PATIENT PRESENTATION
A 5-year-old boy was brought to the dermatologist’s office by his mother for evaluation of a rash on his hands. He complained of mild discomfort and a burning sensation on the palms. On examination, multiple vesicles with surrounding erythema were noted to predominantly affect the palms in a symmetrical distribution. He presented with odynophagia and 2 erosions on the buccal mucosa.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Hand, Foot and Mouth Disease
Hand, foot and mouth disease (HFMD) is a common enteroviral illness of childhood characterized by fever and classic cutaneous findings, which include a papulovesicular eruption on the palms and soles as well as an erosive stomatitis. Children under the age of 10 are usually affected, although HFMD has also been described in immunocompetent adolescents and adults.1 Males and females are equally affected, and incidence is greatest during the summer and autumn months.2 The virus is transmitted by respiratory and oral-fecal routes through contact with respiratory secretions, vesicular fluid, saliva and feces.
Coxsackievirus A16 is the most common cause of HFMD in the United States, but other non-polio enteroviruses, including coxsackieviruses A5-7, A9, A10, B11, B3, B5, echovirus 4 and enterovirus 71, have been implicated.2,3 Notably, enterovirus 71(EV71) infection is linked to large epidemics of the disease in Asian-Pacific countries and is associated with neurologic and systemic complications that can prove fatal.4-7 The prevalence of EV71 infection in this region has greatly increased since 1997, with large outbreaks reported in Japan, Malaysia, Singapore, South Korea, China and Australia. Although outbreaks of EV71-related HFMD have been noted in the aforementioned countries, no large-scale epidemics have been reported in the United States. Coxsackie A16 infection was largely thought to be free of these neurologic complications, but a recent study disputes that claim.8 It is difficult to assess the epidemiological details of HFMD in the United States, as countries have different reporting and surveillance practices. HFMD is not a notifiable disease in the United States and, therefore, the actual number of HFMD cases in the country is unknown.
Clinical Presentation
Clinically, hand, foot and mouth disease is characterized by a vesicular eruption on the palms and soles and an erosive stomatitis. A prodromal illness of fever, malaise and myalgias precedes the mucocutaneous findings by 1-4 days. Erythematous macules and papules evolve into 3-mm to 7-mm, grey to white, oval to football shaped vesicles with an erythematous halo on the palms and soles. Less commonly, the dorsal hands and feet are involved. A vesicular or morbilliform eruption may be present on the buttocks, genitalia, extremities and perianally. Enanthem, or mucosal eruption, is characterized by vesicles and erosions with surrounding erythema on the buccal mucosa, gingiva, tonsilar pillars, palate and uvula. The mucosal lesions usually precede the hand and foot findings but may be absent in some individuals.1 Lesions can be asymptomatic or associated with pain from touch or pressure. The illness is usually mild with resolution of symptoms within 7-14 days. Onychomadesis may result 1-2 months after resolution of the exanthem.
During outbreaks of the EV71 virus in Asian-Pacific countries, thousands of children developed mild, self-limited HFMD. However, a small proportion of cases rapidly become associated with neurological and systemic complications that can be fatal. Infection with EV71 has been linked with severe symptoms including aseptic meningitis, flaccid paralysis, pulmonary edema, brainstem encephalitis and cardiopulmonary collapse.4-7,9 A large, prospective, study of several epidemics that occurred over 7 years in Malaysia showed 10%–30% of children hospitalized with EV71-related HFMD developed CNS complications.10 Brainstem encephalitis was the most frequent presentation, accounting for 58% of neurological manifestations, followed by aseptic meningitis (36%) and brainstem encephalitis with cardiorespiratory dysfunction (4%).9 Most children with CNS involvement had concurrent clinical features of HFMD, but a small proportion presented only with neurological features. Myoclonic jerks are seen more often in EV71 infection compared to other enteroviruses and could be an early indicator of neurological involvement.10
Brainstem encephalitis associated with cardiopulmonary dysfunction has become a notable feature in EV71 epidemics in Asia and is the primary cause of death. Exact statistics of this entity are difficult to assess based on the current literature. A Malaysian study found 4% of children with neurologic manifestations developed brainstem encephalitis and cardiorespiratory dysfunction.9 A Tawainese study found 10 out of 97 patients developed the entity.11 Children typically present with a brief febrile illness, clinical features of HFMD and mild neurological symptoms. A sudden deterioration is noted after 3-5 days; without swift intervention in the ICU, this manifestation can result in death.
 Differential Diagnoses
Differential Diagnoses
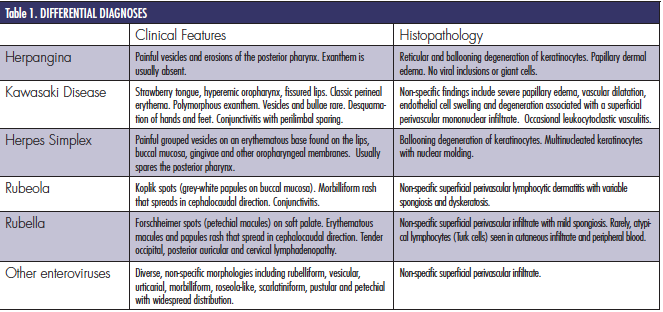
Overlapping clinical features may be seen in herpangina, herpes simplex virus, Kawasaki disease, alternative enteroviral infections and other viral exanthems, including measles and rubella (Table 1).
Histopathology
Histopathologic findings are not diagnostic for HFMD. Biopsy reveals an intra-epidermal vesicle, ballooning degeneration of keratinocytes, epidermal necrosis and marked papillary edema. A non-specific dermal inflammatory infiltrate is present. Viral inclusion bodies and giant cells are not appreciated.
Diagnosis and Management
Hand, foot and mouth disease is primarily a clinical diagnosis. When necessary, the virus can be isolated through culture or polymerase chain reaction of oropharyngeal secretions, vesicular fluid or feces. The disease usually has a benign, self-limited clinical course. Supportive measures and symptomatic management will normally suffice. However, in cases of enterovirus 71 infection complicated by severe neurologic and systemic sequelae, hospitalization and possible mechanical ventilation may be required.
No established antiviral treatment exists for EV71 infection, although several treatments have been tried. Pleconaril is an antiviral medication that inhibits the entry of several enteroviruses into cells by blocking viral attachment and uncoating. It has been used in clinical trials for aseptic meningitis and was once thought to be a promising treatment for EV71 infection. However, a recent study revealed pleconaril does not appear to be active against the EV71 strain.12
Intravenous immunoglobulin has been shown to be of benefit when given early in the disease course13,14 and is used on the presumptive basis that it neutralizes EV71 and has non-specific anti-inflammatory properties. One retrospective comparison in Malaysia showed 204 (95%) of 215 survivors who had severe CNS complications had received intravenous immunoglobulin treatment in comparison to only one (11%) of 9 fatal cases.14 No randomized trials have been undertaken, but intravenous immunoglobulin is being more routinely used. Other treatments being explored include ribavirin, interferons and RNA interference.15-18
Proper hygiene helps to prevent transmission. HFMD is most contagious during the presence of cutaneous symptoms, but the virus can be shed for weeks after vesicular resolution. As a result, it is ineffective to keep children sequestered from school after the initial cutaneous findings have resolved.
In our patient, the clinical symptoms resolved within 2 weeks without sequelae.
Conclusion
HFMD is a common pediatric enteroviral illness that usually follows a benign, self-limited course. However, clinicians should be aware of other enteroviral strains with neurologic and systemic sequelae, namely EV71, that have resulted in epidemics in Asian-Pacific countries.
Dr. Wright is a second-year dermatology resident at the State University of New York Downstate in Brooklyn, NY.
Dr. Ehrsam is a dermatologist in Lille, France.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Shin JU, Oh SH, Lee JH. A case of hand-foot-mouth disease in an immunocompetent adult. Ann Dermatol. 2010;22(2):216-218. doi: 10.5021/ad.2010.22.2.216. Epub 2010 May 18.
2. Centers of Disease Control and Prevention. Hand, foot and mouth disease. Available at: https://www.cdc.gov/hand-foot-mouth/index.html. Accessibility verified March 21, 2013.
3. Wu Y, Yeo A, Phoon MC, et al. The largest outbreak of hand; foot and mouth disease in Singapore in 2008: The role of enterovirus 71 and coxsackievirus A strains. Int J Infect Dis. 2010;14(12):e1076-e1081. doi: 10.1016/j.ijid.2010.07.006. Epub 2010 Oct 16.
4. Chan KP, Goh KT, Chong CY, Teo ES, Lau G, Ling AE. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infect Dis. 2003;9(1):78–85.
5. Lin TY, Twu SJ, Ho MS, Chang LY, Lee CY. Enterovirus 71 outbreaks, Taiwan: Occurrence and recognition. Emerg Infect Dis. 2003;9(3):291–293.
6. Ho M. Enterovirus 71: The virus, its infections and outbreaks. J Microbiol Immunol Infect. 2000;33(4):205–216.
7. Chan LG, Parashar UD, Lye MS, et al. Deaths of children during an outbreak of hand, foot, and mouth disease in Sarawak, Malaysia: Clinical and pathological characteristics of the disease. For the Outbreak Study Group. Clin Infect Dis. 2000;31(3):678–683.
8. Xu W, Liu CF, Yan L, et al. Distribution of enteroviruses in hospitalized children with hand, foot and mouth disease and relationship between pathogens and nervous system complications. Virol J. 2012;9;9(1):8. doi: 10.1186/1743-422X-9-8.
9. Ooi MH, Wong SC, Lewthwaite P, Cardosa MJ, Solomon T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010;9(11):1097–1105. doi: 10.1016/S1474-4422(10)70209-X.
10. Ooi MH, Wong SC, Podin Y, et al. Human enterovirus 71 disease in Sarawak, Malaysia: A prospective clinical, virulogical and molecular epidemiological study. Clin Infect Dis. 2007;44(5):646-656.
11. Wang SM, Liu CC, Tseng HW, et al. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurologic complications. Clin Infect Dis. 1999; 29(1):184-90.
12. Chen TC, Weng KF, Chang SC, Lin JY, Huang PN, Shih SR. Development of antiviral agents for enteroviruses. J Antimicrob Chemother. 2008 Dec;62(6):1169–1173. doi: 10.1093/jac/dkn424. Epub 2008 Oct 18.
13. Chang LY, Hsia SH, Wu CT, et al. Outcome of enterovirus 71 infections with or without stage-based management: 1998 to 2002. Pediatr Infect Dis J. 2004;23(4):327–332.
14. Ooi MH, Wong SC, Mohan A, et al. Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot, and mouth disease in Sarawak. BMC Infect Dis. 2009 Jan 19;9:3. doi: 10.1186/1471-2334-9-3.
15. Li ZH, Li CM, Ling P, et al. Ribavirin reduces mortality in enterovirus 71-infected mice by decreasing viral replication. J Infect Dis. 2008;197(6):854–857. doi: 10.1086/527326.
16. Liu ML, Lee YP, Wang YF, et al. Type I interferons protect mice against enterovirus 71 infection. J Gen Virol. 2005;86(Pt 12):3263–3269.
17. Sim AC, Luhur A, Tan TM, Chow VT, Poh CL. RNA interference against enterovirus 71 infection. Virology. 2005;341(1):72–79.
18. Wu Z, Yang F, Zhao R, Zhao L, Guo D, Jin Q. Identification of small interfering RNAs which inhibit the replication of several Enterovirus 71 strains in China. J Virol Methods. 2009;159(2):233–238. doi: 10.1016/j.jviromet.2009.04.002. Epub 2009 Apr 10.
PATIENT PRESENTATION
A 5-year-old boy was brought to the dermatologist’s office by his mother for evaluation of a rash on his hands. He complained of mild discomfort and a burning sensation on the palms. On examination, multiple vesicles with surrounding erythema were noted to predominantly affect the palms in a symmetrical distribution. He presented with odynophagia and 2 erosions on the buccal mucosa.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Hand, Foot and Mouth Disease
Hand, foot and mouth disease (HFMD) is a common enteroviral illness of childhood characterized by fever and classic cutaneous findings, which include a papulovesicular eruption on the palms and soles as well as an erosive stomatitis. Children under the age of 10 are usually affected, although HFMD has also been described in immunocompetent adolescents and adults.1 Males and females are equally affected, and incidence is greatest during the summer and autumn months.2 The virus is transmitted by respiratory and oral-fecal routes through contact with respiratory secretions, vesicular fluid, saliva and feces.
Coxsackievirus A16 is the most common cause of HFMD in the United States, but other non-polio enteroviruses, including coxsackieviruses A5-7, A9, A10, B11, B3, B5, echovirus 4 and enterovirus 71, have been implicated.2,3 Notably, enterovirus 71(EV71) infection is linked to large epidemics of the disease in Asian-Pacific countries and is associated with neurologic and systemic complications that can prove fatal.4-7 The prevalence of EV71 infection in this region has greatly increased since 1997, with large outbreaks reported in Japan, Malaysia, Singapore, South Korea, China and Australia. Although outbreaks of EV71-related HFMD have been noted in the aforementioned countries, no large-scale epidemics have been reported in the United States. Coxsackie A16 infection was largely thought to be free of these neurologic complications, but a recent study disputes that claim.8 It is difficult to assess the epidemiological details of HFMD in the United States, as countries have different reporting and surveillance practices. HFMD is not a notifiable disease in the United States and, therefore, the actual number of HFMD cases in the country is unknown.
Clinical Presentation
Clinically, hand, foot and mouth disease is characterized by a vesicular eruption on the palms and soles and an erosive stomatitis. A prodromal illness of fever, malaise and myalgias precedes the mucocutaneous findings by 1-4 days. Erythematous macules and papules evolve into 3-mm to 7-mm, grey to white, oval to football shaped vesicles with an erythematous halo on the palms and soles. Less commonly, the dorsal hands and feet are involved. A vesicular or morbilliform eruption may be present on the buttocks, genitalia, extremities and perianally. Enanthem, or mucosal eruption, is characterized by vesicles and erosions with surrounding erythema on the buccal mucosa, gingiva, tonsilar pillars, palate and uvula. The mucosal lesions usually precede the hand and foot findings but may be absent in some individuals.1 Lesions can be asymptomatic or associated with pain from touch or pressure. The illness is usually mild with resolution of symptoms within 7-14 days. Onychomadesis may result 1-2 months after resolution of the exanthem.
During outbreaks of the EV71 virus in Asian-Pacific countries, thousands of children developed mild, self-limited HFMD. However, a small proportion of cases rapidly become associated with neurological and systemic complications that can be fatal. Infection with EV71 has been linked with severe symptoms including aseptic meningitis, flaccid paralysis, pulmonary edema, brainstem encephalitis and cardiopulmonary collapse.4-7,9 A large, prospective, study of several epidemics that occurred over 7 years in Malaysia showed 10%–30% of children hospitalized with EV71-related HFMD developed CNS complications.10 Brainstem encephalitis was the most frequent presentation, accounting for 58% of neurological manifestations, followed by aseptic meningitis (36%) and brainstem encephalitis with cardiorespiratory dysfunction (4%).9 Most children with CNS involvement had concurrent clinical features of HFMD, but a small proportion presented only with neurological features. Myoclonic jerks are seen more often in EV71 infection compared to other enteroviruses and could be an early indicator of neurological involvement.10
Brainstem encephalitis associated with cardiopulmonary dysfunction has become a notable feature in EV71 epidemics in Asia and is the primary cause of death. Exact statistics of this entity are difficult to assess based on the current literature. A Malaysian study found 4% of children with neurologic manifestations developed brainstem encephalitis and cardiorespiratory dysfunction.9 A Tawainese study found 10 out of 97 patients developed the entity.11 Children typically present with a brief febrile illness, clinical features of HFMD and mild neurological symptoms. A sudden deterioration is noted after 3-5 days; without swift intervention in the ICU, this manifestation can result in death.
 Differential Diagnoses
Differential Diagnoses
Overlapping clinical features may be seen in herpangina, herpes simplex virus, Kawasaki disease, alternative enteroviral infections and other viral exanthems, including measles and rubella (Table 1).
Histopathology
Histopathologic findings are not diagnostic for HFMD. Biopsy reveals an intra-epidermal vesicle, ballooning degeneration of keratinocytes, epidermal necrosis and marked papillary edema. A non-specific dermal inflammatory infiltrate is present. Viral inclusion bodies and giant cells are not appreciated.
Diagnosis and Management
Hand, foot and mouth disease is primarily a clinical diagnosis. When necessary, the virus can be isolated through culture or polymerase chain reaction of oropharyngeal secretions, vesicular fluid or feces. The disease usually has a benign, self-limited clinical course. Supportive measures and symptomatic management will normally suffice. However, in cases of enterovirus 71 infection complicated by severe neurologic and systemic sequelae, hospitalization and possible mechanical ventilation may be required.
No established antiviral treatment exists for EV71 infection, although several treatments have been tried. Pleconaril is an antiviral medication that inhibits the entry of several enteroviruses into cells by blocking viral attachment and uncoating. It has been used in clinical trials for aseptic meningitis and was once thought to be a promising treatment for EV71 infection. However, a recent study revealed pleconaril does not appear to be active against the EV71 strain.12
Intravenous immunoglobulin has been shown to be of benefit when given early in the disease course13,14 and is used on the presumptive basis that it neutralizes EV71 and has non-specific anti-inflammatory properties. One retrospective comparison in Malaysia showed 204 (95%) of 215 survivors who had severe CNS complications had received intravenous immunoglobulin treatment in comparison to only one (11%) of 9 fatal cases.14 No randomized trials have been undertaken, but intravenous immunoglobulin is being more routinely used. Other treatments being explored include ribavirin, interferons and RNA interference.15-18
Proper hygiene helps to prevent transmission. HFMD is most contagious during the presence of cutaneous symptoms, but the virus can be shed for weeks after vesicular resolution. As a result, it is ineffective to keep children sequestered from school after the initial cutaneous findings have resolved.
In our patient, the clinical symptoms resolved within 2 weeks without sequelae.
Conclusion
HFMD is a common pediatric enteroviral illness that usually follows a benign, self-limited course. However, clinicians should be aware of other enteroviral strains with neurologic and systemic sequelae, namely EV71, that have resulted in epidemics in Asian-Pacific countries.
Dr. Wright is a second-year dermatology resident at the State University of New York Downstate in Brooklyn, NY.
Dr. Ehrsam is a dermatologist in Lille, France.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Shin JU, Oh SH, Lee JH. A case of hand-foot-mouth disease in an immunocompetent adult. Ann Dermatol. 2010;22(2):216-218. doi: 10.5021/ad.2010.22.2.216. Epub 2010 May 18.
2. Centers of Disease Control and Prevention. Hand, foot and mouth disease. Available at: https://www.cdc.gov/hand-foot-mouth/index.html. Accessibility verified March 21, 2013.
3. Wu Y, Yeo A, Phoon MC, et al. The largest outbreak of hand; foot and mouth disease in Singapore in 2008: The role of enterovirus 71 and coxsackievirus A strains. Int J Infect Dis. 2010;14(12):e1076-e1081. doi: 10.1016/j.ijid.2010.07.006. Epub 2010 Oct 16.
4. Chan KP, Goh KT, Chong CY, Teo ES, Lau G, Ling AE. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infect Dis. 2003;9(1):78–85.
5. Lin TY, Twu SJ, Ho MS, Chang LY, Lee CY. Enterovirus 71 outbreaks, Taiwan: Occurrence and recognition. Emerg Infect Dis. 2003;9(3):291–293.
6. Ho M. Enterovirus 71: The virus, its infections and outbreaks. J Microbiol Immunol Infect. 2000;33(4):205–216.
7. Chan LG, Parashar UD, Lye MS, et al. Deaths of children during an outbreak of hand, foot, and mouth disease in Sarawak, Malaysia: Clinical and pathological characteristics of the disease. For the Outbreak Study Group. Clin Infect Dis. 2000;31(3):678–683.
8. Xu W, Liu CF, Yan L, et al. Distribution of enteroviruses in hospitalized children with hand, foot and mouth disease and relationship between pathogens and nervous system complications. Virol J. 2012;9;9(1):8. doi: 10.1186/1743-422X-9-8.
9. Ooi MH, Wong SC, Lewthwaite P, Cardosa MJ, Solomon T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010;9(11):1097–1105. doi: 10.1016/S1474-4422(10)70209-X.
10. Ooi MH, Wong SC, Podin Y, et al. Human enterovirus 71 disease in Sarawak, Malaysia: A prospective clinical, virulogical and molecular epidemiological study. Clin Infect Dis. 2007;44(5):646-656.
11. Wang SM, Liu CC, Tseng HW, et al. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurologic complications. Clin Infect Dis. 1999; 29(1):184-90.
12. Chen TC, Weng KF, Chang SC, Lin JY, Huang PN, Shih SR. Development of antiviral agents for enteroviruses. J Antimicrob Chemother. 2008 Dec;62(6):1169–1173. doi: 10.1093/jac/dkn424. Epub 2008 Oct 18.
13. Chang LY, Hsia SH, Wu CT, et al. Outcome of enterovirus 71 infections with or without stage-based management: 1998 to 2002. Pediatr Infect Dis J. 2004;23(4):327–332.
14. Ooi MH, Wong SC, Mohan A, et al. Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot, and mouth disease in Sarawak. BMC Infect Dis. 2009 Jan 19;9:3. doi: 10.1186/1471-2334-9-3.
15. Li ZH, Li CM, Ling P, et al. Ribavirin reduces mortality in enterovirus 71-infected mice by decreasing viral replication. J Infect Dis. 2008;197(6):854–857. doi: 10.1086/527326.
16. Liu ML, Lee YP, Wang YF, et al. Type I interferons protect mice against enterovirus 71 infection. J Gen Virol. 2005;86(Pt 12):3263–3269.
17. Sim AC, Luhur A, Tan TM, Chow VT, Poh CL. RNA interference against enterovirus 71 infection. Virology. 2005;341(1):72–79.
18. Wu Z, Yang F, Zhao R, Zhao L, Guo D, Jin Q. Identification of small interfering RNAs which inhibit the replication of several Enterovirus 71 strains in China. J Virol Methods. 2009;159(2):233–238. doi: 10.1016/j.jviromet.2009.04.002. Epub 2009 Apr 10.
PATIENT PRESENTATION
A 5-year-old boy was brought to the dermatologist’s office by his mother for evaluation of a rash on his hands. He complained of mild discomfort and a burning sensation on the palms. On examination, multiple vesicles with surrounding erythema were noted to predominantly affect the palms in a symmetrical distribution. He presented with odynophagia and 2 erosions on the buccal mucosa.
WHAT IS YOUR DIAGNOSIS?
DIAGNOSIS: Hand, Foot and Mouth Disease
Hand, foot and mouth disease (HFMD) is a common enteroviral illness of childhood characterized by fever and classic cutaneous findings, which include a papulovesicular eruption on the palms and soles as well as an erosive stomatitis. Children under the age of 10 are usually affected, although HFMD has also been described in immunocompetent adolescents and adults.1 Males and females are equally affected, and incidence is greatest during the summer and autumn months.2 The virus is transmitted by respiratory and oral-fecal routes through contact with respiratory secretions, vesicular fluid, saliva and feces.
Coxsackievirus A16 is the most common cause of HFMD in the United States, but other non-polio enteroviruses, including coxsackieviruses A5-7, A9, A10, B11, B3, B5, echovirus 4 and enterovirus 71, have been implicated.2,3 Notably, enterovirus 71(EV71) infection is linked to large epidemics of the disease in Asian-Pacific countries and is associated with neurologic and systemic complications that can prove fatal.4-7 The prevalence of EV71 infection in this region has greatly increased since 1997, with large outbreaks reported in Japan, Malaysia, Singapore, South Korea, China and Australia. Although outbreaks of EV71-related HFMD have been noted in the aforementioned countries, no large-scale epidemics have been reported in the United States. Coxsackie A16 infection was largely thought to be free of these neurologic complications, but a recent study disputes that claim.8 It is difficult to assess the epidemiological details of HFMD in the United States, as countries have different reporting and surveillance practices. HFMD is not a notifiable disease in the United States and, therefore, the actual number of HFMD cases in the country is unknown.
Clinical Presentation
Clinically, hand, foot and mouth disease is characterized by a vesicular eruption on the palms and soles and an erosive stomatitis. A prodromal illness of fever, malaise and myalgias precedes the mucocutaneous findings by 1-4 days. Erythematous macules and papules evolve into 3-mm to 7-mm, grey to white, oval to football shaped vesicles with an erythematous halo on the palms and soles. Less commonly, the dorsal hands and feet are involved. A vesicular or morbilliform eruption may be present on the buttocks, genitalia, extremities and perianally. Enanthem, or mucosal eruption, is characterized by vesicles and erosions with surrounding erythema on the buccal mucosa, gingiva, tonsilar pillars, palate and uvula. The mucosal lesions usually precede the hand and foot findings but may be absent in some individuals.1 Lesions can be asymptomatic or associated with pain from touch or pressure. The illness is usually mild with resolution of symptoms within 7-14 days. Onychomadesis may result 1-2 months after resolution of the exanthem.
During outbreaks of the EV71 virus in Asian-Pacific countries, thousands of children developed mild, self-limited HFMD. However, a small proportion of cases rapidly become associated with neurological and systemic complications that can be fatal. Infection with EV71 has been linked with severe symptoms including aseptic meningitis, flaccid paralysis, pulmonary edema, brainstem encephalitis and cardiopulmonary collapse.4-7,9 A large, prospective, study of several epidemics that occurred over 7 years in Malaysia showed 10%–30% of children hospitalized with EV71-related HFMD developed CNS complications.10 Brainstem encephalitis was the most frequent presentation, accounting for 58% of neurological manifestations, followed by aseptic meningitis (36%) and brainstem encephalitis with cardiorespiratory dysfunction (4%).9 Most children with CNS involvement had concurrent clinical features of HFMD, but a small proportion presented only with neurological features. Myoclonic jerks are seen more often in EV71 infection compared to other enteroviruses and could be an early indicator of neurological involvement.10
Brainstem encephalitis associated with cardiopulmonary dysfunction has become a notable feature in EV71 epidemics in Asia and is the primary cause of death. Exact statistics of this entity are difficult to assess based on the current literature. A Malaysian study found 4% of children with neurologic manifestations developed brainstem encephalitis and cardiorespiratory dysfunction.9 A Tawainese study found 10 out of 97 patients developed the entity.11 Children typically present with a brief febrile illness, clinical features of HFMD and mild neurological symptoms. A sudden deterioration is noted after 3-5 days; without swift intervention in the ICU, this manifestation can result in death.
Differential Diagnoses
Overlapping clinical features may be seen in herpangina, herpes simplex virus, Kawasaki disease, alternative enteroviral infections and other viral exanthems, including measles and rubella (Table 1).
Histopathology
Histopathologic findings are not diagnostic for HFMD. Biopsy reveals an intra-epidermal vesicle, ballooning degeneration of keratinocytes, epidermal necrosis and marked papillary edema. A non-specific dermal inflammatory infiltrate is present. Viral inclusion bodies and giant cells are not appreciated.
Diagnosis and Management
Hand, foot and mouth disease is primarily a clinical diagnosis. When necessary, the virus can be isolated through culture or polymerase chain reaction of oropharyngeal secretions, vesicular fluid or feces. The disease usually has a benign, self-limited clinical course. Supportive measures and symptomatic management will normally suffice. However, in cases of enterovirus 71 infection complicated by severe neurologic and systemic sequelae, hospitalization and possible mechanical ventilation may be required.
No established antiviral treatment exists for EV71 infection, although several treatments have been tried. Pleconaril is an antiviral medication that inhibits the entry of several enteroviruses into cells by blocking viral attachment and uncoating. It has been used in clinical trials for aseptic meningitis and was once thought to be a promising treatment for EV71 infection. However, a recent study revealed pleconaril does not appear to be active against the EV71 strain.12
Intravenous immunoglobulin has been shown to be of benefit when given early in the disease course13,14 and is used on the presumptive basis that it neutralizes EV71 and has non-specific anti-inflammatory properties. One retrospective comparison in Malaysia showed 204 (95%) of 215 survivors who had severe CNS complications had received intravenous immunoglobulin treatment in comparison to only one (11%) of 9 fatal cases.14 No randomized trials have been undertaken, but intravenous immunoglobulin is being more routinely used. Other treatments being explored include ribavirin, interferons and RNA interference.15-18
Proper hygiene helps to prevent transmission. HFMD is most contagious during the presence of cutaneous symptoms, but the virus can be shed for weeks after vesicular resolution. As a result, it is ineffective to keep children sequestered from school after the initial cutaneous findings have resolved.
In our patient, the clinical symptoms resolved within 2 weeks without sequelae.
Conclusion
HFMD is a common pediatric enteroviral illness that usually follows a benign, self-limited course. However, clinicians should be aware of other enteroviral strains with neurologic and systemic sequelae, namely EV71, that have resulted in epidemics in Asian-Pacific countries.
Dr. Wright is a second-year dermatology resident at the State University of New York Downstate in Brooklyn, NY.
Dr. Ehrsam is a dermatologist in Lille, France.
Dr. Khachemoune, the Section Editor of Derm DX, is with the Department of Dermatology at the State University of New York Downstate in Brooklyn, NY.
Disclosures: The authors have no conflicts of interest to report.
References
1. Shin JU, Oh SH, Lee JH. A case of hand-foot-mouth disease in an immunocompetent adult. Ann Dermatol. 2010;22(2):216-218. doi: 10.5021/ad.2010.22.2.216. Epub 2010 May 18.
2. Centers of Disease Control and Prevention. Hand, foot and mouth disease. Available at: https://www.cdc.gov/hand-foot-mouth/index.html. Accessibility verified March 21, 2013.
3. Wu Y, Yeo A, Phoon MC, et al. The largest outbreak of hand; foot and mouth disease in Singapore in 2008: The role of enterovirus 71 and coxsackievirus A strains. Int J Infect Dis. 2010;14(12):e1076-e1081. doi: 10.1016/j.ijid.2010.07.006. Epub 2010 Oct 16.
4. Chan KP, Goh KT, Chong CY, Teo ES, Lau G, Ling AE. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infect Dis. 2003;9(1):78–85.
5. Lin TY, Twu SJ, Ho MS, Chang LY, Lee CY. Enterovirus 71 outbreaks, Taiwan: Occurrence and recognition. Emerg Infect Dis. 2003;9(3):291–293.
6. Ho M. Enterovirus 71: The virus, its infections and outbreaks. J Microbiol Immunol Infect. 2000;33(4):205–216.
7. Chan LG, Parashar UD, Lye MS, et al. Deaths of children during an outbreak of hand, foot, and mouth disease in Sarawak, Malaysia: Clinical and pathological characteristics of the disease. For the Outbreak Study Group. Clin Infect Dis. 2000;31(3):678–683.
8. Xu W, Liu CF, Yan L, et al. Distribution of enteroviruses in hospitalized children with hand, foot and mouth disease and relationship between pathogens and nervous system complications. Virol J. 2012;9;9(1):8. doi: 10.1186/1743-422X-9-8.
9. Ooi MH, Wong SC, Lewthwaite P, Cardosa MJ, Solomon T. Clinical features, diagnosis, and management of enterovirus 71. Lancet Neurol. 2010;9(11):1097–1105. doi: 10.1016/S1474-4422(10)70209-X.
10. Ooi MH, Wong SC, Podin Y, et al. Human enterovirus 71 disease in Sarawak, Malaysia: A prospective clinical, virulogical and molecular epidemiological study. Clin Infect Dis. 2007;44(5):646-656.
11. Wang SM, Liu CC, Tseng HW, et al. Clinical spectrum of enterovirus 71 infection in children in southern Taiwan, with an emphasis on neurologic complications. Clin Infect Dis. 1999; 29(1):184-90.
12. Chen TC, Weng KF, Chang SC, Lin JY, Huang PN, Shih SR. Development of antiviral agents for enteroviruses. J Antimicrob Chemother. 2008 Dec;62(6):1169–1173. doi: 10.1093/jac/dkn424. Epub 2008 Oct 18.
13. Chang LY, Hsia SH, Wu CT, et al. Outcome of enterovirus 71 infections with or without stage-based management: 1998 to 2002. Pediatr Infect Dis J. 2004;23(4):327–332.
14. Ooi MH, Wong SC, Mohan A, et al. Identification and validation of clinical predictors for the risk of neurological involvement in children with hand, foot, and mouth disease in Sarawak. BMC Infect Dis. 2009 Jan 19;9:3. doi: 10.1186/1471-2334-9-3.
15. Li ZH, Li CM, Ling P, et al. Ribavirin reduces mortality in enterovirus 71-infected mice by decreasing viral replication. J Infect Dis. 2008;197(6):854–857. doi: 10.1086/527326.
16. Liu ML, Lee YP, Wang YF, et al. Type I interferons protect mice against enterovirus 71 infection. J Gen Virol. 2005;86(Pt 12):3263–3269.
17. Sim AC, Luhur A, Tan TM, Chow VT, Poh CL. RNA interference against enterovirus 71 infection. Virology. 2005;341(1):72–79.
18. Wu Z, Yang F, Zhao R, Zhao L, Guo D, Jin Q. Identification of small interfering RNAs which inhibit the replication of several Enterovirus 71 strains in China. J Virol Methods. 2009;159(2):233–238. doi: 10.1016/j.jviromet.2009.04.002. Epub 2009 Apr 10.



 Differential Diagnoses
Differential Diagnoses







