


Off-Label Flow Diverter Stent as a Salvage Technique for Early Post-Liver Transplant Hepatic Arterial Occlusion: A Novel Technique
Key Summary
- A 58-year-old man developed early hepatic artery thrombosis/occlusion on postoperative day 5 after deceased-donor liver transplantation. Surgical thrombectomy, intraoperative thrombolysis, catheter-directed alteplase, and splenic artery embolization failed to restore flow.
- An off-label Pipeline Flex Embolization Device (Medtronic) was deployed across the transplant hepatic artery anastomosis. Immediate angiography showed restored antegrade hepatic arterial flow; Doppler ultrasound confirmed intrahepatic perfusion, liver enzymes normalized, and CT demonstrated a patent hepatic artery at 6 months.
- Authors describe flow diverter stenting as a potential bailout salvage technique when standard surgical/endovascular options are unsuccessful or unsuitable in early post-transplant hepatic artery occlusion. Evidence is limited to a single-patient case report; larger studies are needed to assess safety, durability, and generalizability.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Vascular Disease Management or HMP Global, their employees, and affiliates.
VASCULAR DISEASE MANAGEMENT. 2026;23(7):E92-E98
Abstract
Hepatic arterial flow in a transplanted liver is crucial. If there is any compromise in the flow, especially in the immediate postoperative period, it should be immediately addressed. We describe a case report where an off-label technique was performed using a flow diverter stent. The patient’s recovery was uneventful, and he was doing well at 6-month follow-up. The treatment options and choice of treatment are discussed
Introduction
Hepatic artery thrombosis (HAT) is the most critical arterial complication after liver transplantation. It is a major cause of graft loss, and early HAT requires urgent revascularization, traditionally with surgical revision.
Case Report
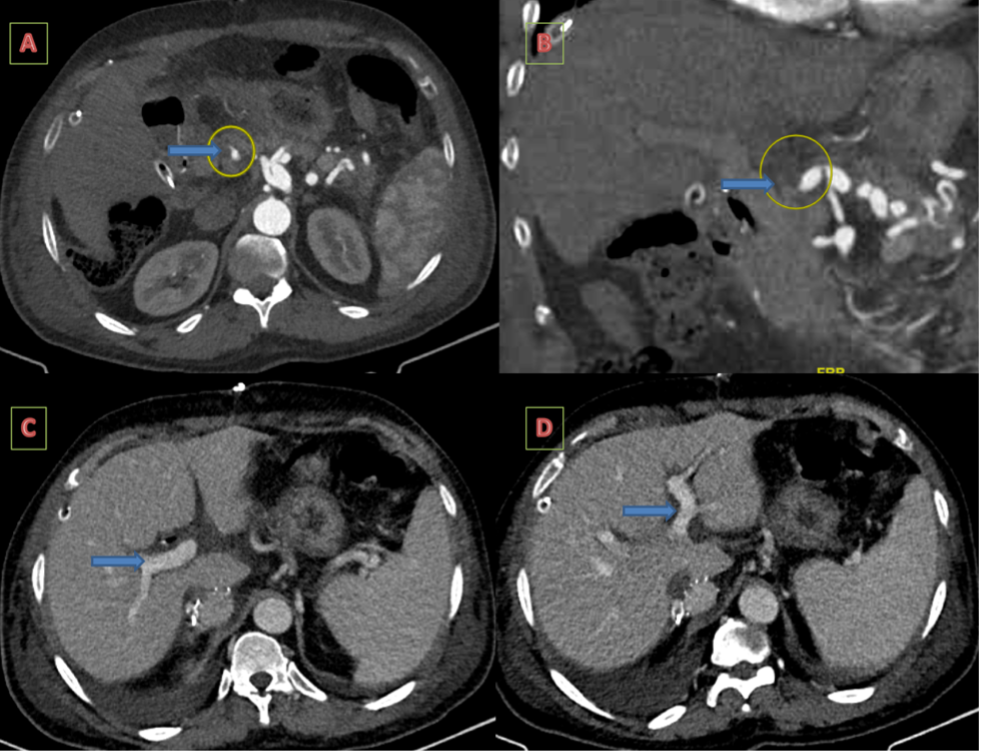
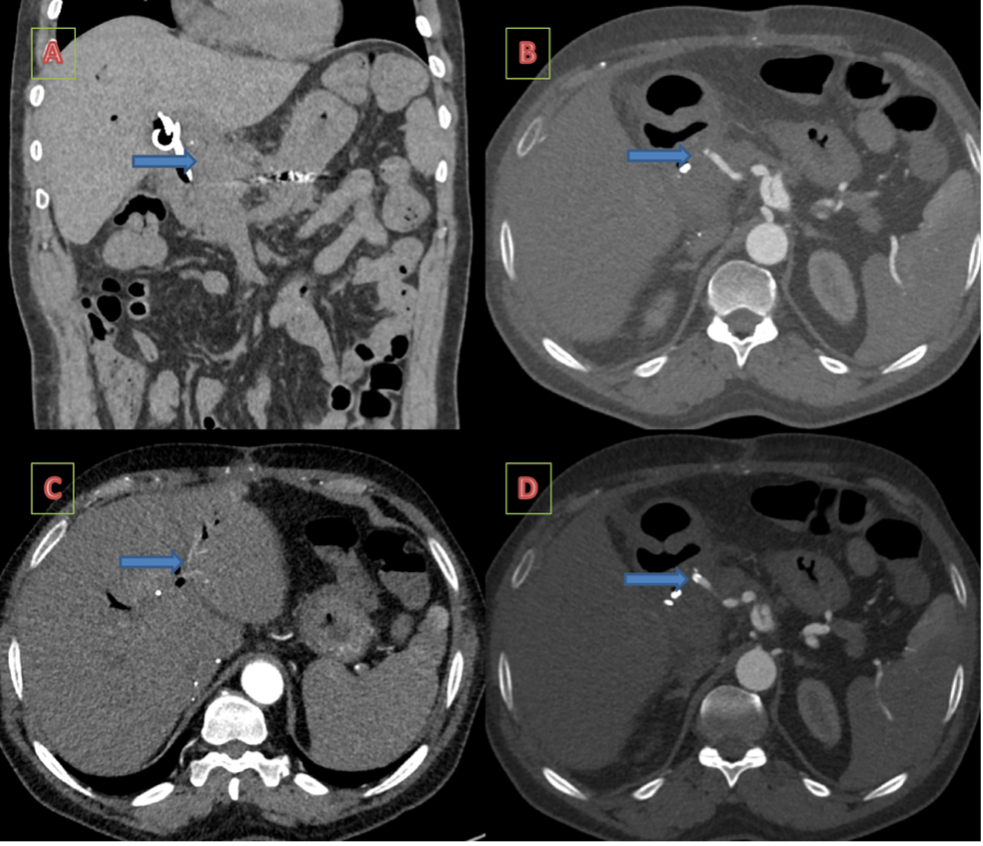
A 58-year-old man with autoimmune hepatitis and a previously ablated segment III hepatocellular carcinoma underwent deceased donor liver transplantation. The immediate postoperative course was uneventful. On postoperative day 5, there was no detectable flow in the hepatic artery on Doppler ultrasound. Liver enzymes were elevated (SGOT, 180; SGPT, 148; alkaline phosphatase, 797). Contrast-enhanced computed tomography (CECT) did not show any opacification of the hepatic artery distal to the anastomosis (Figure 1). The patient underwent emergency surgical re-exploration. Fogarty thrombectomy and intraoperative thrombolysis were attempted, but distal hepatic arterial flow could not be restored.
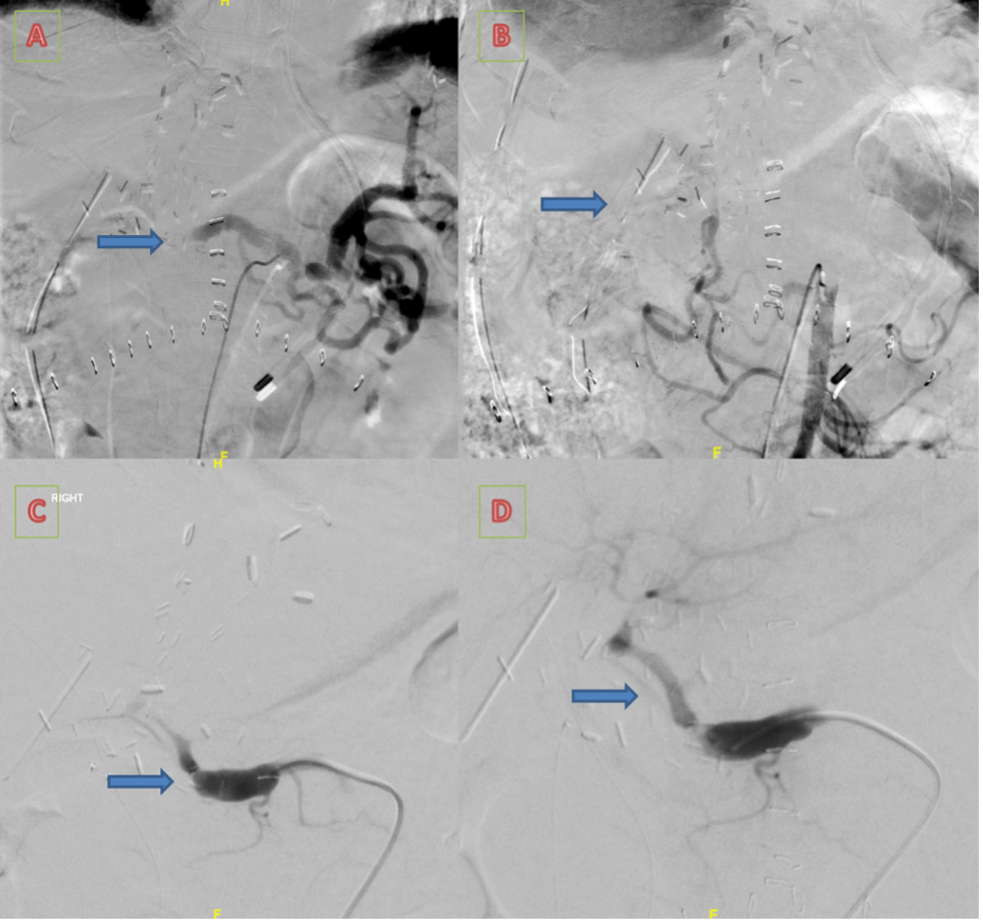
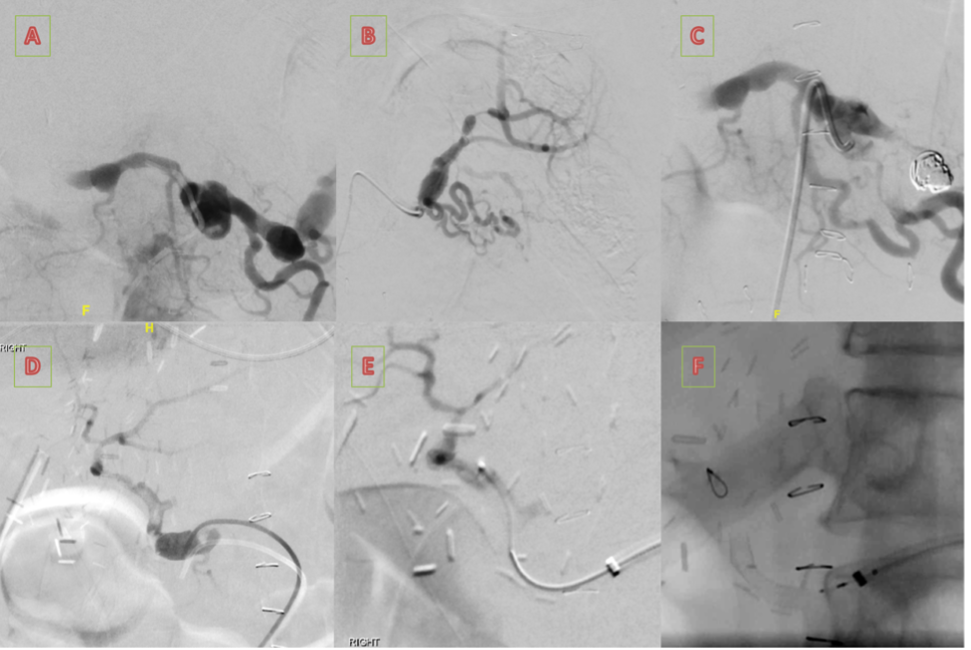
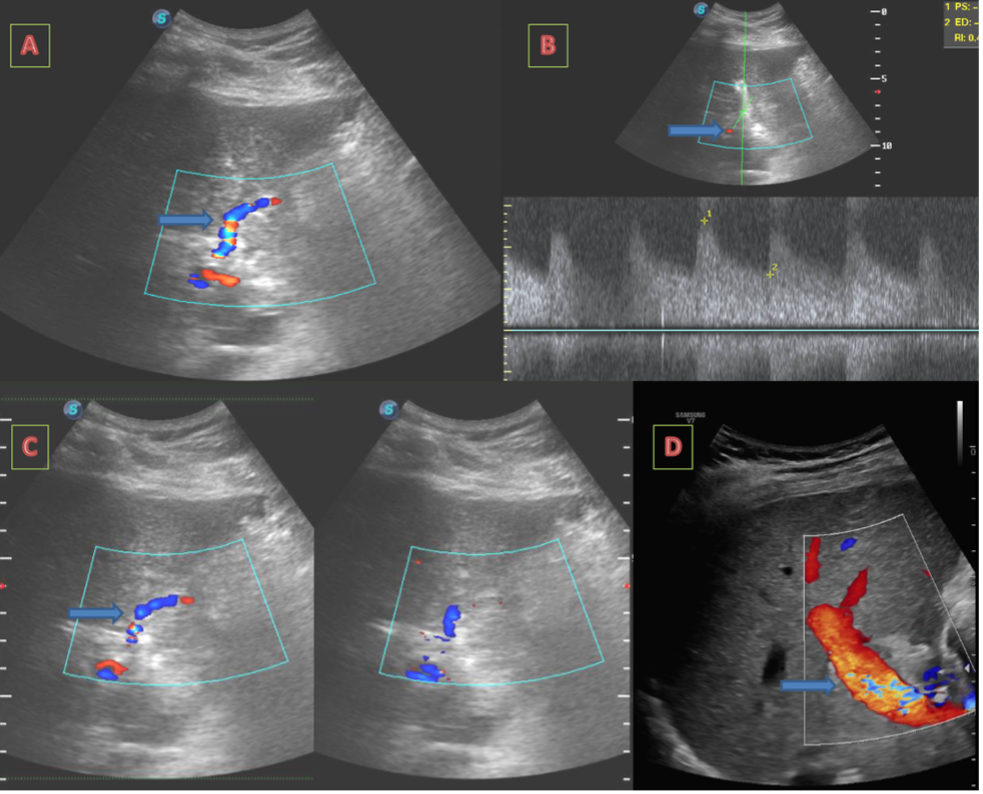
Diagnostic angiography showed complete occlusion at the anastomosis with retrograde splenic steal physiology (Figure 2). Catheter-directed thrombolysis with alteplase (10 mg over 12 hours) was initiated but discontinued due to drain-site bleeding. Repeat angiography again showed no antegrade hepatic inflow. Proximal splenic artery embolization was performed using coils to redirect flow; however, hepatic perfusion did not improve. The anastomosis was successfully crossed with a 3F Progreat microcatheter (Terumo). A balloon angioplasty was avoided as the anastomosis was very recent and had a risk of dehiscence or rupture. Given the persistent occlusion and failed conventional options, a 3.75 x 18-mm Pipeline Flex Embolization Device (PED) (Medtronic) was deployed across the anastomotic narrowing via a 6F long sheath positioned in the common hepatic artery (Figure 3 and Figure 4). The patient was given 300 mg aspirin intraprocedurally through a nasogastric tube. Immediate post-deployment angiography showed brisk antegrade flow through the stent into the left hepatic artery and its branches.
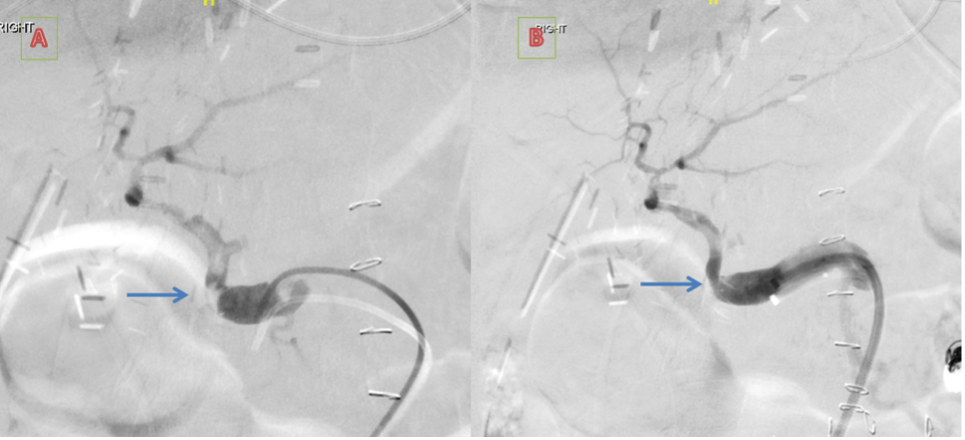
Postprocedural Doppler ultrasound demonstrated restored color flow within the intrahepatic branches (Figure 5). Liver enzymes normalized steadily. Oral aspirin 75 mg daily was given, and the patient was discharged in stable condition. The patient was asymptomatic on follow-up at 6 months; CECT showed a patent hepatic artery (Figure 6).
Discussion
Early HAT is reported in approximately 4% to 9% of liver transplant recipients and requires rapid intervention to prevent irreversible graft ischemia.1-3 Standard management includes surgical revision, thrombolysis, balloon angioplasty, or stent placement.4,5 However, interventions in the immediate postoperative period are challenging due to fragile anastomoses and altered hemodynamics.3-5
This patient presented a rare and technically complex scenario:
- fresh anastomosis precluding angioplasty
- angulation of the hepatic artery precluding the option of a covered stent, which is usually rigid
- failure of thrombectomy and thrombolysis
- persistent steal physiology despite splenic artery embolization
- persistent significant narrowing acting as a fixed outflow obstruction
Flow diverter stents were considered suitable in this context for the following reasons:
- self-expansile nature with low radial force, reducing mechanical stress on the anastomosis
- flexibility to conform to the angulation of the hepatic artery
- high mesh density redirecting laminar flow through the true lumen
- potential to scaffold the anastomosis without overexpansion
- proven track record in small-caliber, tortuous neurovascular arteries
PED is primarily used for treating intracranial aneurysms. However, evidence supporting its use in visceral arterial aneurysms and pseudoaneurysms is growing.6-10 Its deployment across a transplant hepatic artery in acute anastomotic narrowing has not been seen in the published literature.
Conclusion
Flow diverter stent placement may serve as an effective bailout option for early post-liver transplant HAT when surgical revision, thrombolysis, and standard endovascular techniques fail or are not suitable options.
Affiliations and Disclosures
At Christian Medical College, Vellore, Tamil Nadu, India, Santhosh Babu K.B, MBBS, MD, FNVIR, and Shyamkumar N. Keshava, MBBS, DMRD, DNB, FRCR, FRANZCR, are from the Department of Interventional Radiology; Ashish Goel, DM, MD, is from the Department of Hepatology; Ravish Raju, MBBS, is from the Department of Hepatobiliary Surgery; and Anu Eapen, DMRD, DNB, is from the Department of Radiodiagnosis.
The authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted May 5, 2026.
Address for correspondence: Shyamkumar N. Keshava, Department of Interventional Radiology, Christian Medical College, W4GP+7CW, Vellore, Tamil Nadu 632004 India. Email: shyankumar.n.keshava@gmail.com
References
1. Vignali C, Cioni R, Petruzzi P, et al. Role of interventional radiology in the management of vascular complications after liver transplantation. Transplant Proc. 2004;36(3):552-554. doi:10.1016/j.transproceed.2004.02.038
2. Naidu SG, Alzubaidi SJ, Patel IJ, et al. Interventional radiology management of adult liver transplant complications. Radiographics. 2022;42(6):1705-1723. doi:10.1148/rg.220011
3. Molvar C, Ogilvie R, Aggarwal D, Borge M. Transplant hepatic artery stenosis: endovascular treatment and complications. Semin Intervent Radiol. 2019;36(2):84-90. doi:10.1055/s-0039-1688420
4. Maaty MEGAE, Ibrahim AM, Soliman AH, Mohamed AH. Role of interventional radiology in management of post-liver transplant anastomotic complications. Egypt J Radiol Nucl Med. 2022;53(1):168. doi:10.1186/s43055-022-00853-6
5. Zammar SG, Buell TJ, Chen C, et al. Outcomes after off-label use of the Pipeline embolization device for intracranial aneurysms: a multicenter cohort study. World Neurosurg. 2018;115:e200-e205. doi:10.1016/j.wneu.2018.04.012
6. van Veenendaal P, Maingard J, Kok HK, et al. Endovascular flow-diversion of visceral and renal artery aneurysms using dual-layer braided nitinol carotid stents. CVIR Endovasc. 2020;3(1):33. doi:10.1186/s42155-020-00125-2
7. Patel PD, Chalouhi N, Atallah E, et al. Off-label uses of the Pipeline embolization device: a review of the literature. Neurosurg Focus. 2017;42(6):E4. doi:10.3171/2017.3.FOCUS1742
8. Murray TÉ, Brennan P, Maingard JT, et al. Treatment of visceral artery aneurysms using novel neurointerventional devices and techniques. J Vasc Interv Radiol. 2019;30(9):1407-1417. doi:10.1016/j.jvir.2018.12.733
9. Rabuffi P, Bruni A, Antonuccio EGM, Ambrogi C, Vagnarelli S. Treatment of visceral artery aneurysms and pseudoaneurysms with the use of cerebral flow diverting stents: initial experience. CVIR Endovasc. 2020;3(1):48. doi:10.1186/s42155-020-00137-y
10. Pothula V, Ray N, Dhanasekaran J, Sekar S, Joseph S. Endovascular repair of anastomotic pseudoaneurysms in a transplant renal artery using flow-diverter stents. J Vasc Interv Radiol. 2023;34(4):719-721. doi:10.1016/j.jvir.2022.05.027




