The Diabetic Foot Valley Project: A Bottom-Up Model for a Multidisciplinary Community of Care for the Management of Diabetic Foot Syndrome in Tuscany
Abstract
Objective: To implement the regional organization of diabetic foot syndrome (DFS) care, diabetologists of the Tuscany Regional Health Service (RHS) realized an initiative called the Diabetic Foot Valley Project (DFV) to create a community of practice including physicians, nurses, and podiatrists. Methods: The project began in 2022 with the organization of 3 meetings focused on acute, subacute, and chronic DFS. These meetings identified critical issues, and the results were used to develop improvement projects (IPs) focused on these issues in 2023 and 2024. The results of the IPs will be evaluated upon completion and compared with initial results to assess progress. Results: The focus groups identified IPs related to revascularization, emergency case management, offloading, local care and hospital-community networks, primary prevention and early diagnosis, and rehabilitation. Another project involves the development of a dedicated electronic platform accessible to all DFV centers. Discussion: Completed IPs focus on revascularization, surgical management, offloading, and local care and networking, including the design and implementation of a dedicated electronic platform. Those focused on screening and prevention and on rehabilitation and follow-up are currently being implemented and are expected to begin in early 2026. Conclusion: The project promoted in the Methods section and sponsored by Regione Toscana and the European Wound Management Association represents a pilot project that could serve as an example for similar experiences in other European countries for the implementation of international guidelines on DFS.
J CRIT LIMB ISCHEM 2026:6(2):E61-E69. doi: 10.25270/jcli/CLIG-2500013
Key words: diabetic foot, implementation, guidelines, chronic limb-threatening ischemia, revascularization
Introduction
Diabetic foot syndrome (DFS) is a complex, multifactorial condition that affects 25% of the diabetic population worldwide, at least once in their life. Due to its increasing incidence, severity, and progression, it is considered a clinical emergency, with a 98% recurrence rate at 10 years of follow-up.1 It is the leading cause of nontraumatic lower limb extremity amputation worldwide, with a 20-fold greater risk for diabetic patients compared to the general population and a 60% 5-year mortality rate comparable to that of the most aggressive forms of cancer.2,3
In Italy, diabetes mellitus is a disease of social relevance, and a network of diabetes services within the Servizio Sanitario Nazionale were created following the introduction of a specific national law in the late 1980s and then incorporated into the National Health Plan of 1999 (Law 115 of 3/16/1987).4,5
In Tuscany, approximately 250,000 inhabitants are diabetic and of these, 15,000 have DFS. This led to the establishment of diabetic foot prevention and treatment services at regional diabetes departments since the early 1990s.6 In 2003, thanks to a regional law (DLR 1304 of 12/9/2003) promoted by diabetologists and implemented by the regional health authority, regional organizational guidelines were defined based on the international guidelines of the International Working Group on the Diabetic Foot.7 This law was then updated in 2016 (DLR 698 of 7/19/2016) to adapt it to the new organizational model in 3 macro-areas of the RHS.8
Despite promising intentions, the regional guidelines have not been implemented, resulting in a clear gap in treatment and outcomes among regional centers.9,10 In particular, the analysis of the quality of outcomes in the Tuscany Regional Health System, conducted annually by the MeS Laboratory of Scuola Superiore di Studi Universitari e di Perfezionamento Sant’Anna, an independent auditor of the RHS, showed that the number of major amputations remained high, as did variations in performance related to diabetic foot management such as revascularization procedures.11
The inconsistency between the guideline theory and the reality of diabetic foot care in Tuscany became more evident during the COVID-19 pandemic, when available resources were diverted to combat the emergency at the expense of other conditions such as DFS, resulting in a 47% increase in lower limb amputations and a 62% increase in deaths compared to pre-COVID years.12
For this reason, diabetologists affiliated with the Tuscany Region’s diabetes services felt the need to unite to launch the Diabetic Foot Valley Project (DFV). The aim of the project is to overcome regional differences and implement existing guidelines into clinical practice, creating an integrated practice network that includes all professionals working in the regional health care system specializing in diabetic foot care: doctors (MDs), nurses (RNs), and podiatrists (DPMs), according to the indications of the Regional Guidelines (Appendix 1).
Methods
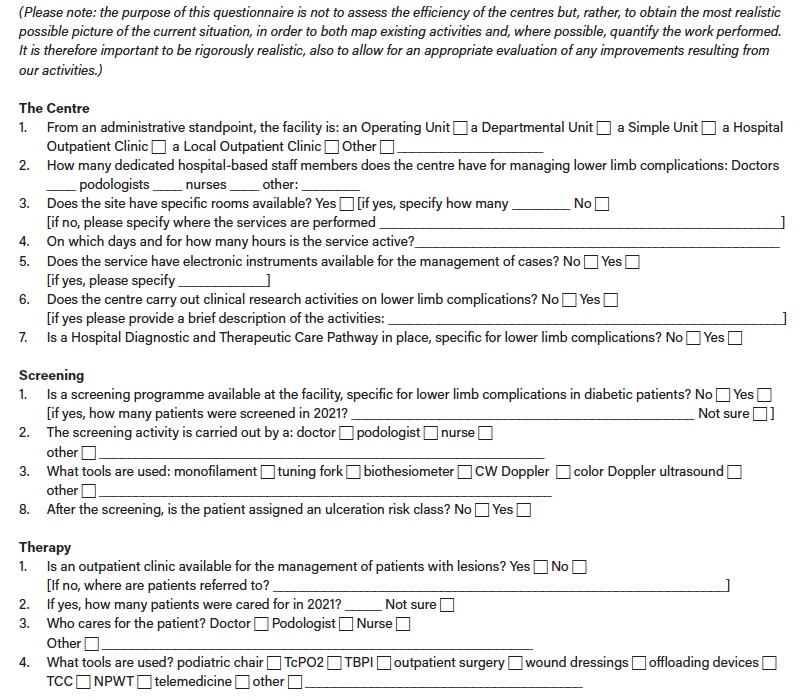
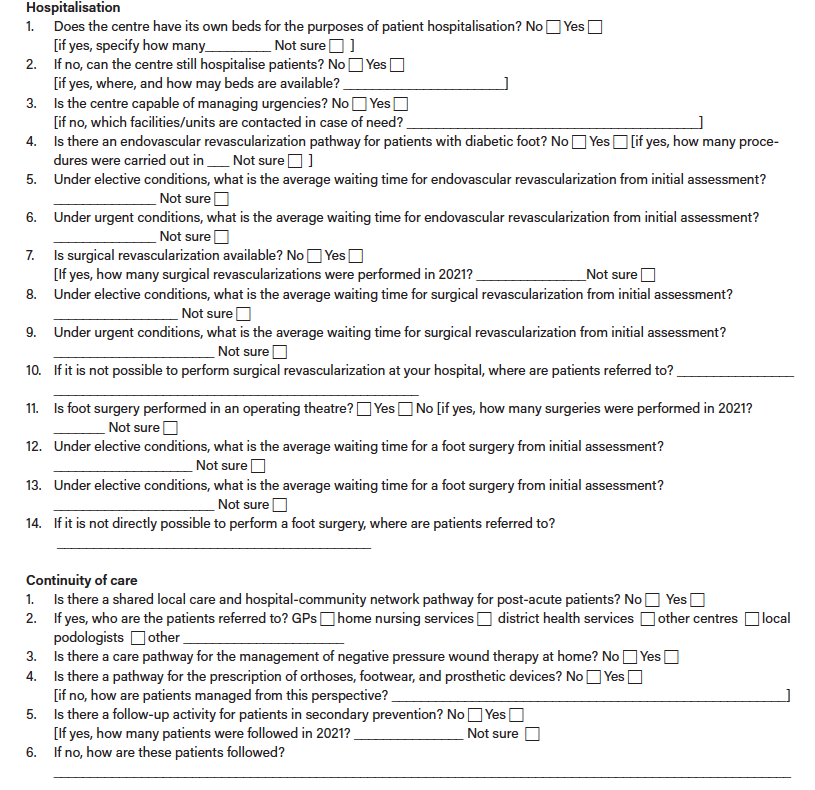
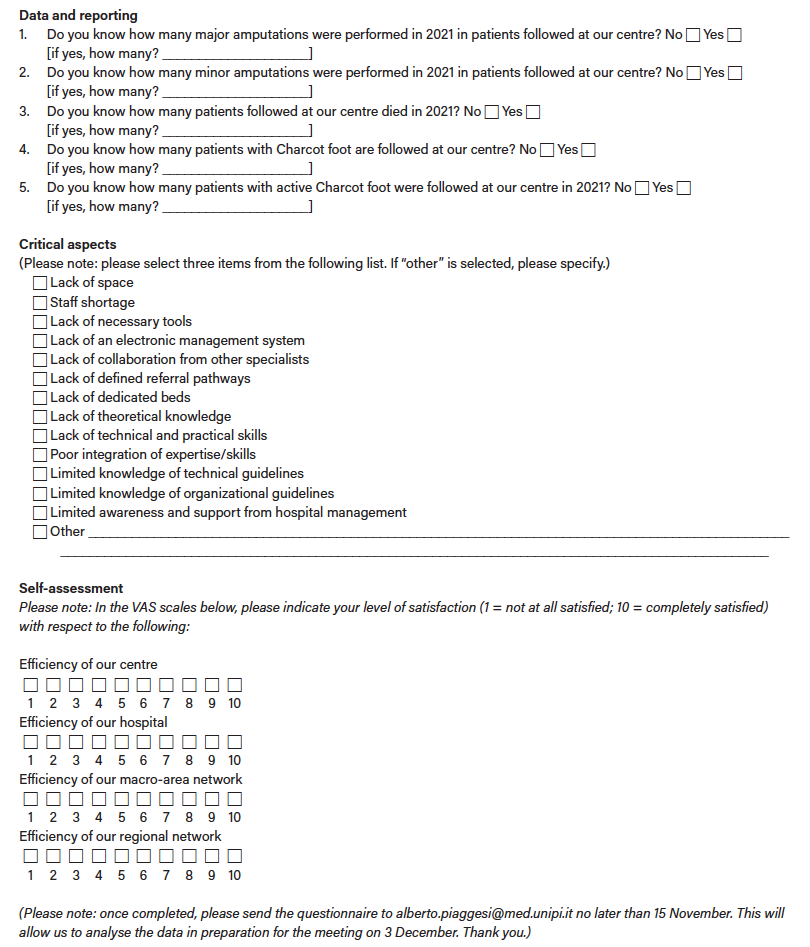
After an initial informal meeting held in Pisa in July 2022, which involved only the members of the DFV board, it was decided to distribute an online questionnaire to the 15 public diabetes services of the Tuscany RHS (Appendix 2). The goal was to outline the diabetes care pathways for each center, quantify ongoing activities, and identify critical issues. The questionnaire, structured into 3 distinct parts, asked health care professionals at each center to self-assess their interest in both patients and clinical practice and to rank the most critical aspects of diabetic foot management in order of importance, both from a clinical and managerial point of view. Among the various aspects considered, those deemed essential were availability of dedicated spaces and suitable equipment, screening, hospitalizations and visits, revascularization procedures, surgical interventions, emergency room pathways, follow-up, and continuity of care. From the analysis of the data extrapolated from the questionnaires, a list of priorities to be addressed was drawn up, and consequently it was decided to organize 3 focus meetings that took place in Pisa on December 3, 2022, Arezzo on February 18, 2023, and Florence on April 15, 2023.
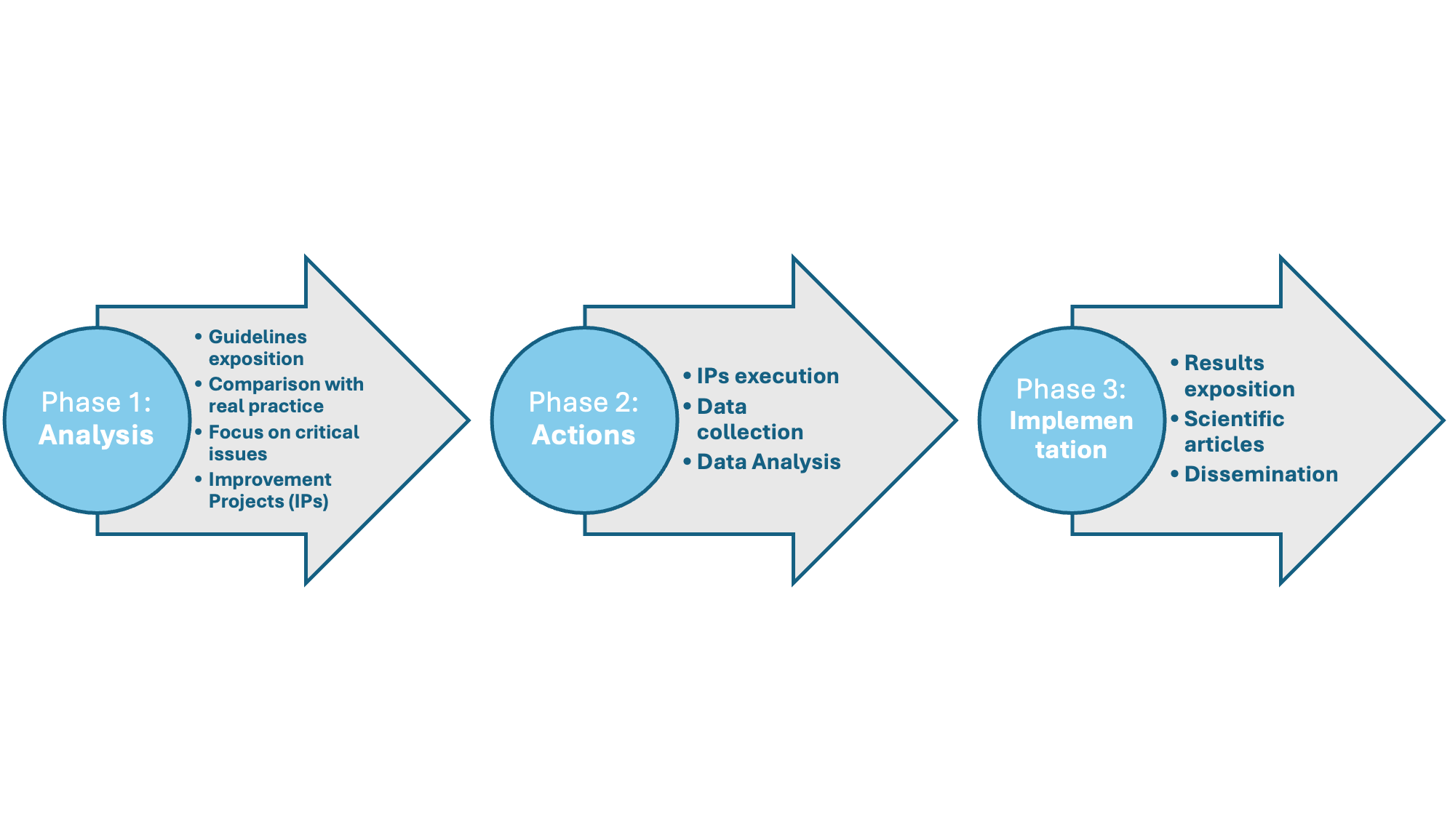
The aim of the meetings was to compare actual diabetic foot clinical practice with that theoretically defined by regional guidelines, as well as to discuss critical aspects, recognize and define barriers to best practices, and propose improvements. The meetings were held in an initial plenary session during which the results of the questionnaire were presented and the differences that emerged between the various centers involved in the survey were compared. Participants were then divided into 3 focus groups that met separately to discuss critical aspects related to acute, subacute, and chronic DFS. The aim of each focus group was to reach an internal consensus to initiate and subsequently develop improvement projects (IPs) to be developed over a 2- to 4-year period. The goal of the IPs was to update and standardize procedures and pathways with the model proposed by the regional guidelines.
The results obtained from the development and implementation of each individual IP will be evaluated and compared with the baseline data collected before the start of the project, as shown in Figure 1.
Results
The 3 meetings were attended by health care professionals from 15 Tuscan diabetes centers. The first meeting was attended by 62 health care professionals, comprising 47.5% MDs, 26.2% DPMs, and 26.3% RNs. In the second meeting, 68 health care professionals participated, distributed among 47.6% MDs, 21.9% DPMs, and 30.5% RNs. The third meeting was attended by 74 health care professionals, comprising 41% MDs, 19.7% DPMs, and 39.3% RNs. The rate of participants at the 3 meetings was 51.6%, 56.6%, and 61.6%, respectively, of the total amount of professionals working in the diabetes centers.
During the 3 meetings, the focus groups identified IPs related to the different phases of diabetic foot treatment. Specifically, one following the acute phase meeting focused on improving revascularization pathways, the management of urgent cases, and the management of patients with Charcot disease and acute DFS. Another one following the subacute meeting focused on local care, the use of negative pressure wound therapy (NPWT), and hospital-community collaboration for subacute DFS. Another one following the chronic phase meeting focused on primary prevention and early diagnosis, rapid referral, and rehabilitation of patients with chronic DFS.
Furthermore, the development of an improvement project covering all phases of DFS management has been defined as a priority. Specifically, this IP involves the development and implementation of a dedicated Regional Electronic Operational Instrument (software), which will serve as a case report form as well as a database of clinical, organizational, and econometric information to be shared by all the centers of the DFV community of practice. The results of the amelioration projects will be published in separate and dedicated articles.
Discussion
This paper presents the general outline of the DFV, which involves the 15 diabetes centers in the Tuscany region of Italy, with the shared goal of resolving discrepancies among the various centers and implementing existing regional guidelines.
For this reason, the project directly involved the Tuscany region and was presented to the General Director of the Tuscan Health Authority, who approved it and authorized the implementation and funding of an operational software (Regional Electronic Operational Instrument), managed by the Regional Department for Electronic Data Management, and a regional database for the management of patients with DFS in the public diabetes network as part of the Piano Nazionale di Ripresa e Resilienza.13 The electronic instrument will serve as a link between the various centers in the network and as a database for entering patient information, making it also available for analyzing the progress of other IPs.
This was the first step toward finalizing the project and represents the first IP developed and implemented. The other IPs arose from critical issues identified by the focus groups and were designed and developed to be completed within 2 to 4 years of initiation, depending on the complexity of the individual projects and the centers’ ability to gather information rapidly.
Each IP was conceived as a prospective interventional study in accordance with the principles of good clinical research practice and respecting patient privacy and dignity, in compliance with applicable laws and regulations.14,15
The results of each study are analyzed using a scientifically sound methodology and presented by the focus group that proposed it to a peer-reviewed journal. Some IPs, particularly those focused on revascularization, surgical management, offloading, local care, and networking, have already been completed. Those focused on screening and prevention, as well as rehabilitation and follow-up, are currently being implemented and are expected to begin in early 2026.
Based on the interpretation of DFS as a chronic remitting-relapsing disease rather than an acute one, some of the completed projects, particularly those related to the quality and quantity of interventional procedures in terms of revascularization and infection management, have been monitored by indicators that reflect not only the final outcome (eg, recovery, amputation, death) but also intermediate outcomes, such as referral delay, number of procedures per patient, recurrences, and complications.
Although this article does not intend to provide precise information on the results of individual IPs, it is interesting in this context to highlight the information on the baseline survey upon the revascularization procedures in Tuscany. The 15 centers of the RHS were asked to prospectively get information from 10 consecutive patients with chronic limb-threatening ischemia scheduled for endovascular revascularization.
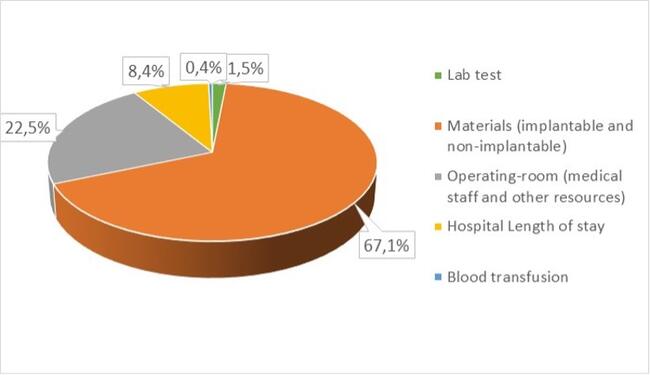
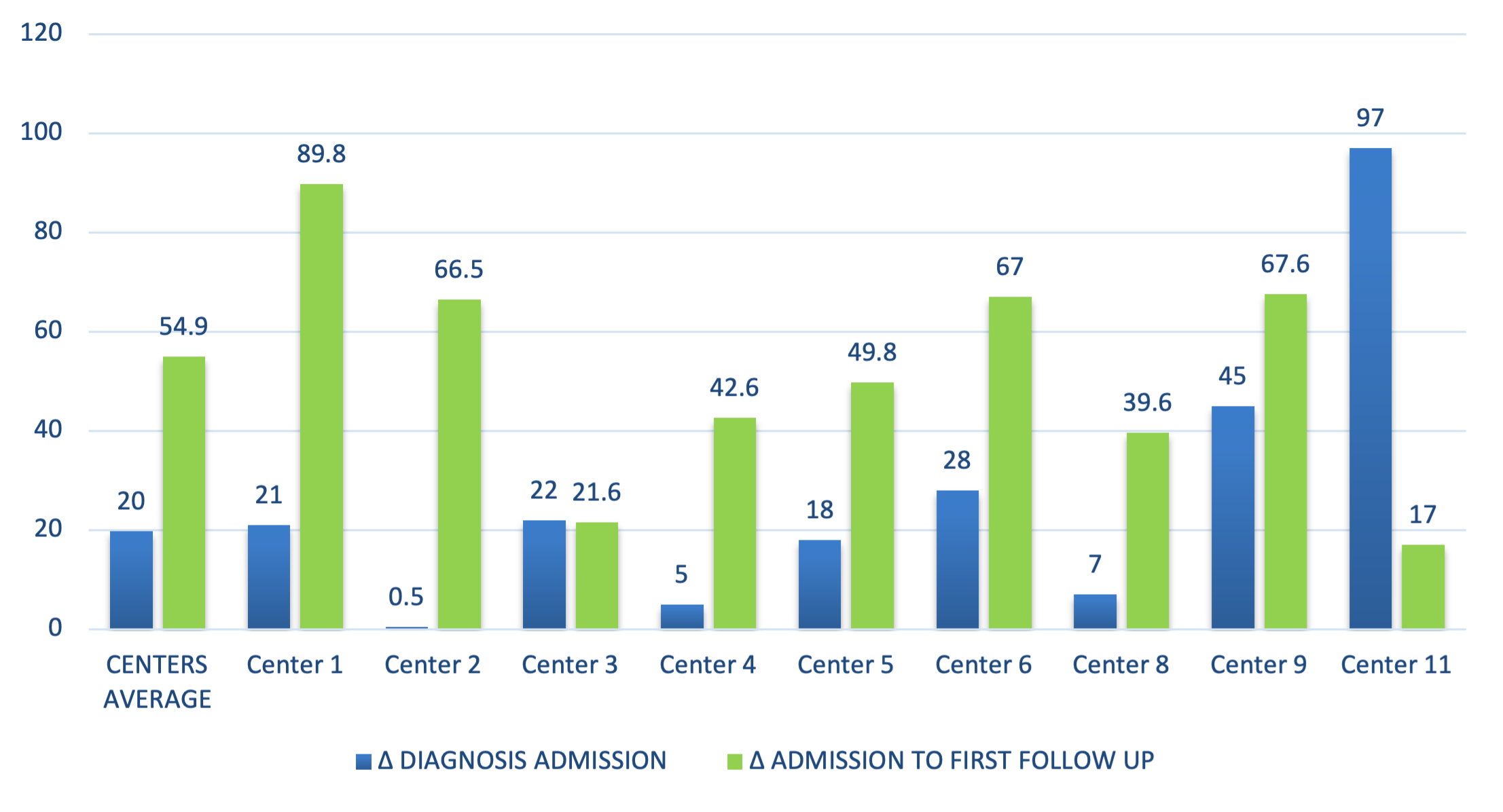
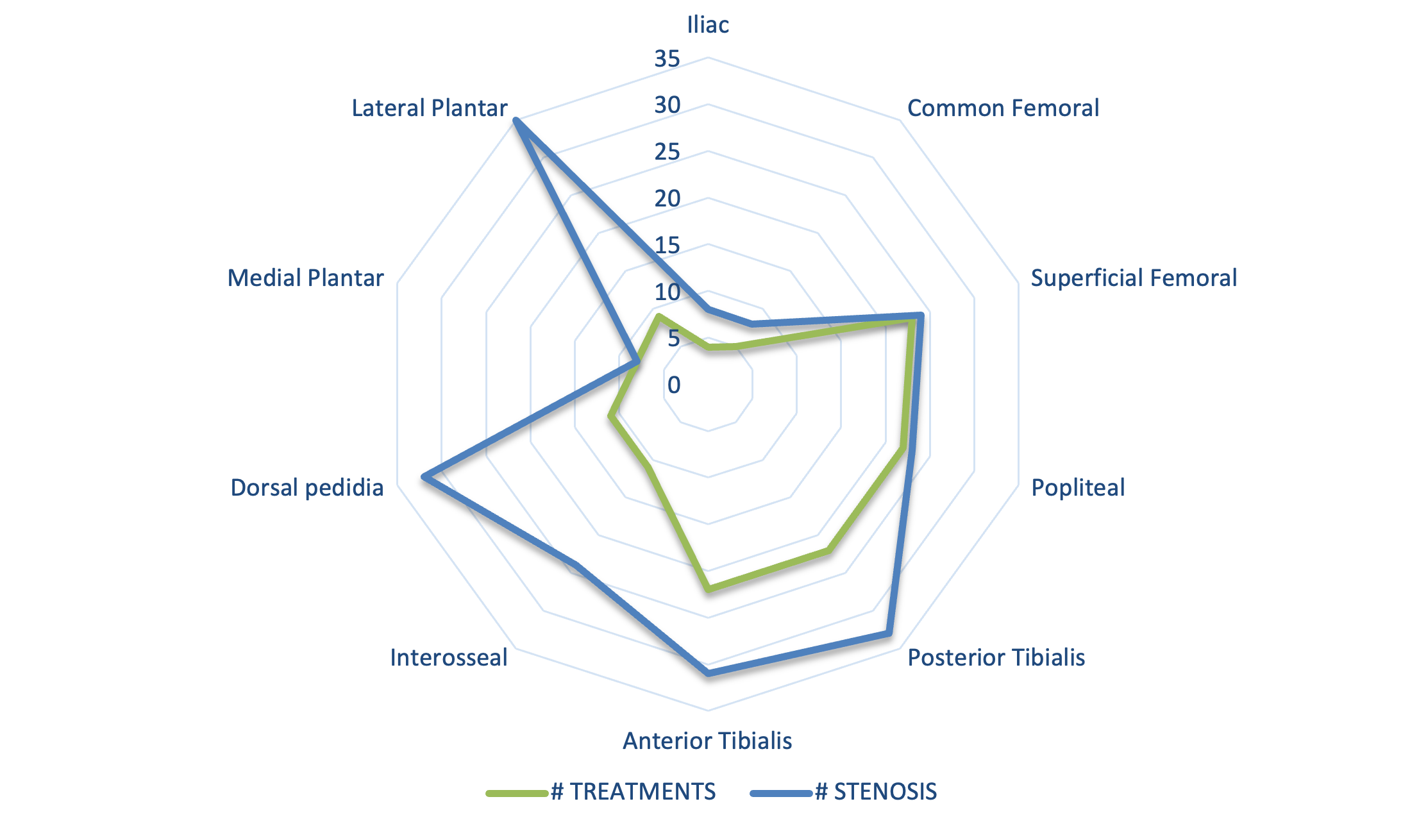
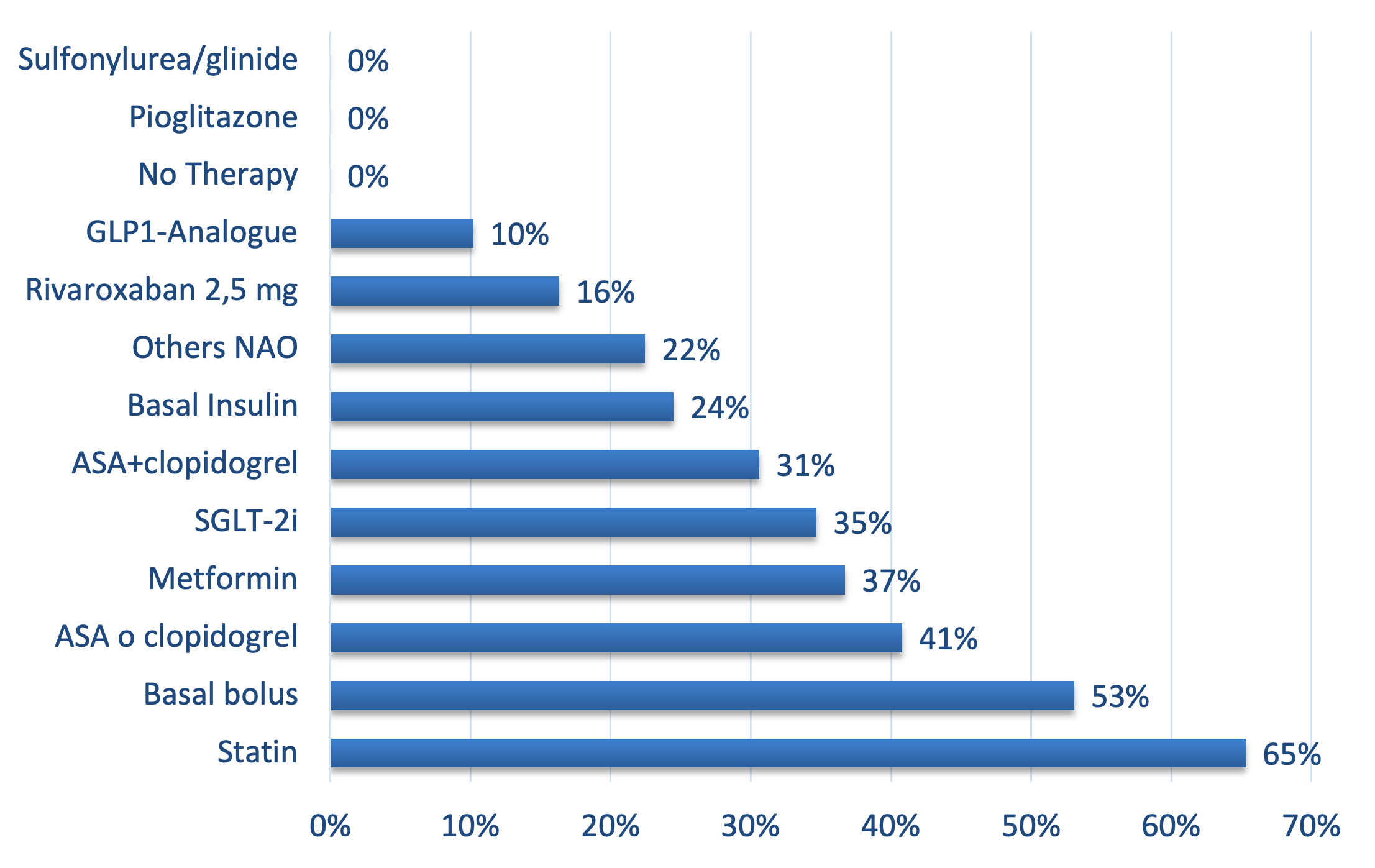
The data collected regarded the delay between the indication to revascularization, its actual execution and the first follow-up visit, the quality of revascularization, and the therapy at dismission. Beyond a wide variability among the centers, the results showed an average delay between indication to revascularization and its execution of 3 weeks and of 3 months for the first follow-up visit (Figure 2), a high prevalence of ineffective procedures, especially in the lower limb arteries (Figure 3), and a significant gap between the ideal therapy according to the cardiovascular and diabetology societies’ recommendations and the actual therapy prescribed at dismission to the patients (Figure 4).
The results of the IPs were presented and discussed in a dedicated conference in Pisa on March 1, 2025, which brought together all health care professionals involved in the DFV to discuss the project’s progress. At the same conference, participants were divided into 4 groups and had the opportunity to participate in 4 different interactive hands-on sessions focusing on patient screening and assessment, NPWT, advanced wound dressings, and acute and chronic diabetic foot offloading.
The results of the IPs will also be presented at scientific conferences organized by the European Wound Management Association (EWMA), which supports the DFV, considering it a model for improving patient outcomes, potentially applicable to other diseases and/or European regions, and capable of producing clinical and scientific data on a significant group of patients managed in a welfare-based health care system. This represents an opportunity to promote the debate on diabetic foot management in Europe and propose a methodology for improving the organization of diabetic foot management.
Conclusion
The DVF is an initiative initiated in Tuscany, Italy, by Tuscan diabetologists. Its goal is to create a community of health care professionals involved in the care of patients with DFS, improving prevention, early diagnosis, and treatment, and implementing clinical and organizational guidelines in a multidisciplinary clinical network within the Tuscany RHS. The IPs planned by the focus groups consider the critical issues identified by analyzing the existing situation and evaluate their effectiveness by comparing clinical and organizational parameters before and after the project implementation intervention. Furthermore, they will be discussed and published as the result of the work of the entire health care community. Finally, thanks to the support of the EWMA, the DFV could be considered a model for implementation in other European countries.
Affiliations and Disclosures
Elisa Amato, DPM, Francesco Giangreco, MD, and Alberto Piaggesi, MD, are from the Diabetic Foot Section, Department of Endocrinology and Metabolism, University of Pisa, Italy; Simone Barbagallo, PhD, is from the Hippocrates Research Society, Genova, Italy. See Appendix 1 for the list of members in The Diabetic Foot Valley Working Group.
The authors report no financial relationships or conflicts of interest regarding the content herein.
Dr Piaggesi designed the study, coordinated the project, analyzed the data, wrote and edited the manuscript; Dr Amato collected and analysed the data and wrote the manuscript; Dr Barbagallo collected and analysed the data; and Dr Giangreco collected and analysed the data and revised the manuscript.
The authors received no funding for this study.
Manuscript accepted March 23, 2026.
Address for correspondence: Elisa Amato, DPM, Diabetic Foot Section, Department of Endocrinology and Metabolism, University of Pisa, Via Mario Selli 1, 56124 Pisa, Italy. Email: elisa.amato92@gmail.com
Appendix 1. The Diabetic Foot Valley Working Group
Lorenza Abbruzzese, DPM (Pisa); Valeria Achilli, DPM (Piombino); Elisa Amato, DPM (Pisa); Laura Ambrosini Nobili, DPM (Pisa); Carmelina Amendola, RN (Prato); Michela Amendolia, DPM (Livorno); Roberto Anichini, MD (Pistoia); Matteo Apicella, DPM (Arezzo); Fabio Baccetti, MD (Carrara); Cristiana Baggiore, MD (Firenze); Elisa Banchellini, DPM (Lido di Camaiore); Valeria Barbaro, MD (Firenze); Genny Barnini, DPM (Empoli); Walter Baronti, DM (Grosseto); Eleonora Bastarelli, RN (Firenze); Roberto Becherini, MD (Pistoia); Arianna Bernini, DPM (Empoli); Stefania Bertoli, MD (Camaiore); Carlotta Bini, RN (Firenze); Sofia Butini, RN (Arezzo); Elisabetta Cacioli, RN (Grosseto); Maria Calabrese, MD (Prato); Michela Cameron Smith, MD (Firenze); Ilaria Casadidio, DPM (Lucca); Cristina Chelli, RN (Grosseto); Claudia Colombi, MD (Firenze); Alessandro Costa, DPM (Lido di Camaiore); Cristina Cossu, RN (Grosseto); Isabella Crisci, MD (Viareggio); Ilaria Cuccuru, DPM (Lucca) Giovanni De Gennaro, MD (Grosseto); Simona De Gregorio, DPM (Pontedera); Antonio De Luca, MD (Empoli); Elisa Del Bianco, RN (Lucca); Simone Della Valentina, DPM (Pisa); Arianna Desideri, DPM (Lucca); Alberto Di Carlo, MD (Lucca); Manuela Faenzi, RN (Firenze); Stefania Fanelli, PsyD (Arezzo); Cecilia Fondelli, MD (Siena); Francesco Giangreco, MD (Pisa); Romina Golini, RN (Arezzo); Chiara Goretti, MD (Pisa); Roberta Gori, RN (Firenze); Elisabetta Iacopi, MD (Pisa); Matteo Ieri, DPM (Firenze); Emilia Lacaria, DPM (Livorno); Cristina Landini, RN (Bordo San Lorenzo); Andrea Lazzeri, DPM (Firenze); Cristina Lencioni, MD (Lucca); Elisa Leporati, MD (Pisa); Teresa Leva, RN (Lucca); Monica Lorenzetti, MD (Prato); Linda Luppichini, DPM (Firenze); Silvia Magi, DPM (Arezzo); Dino Maionchi, MD (Lucca); Francesco Manetti, MD (Bagno a Ripoli); Michele Mantuano, MD (Arezzo); Elisa Marinelli, RN (Arezzo); Angela Marsocci, MD (Prato); Carmela Martinez, RN (Arezzo); Mary Mattesimi, RN (Arezzo); Matteo Monami, MD (Firenze); Marco Musco, DPM (Firenze); Barbara Neri, DPM (Prato); Rosa Nigro, RN (Arezzo); Besmir Nreu, DPM (Firenze); Margherita Occhipinti, MD (Empoli); Paola Orsini, MD (Livorno); Lavinia Palladino (Pisa); Cecilia Parra, DPM (Lucca); Marzia Piacentini, RN (Lucca); Alberto Piaggesi, MD (Pisa); Valentina Piccini, MD (Empoli); Letizia Pieruzzi, MD (Pisa); Catia Polloni, RN (Grosseto); Gabriella Postiglione, RN (Prato); Benedetta Ragghianti, MD (Firenze); Anna Ranchelli (Arezzo); Nicola Riitano, DPM (Pisa); Loredana Rizzo, MD (Grosseto); Anxhela Rabuchia, DPM (Prato); Chiara Russo, RN (Lucca); Giovanna Sabatini, DPM (Firenze); Elisabetta Salutini, MD (Pistoia); Laura Sambuco, MD (Grosseto); Sara Sandroni, RN (Arezzo); Maheva Sarzanini, DPM (Carrara); Alessia Scatena, MD (Arezzo); Simone Serantoni, MD (Prato); Giovanni Antonio Silverii, MD (Borgo San Lorenzo); Barbara Simi, RN (Grosseto); Massimiliano Telleschi, RN (Empoli); Edoardo Trapani, DPM (Grosseto); Cristiana Valdambrini, RN (Grosseto); Serena Vannacci, RN (Grosseto); Secondina Viti, MD (Pescia).
References
1. Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367-2375. doi:10.1056/NEJMra1615439
2. Armstrong DG, Tan T, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62-75. doi:10.1001/ jama.2023.10578
3. Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. doi:10.1186/s13047-020-00383- 2
4. Gazzetta Ufficiale. [Provisions for the prevention and treatment of diabetes mellitus]. March 16, 1987. Accessed October 4, 2023. https://www.gazzettaufficiale.it/eli/id/1987/03/26/087U0115/sg
5. Gazzetta Ufficiale. [Regulations for the rationalization of the National Health Service, pursuant to Article 1 of Law No. 419 of November 30, 1998]. June 19, 1999. Accessed October 4, 2023. https://www.gazzettaufficiale.it/eli/id/1999/07/16/099G0301/sg
6. Italian Society of Diabetology. https://www.siditalia.it. Accessed October 4, 2023.
7. Regione Toscana. [Official Bulletin of the Tuscany Region, Regional Executive Decree No. 1304 of December 9, 2003: Organizational Guidelines for the Management of Diabetic Foot]. Accessed October 4, 2023. https://trasparenza.consiglio.regione.toscana.it/node/49647
8. Regione Toscana. [Official Bulletin of the Tuscany Region, Regional Decree No. 698 of July 19, 2016: Diagnostic-Therapeutic-Care Pathway for Persons Affected by Diabetic Foot: Regional Guidelines]. https://trasparenza.consiglio.regione.toscana.it/node/38362. Accessed October 4, 2023.
9. Piaggesi A, Ferraresi R, Gargiulo M. The elephant in the room. Int J Low Extrem Wounds. 2023:15347346231191229. doi:10.1177/15347346231191229
10. Nuti S, Bini B, Ruggieri TG, Piaggesi A, Ricci L. Bridging the gap between theory and practice in integrated care: the case of the Diabetic Foot Pathway in Tuscany. Int J Integr Care. 2016;16(2):9. doi:10.5334/ijic.1991
11. Piaggesi A, Coppelli A, Goretti C, Iacopi E, Mattaliano C. Do you want to organize a multidisciplinary diabetic foot clinic? We can help. Int J Low Extrem Wounds. 2014;13(4):363-370. doi:10.1177/1534734614545876
12. Iacopi E, Pieruzzi L, Goretti C, Piaggesi A. I fear COVID but diabetic foot (DF) is worse: a survey on patients’ perception of a telemedicine service for DF during lockdown. Acta Diabetol. 2021;58(5):587-593. doi:10.1007/s00592-020-01653-y
13. Istituto Superiore di Sanità. EpiCentro - Epidemiology for public health. 2020 National Outcomes Programme. https://www.epicentro.iss.it/politiche_sanitarie/pne-2020. Accessed October 4, 2023.
14. PNRR in Tuscany. Mission 6 - Local Healthcare, Healthcare Service Innovation. https://pnrr.toscana.it/-/missione-6-sanita-territoriale-innovazione-del-servizio-sanitario. Accessed February 10, 2023.
15. Commission Directive 2005/28/EC of 8 April 2005. Laying down principles and detailed guidelines for good clinical practice as regards investigational medicinal products for human use, as well as the requirements for authorisation of the manufacturing or importation of such products. European Community, Brussels, 2005.
16. Council of Europe. Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine, (Oviedo Convention), European Treaty Series No 164, Strasbourg, 1997.