing squamous differentiation.
A 75-year-old woman presented with a lesion on the left wrist.
Microscopic Description
Within the mid and deeper dermis, there was a well-differentiated epithelial tumor characterized by cords and lobules of well differentiated but atypical epithelial cells that show both ductal and squamous differentiation (Figure 1).
The background stroma had a hyalinized appearance. While the lesion was somewhat circumscribed, the borders of the tumor were infiltrative. The tumor cells showed nuclear irregularity with conspicuous basophilic to eosinophilic nucleoli. The cytoplasm of the tumor cells was rather abundant and ranged in quality from somewhat vacuolated to lightly eosinophilic to overtly keratinized, the latter manifested in part by discrete intercellular bridges and foci of squamous pearl formation (Figure 2). In the squamatized areas, the cells exhibited primitive intracytoplasmic ducts lined by distinct cuticles (Figure 3). The less keratinized areas demonstrated well-formed ducts lined by ductal epithelium. There were occasional mitotic figures. There was neither vascular nor perineural infiltration. A broad grenz zone of superficial dermis separated the tumor from the epidermis. There were no areas of continuity of the neoplasm to the epidermis or follicle.
Immunohistochemical Profile
The tumor cells demonstrated striking positivity for cytokeratin 7, Ber-EP4, and P63 (Figures 4 and 5). Focal staining was observed for mammoglobin while the cytokeratin 15 stain was negative. There was periodic Acid–Schiff stain positive diastase resistant mucin found within the neoplastic cells (Figure 6).
The combined light microscopic and phenotypic profile led to a diagnosis of a squamoid eccrine ductal carcinoma (SEDC).
Discussion
This case study presents an unusual case of what we believe is a low-grade eccrine carcinoma showing squamous differentiation. The basis for designating the tumor as malignant is largely due to the deep-seated nature of the tumor exhibiting infiltrative borders along with cytologic atypia. The latter defines a subjective morphologic parameter but the nuclear quality and nuclear heterogeneity suggests a malignant categorization over a benign tumor. The question arises regarding classification. Given its well differentiated but atypical appearance and hybrid squamous and eccrine ductal differentiation, we have elected to designate the case as a SEDC. The purpose of recognizing this entity is to avoid miscategorization as a squamous cell carcinoma (SCC). Furthermore, the distinctive histology confers a more indolent clinical course as seen in our case.
Originally described in 1997, SEDC characterizes eccrine ductal carcinoma that contains squamoid differentiation resembling invasive SCC.1 These tumors usually present in older individuals and are predominantly found on sun-damaged skin, with the face being the most frequently affected site.2 Patients usually present with a nodule or plaque with possible ulceration and necrosis.3 Although SEDC is a rare and poorly documented tumor, a biphasic growth pattern is observed in many cases. The tumor oftentimes and characteristically involves the more superficial aspect of the dermis and is frequently contiguous with the epidermis. It is this superficial aspect of the neoplasm that demonstrates significant and at times exclusive squamous differentiation, while the deeper-seated aspect of the neoplasm shows an infiltrative lesser keratinized morphology and would be more in keeping with a conventional eccrine carcinoma. That being said, there are zones where both the squamoid and eccrine ductal aspects of the neoplasm merge imperceptibly.
Our case is unique because of morphologic features that could be construed as divergent from other reported cases given the lack of epidermal continuity and the absence of a more superficial dermal involvement. The 2 components were also intimately admixed as opposed to being morphologically distinct. Additionally, our case was very well differentiated without overt pleomorphic cytologic features that can occur in these neoplasms.2 Perineural and lymphovascular invasion can also be seen, although it was not seen in this case.4 Despite the aforesaid, the designation of SEDC is a term that would appear to be apropos for the morphology depicted. SEDC is generally considered to be a low-grade malignancy but does have the tendency for local recurrences. SEDC has been described in organ transplant patients.3
The differential diagnosis encompasses a microcystic adnexal carcinoma, which is now categorized as a carcinoma of the folliculosebaceous apocrine unit. Squamous differentiation can occur in the microcystic adnexal carcinoma and indeed one might view cases of the SEDC as a more florid expression of the pattern of squamous differentiation potentially encountered in microcystic adnexal carcinoma. The distinction of SEDC from a porocarcinoma with squamous differentiation or eccrine ductal carcinoma with squamous differentiation can be very difficult. At least with the designation of eccrine ductal carcinoma with squamous differentiation, we would suggest that the 2 terms likely refer to a similar spectrum of carcinomas with a common histogenesis. Eccrine porocarcinoma is sufficiently distinctive in terms of a precursor lesion of poroma and its predilection for distal extremities makes its separation from SEDC reasonable.
The designation of SEDC should likely encompass both the divergent biphasic neoplasms that have been previously reported in the literature, but also include a well differentiation eccrine carcinoma in which there is an intrinsic squamous component within a tumor exhibiting classic features of eccrine ductal carcinoma. Indeed, there are areas captured in images reported on this rare tumor that show infiltrative lobules of an epithelial neoplasm demonstrating both squamous and eccrine differentiation almost reminiscent of a mucoepidermoid carcinoma.
From an ontogeny perspective, the ability of an eccrine carcinoma to exhibit squamous differentiation likely reflects its origin in the keratinizing portion of the acrosyringium.
Dr Magro is the director of dermatopathology at Weill Cornell Medicine in New York, NY.
Disclosure: The author reports no relevant financial relationships.
References
1. Wong TY, Suster S, Mihm MC. Squamoid eccrine ductal carcinoma. Histopathology 197;30(3):288-293.
2. van der Horst MP, Garcia-Herrera A, Markiewicz D, Martin B, Calonje E, Brenn T. Squamoid eccrine ductal carcinoma: A clinicopathologic study of 30 cases [published online January 19, 2016]. Am J Surg Path. doi:10.1097/PAS.0000000000000599.
3. Frouin E, Vignon-Pennamen MD, Balme B, et al. Anatomoclinical study of 30 cases of sclerosing sweat duct carcinomas (microcystic adnexal carcinoma, syringomatous carcinoma and squamoid eccrine ductal carcinoma). J Eur Acad Dermatol Venereol. 2015;29(10):1978-1994.
4. Cardoso JC, Calonje E. Malignant sweat gland tumours: an update. Histopathology. 2015;67(5): 589-606.











