Drug-Eluting Technologies in Peripheral Arterial Disease With a Focus on Chronic Limb-Threatening Ischemia
Abstract
Drug-coated technologies target the delivery of therapeutics directly to specific vascular segments with or without relying on a permanent scaffold. Paclitaxel remains the predominantly utilized antirestenotic medication in peripheral arterial treatment. This review provides a detailed discussion of research evaluating paclitaxel and alternative drug-coated therapies within the context of contemporary treatment of chronic limb-threatening ischemia.
J CRIT LIMB ISCHEM 2026:6(2):E36-E45. doi: 10.25270/jcli/CLIG-2500009
Key words: drug-coated technologies, drug-eluting technologies, paclitaxel, peripheral arterial disease, chronic limb-threatening ischemia
Introduction
Local drug delivery to prevent restenosis has long been a focus of technological advancement in the management of peripheral arterial disease (PAD) and has become one of the most widely studied topics of the last 2 decades. Paclitaxel, initially used in coronary drug-eluting stents (DES), has become the primary antirestenotic medication in peripheral arterial treatment. In this review, we seek to re-examine prior research efforts with paclitaxel and alternative drug-coated therapies in the context of modern treatment of chronic limb-threatening ischemia (CLTI).
Paclitaxel is an extract from the bark of Pacific yew trees and exhibits potent cytotoxic inhibition of cellular proliferation by disrupting cellular microtubule organization (Figure).1 The first U.S. Food and Drug Administration (FDA)-approved coronary DES utilized sirolimus (Cypher, Cordis) and paclitaxel (Taxus, Boston Scientific), respectively, and were heralded for their significant reduction of in-stent restenosis (ISR) compared with bare-metal stenting (BMS).2,3
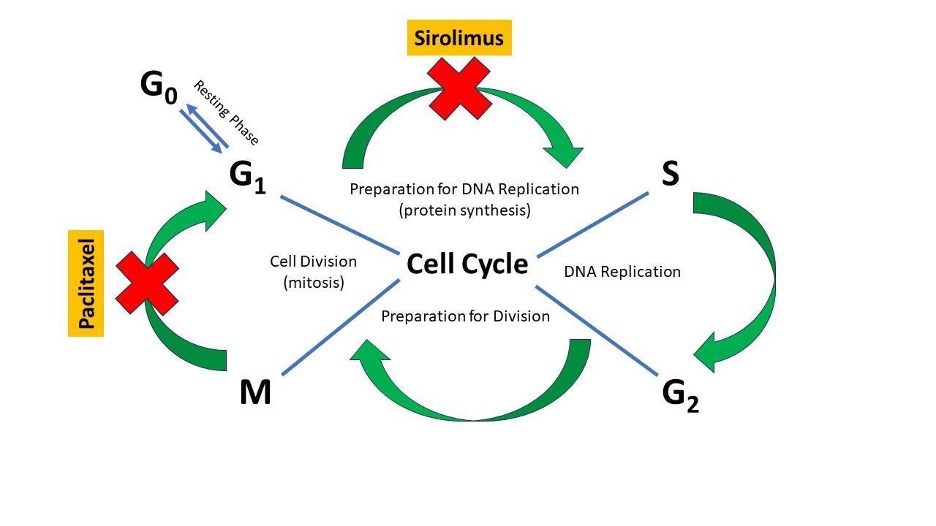
Sirolimus (or rapamycin), another natural compound, was derived in 1972 from a fungus found on Rapa Nui (Easter Island). Originally targeted as an antifungal agent, sirolimus was shown to exhibit cytostatic effects through receptor inhibition of the mammalian target of rapamycin, resulting in the cessation of cell-cycle progression in the late G1 to S phase (Figure).4 Soon after its approval for use in coronary DES, sirolimus-eluting self-expanding stents (S.M.A.R.T., Cordis) for superficial femoral artery disease were evaluated utilizing dose equivalents from those studied in the coronary arteries. Unfortunately, this stent failed to achieve a statistically significant reduction in restenosis compared with BMS.5 This paved the way for translational research, transitioning paclitaxel from drug-eluting coronary stents to wide applications in PAD.
Drug-Coated Balloon Studies in Peripheral Arterial Disease
Historically, percutaneous transluminal angioplasty (PTA) has been the de facto treatment modality for both above-the-knee (ATK) and below-the-knee (BTK) endovascular interventions for PAD. Unfortunately, vessel patency rates as low as 33% at 1 year have been described in the femoropopliteal region with PTA alone.6 Similar or worse outcomes have been described in the tibial arteries after PTA, with short-term patency rates ranging from 13% to 48% in the initial studies.7,8 More contemporary studies have shown similarly low angiographic patency at 3 months in patients with CLTI and long lesions (31% patency, lesion length ≥80 mm).9
Drug-coated balloon (DCB) technology is intended to provide durable treatment results while foregoing the implantation of a permanent scaffold. Currently, several FDA-approved DCBs are available, with data supporting their use in both de novo and ISR lesions. Notably, while all the FDA-approved DCBs primarily use the same chemotherapeutic medications delivered to the vessel, they do so via alternate carrier molecules/mechanisms as well as different drug concentrations; therefore, a class effect should not be assumed.
Drug-coated balloon use in the femoropopliteal arteries
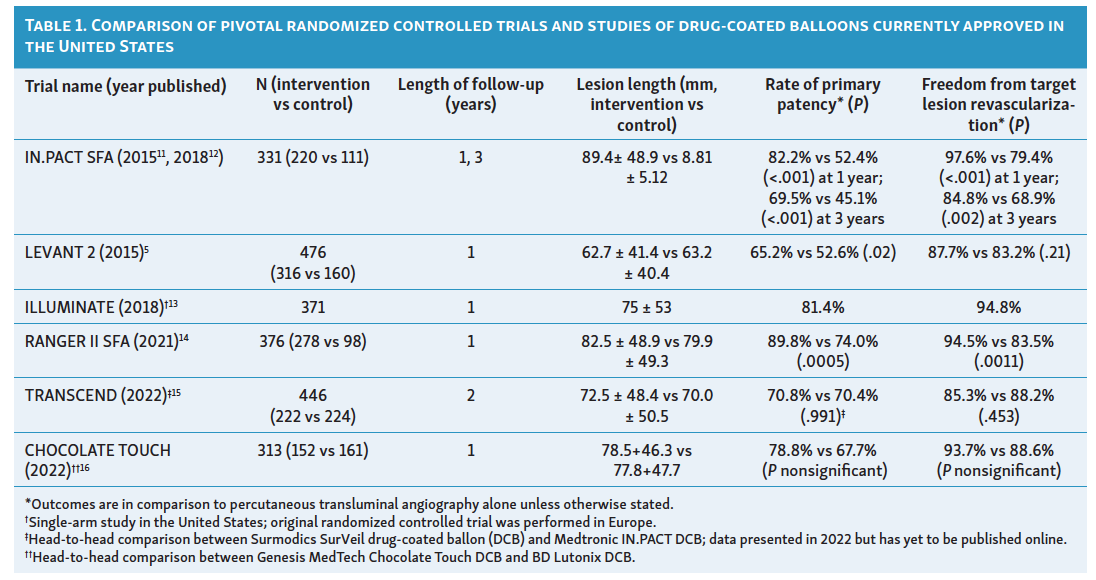
To date, multiple trials have shown the advantage of DCBs over uncoated balloon angioplasty for the treatment of femoropopliteal lesions (Table 1).10 The initial studies comparing DCB use to PTA alone showed favorable primary patency rates at 1 year with a noninferior safety profile.17 Longer-term data (extending to 2-3 years) comes primarily from the IN.PACT device (Medtronic). While still statistically significant, IN.PACT showed lower patency rates compared to PTA over time, compared with the initially published 1-year data (69.5% vs 45.1%, P <.001, for primary patency of DCB compared to PTA at 36 months, compared with 82.2% vs 52.4% primary patency, P <.001, at 12 months).18,19
In the femoropopliteal segment, randomized data from the EffPac program with the Luminor paclitaxel nano-coated DCB (iVascular) demonstrated superior short- and mid-term efficacy vs plain old balloon angioplasty, with higher 12-month primary patency (90.3% vs 65.3%). Luminor DCB had a sustained benefit at 2 years (primary patency 90.2% vs 62.7%; freedom from target lesion revascularization [TLR] 97.2% vs 78%) without an apparent safety signal. By 5 years, the treatment effect had attenuated, although primary patency remained statistically higher (61.4% vs 53.5%) and freedom from clinically driven TLR was numerically higher with DCB (82.1% vs 73.7%), with similar all-cause mortality between groups. Long-term effectiveness appears procedure- and lesion-dependent, with residual stenosis >30% identified as a key determinant of DCB failure.20-24
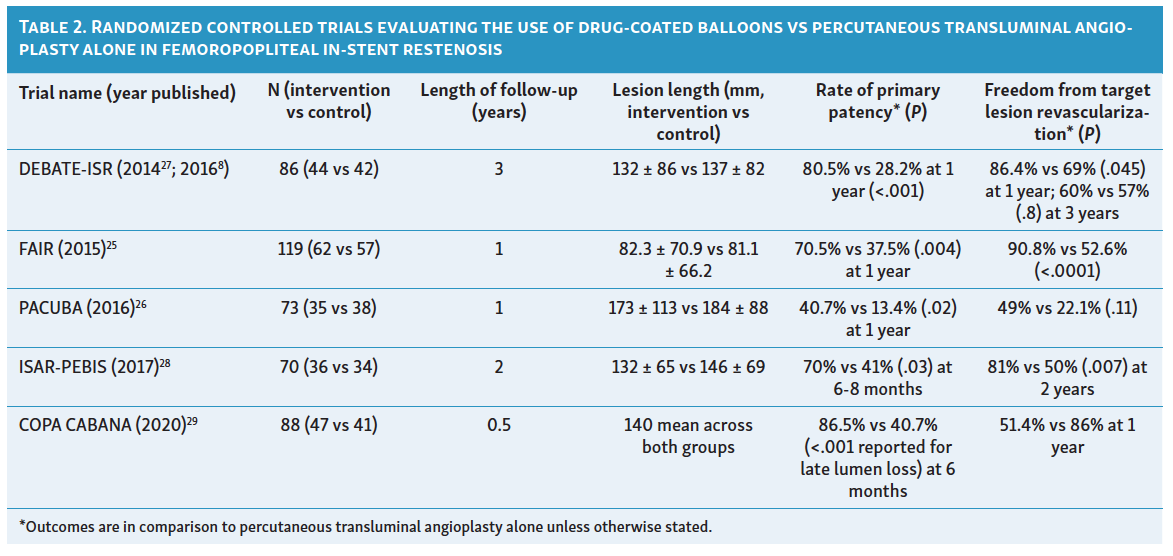
The use of DCBs for femoropopliteal disease extends beyond the treatment of de novo lesions. DCBs are currently 1 of only 3 FDA-approved interventions for femoropopliteal ISR, in addition to laser atherectomy and the Viabahn covered stent (Gore). Initial registry data utilizing the IN.PACT DCB showed promising primary patency rates for femoropopliteal ISR at 12 months as well as high levels of procedural success and safety.25,26 Subsequent randomized controlled trials (RCTs) have confirmed markedly lower rates of recurrent restenosis with DCB than with PTA alone (Table 2). Unfortunately, both rates of restenosis and TLR increase with longer-term follow-up. For example, the Drug-Eluting Balloon in Peripheral Intervention for In-Stent Restenosis (DEBATE-ISR) trial, which had promising 1-year data, demonstrated no difference in TLR at 3 years (40% vs 43% for DCB vs PTA, respectively). Furthermore, shorter lesions tended to do better than longer lesions with regard to rates of recurrent restenosis.28 Collectively, registry data and the available RCTs demonstrate DCB use for femoropopliteal ISR is associated with superior efficacy outcomes compared to PTA alone at 1-year follow-up.
Drug-coated balloon use in patients with chronic limb-threatening ischemia
The major trials in the femoropopliteal segments did not include significant numbers of patients with CLTI; for example, the IN.PACT SFA, EffPac, and ILLUMINATE pivotal trials had less than 5% of subjects enrolled with Rutherford 4-5 disease.20,21 Conversely, nearly 10% of patients enrolled in the LEVANT-2 RCT of the Lutonix balloon (BD) had CLTI. DCB use resulted in improved primary patency when compared with angioplasty alone (65.2% vs 52.6%, P=.02).
Drug-coated balloon use in the infrapopliteal arteries
Given the success of DCBs in the femoropopliteal region, comparable results in the infrapopliteal arteries for patients with CLTI were highly anticipated. Unfortunately, the data did not corroborate this assumption. The first infrapopliteal trial involving DCBs was with the IN.PACT DCB, which did not show an improvement of DCB over PTA alone in the infrapopliteal arteries in regard to either TLR (9.2% vs 13.1%, P=.291 for DCB vs PTA, respectively) or late lumen loss (0.61 + 0.78mm vs 0.62 + 0.78mm, P=.950 for DCB vs PTA, respectively).29 More concerning was a non-statistically significant safety signal for increased rates of major amputations through 12 months seen in the DCB vs PTA alone arm. The follow-up trial presenting 5-year data similarly showed no superiority of DCB compared with PTA. There was no significant difference in safety signals between groups at this time point, including risk of amputation in this longer-term data.30
The Lutonix BTK randomized trial demonstrated noninferior short-term safety at 30 days (short-term safety endpoint: freedom from major adverse limb events [MALE] and perioperative death [POD] 99.3% with DCB vs 99.4% with PTA; noninferiority P<.001). For short-term efficacy, the pre-specified 6-month composite endpoint (freedom from vessel occlusion, clinically driven TLR, and above-ankle amputation) showed benefit that was most evident in the proximal-segment cohort (proximal segment defined as the proximal two-thirds of the BTK artery: 76% DCB vs 62.9% PTA; one-sided P<.01), whereas the overall intent-to-treat analysis did not meet the pre-specified statistical success criterion despite numerically favorable results (74.5% vs 63.5%; one-sided P=.02). Secondary endpoints (including primary patency and clinically driven TLR) also favored DCB at 6 months. However, these early advantages were not maintained at longer-term follow-up (12 months), contributing to the overall conclusion of limited durable efficacy for infrapopliteal DCB in this setting.31
Contradicting the above negative results was the AcoArt-BTK trial of the Litos DCB (Boston Scientific), which showed markedly superior reduction in late lumen loss on routine follow-up angiography at 6 months (0.51 ± 0.60 mm in the DCB group vs 1.31 ± 0.72 mm in the angioplasty arm). These results carried forward for a pivotal randomized trial of 120 patients with CLTI randomized to DCB vs angioplasty (primary patency with DCB 75.0% vs 28.3%, P<.001).32 This was followed by the AcoArt II-BTK trial, which was a prospective, multicenter, randomized, single-blinded study of 120 patients with CLTI undergoing infrapopliteal (BTK) revascularization, comparing the Litos Tulip DCB angioplasty with plain balloon PTA. At 5 years, the DCB group had higher freedom from all-cause death (74.6% vs 57.2%; P=.04) and a lower composite major adverse event rate (34.5% vs 56.1%; P=.013). Freedom from clinically driven TLR was numerically better with DCB angioplasty (70.5% vs 53.7%; P=.058), while major amputation rates were not significantly different (5.2% vs 1.8%; P=.347).
Overall, the findings of the two AcoArt studies support favorable long-term outcomes with DCB angioplasty compared with plain balloon PTA in the BTK segments.33 Furthermore, a meta-analysis of DCB in the infrapopliteal segment found overall benefit in TLR and complete wound healing compared to angioplasty alone.34
The absence of consistently positive data surrounding DCBs in the infrapopliteal arteries may be attributed to factors such as composition of the plaque (eg, higher thrombus burden compared to femoropopliteal arteries), early elastic recoil, insufficient uptake of the chemotherapeutic drug into the vessel wall, or increased distal embolization into wound beds in patients. Supporting the plausibility of a thrombotic component in BTK CLTI, histopathologic assessment of amputation specimens has demonstrated that severe infrapopliteal occlusive disease is frequently associated with luminal thrombi, often in the setting of limited atherosclerosis.35-37
Particulate embolization
Paclitaxel DCBs may underperform in CLTI because clinically meaningful amounts of coating/drug can be lost during delivery, embolizing distally as particulates. In patients with limited tibial runoff and impaired microcirculatory reserve, this downstream particulate burden may contribute to microvascular obstruction, vasospasm, or inflammatory responses, manifesting as slow-flow/no-reflow and potentially reducing healing.38 Limus-based balloons (eg, sirolimus/everolimus) are proposed as an alternative because limus drugs are predominantly cytostatic with anti-inflammatory effects, theoretically lowering the risk of distal tissue injury. Furthermore, contemporary limus balloon platforms often use carrier or microreservoir technologies to improve arterial wall uptake and prolong tissue residence while minimizing coating loss—features that could translate into less distal embolization-related microvascular compromise in CLTI, although definitive comparative clinical evidence in CLTI needs further study.39,40
Removable scaffolds coupled with drug-coated balloons
In a novel approach to BTK treatment with DCB, the DEEPER OUS study described the use of a removable self-expanding Spur stent with external penetrating spikes (Reflow Medical) followed by a DCB, which demonstrated a primary patency of 85.7% (95% confidence interval [CI]: 78.2-93.2%; P<.001 vs 51% performance goal).41 More recently, the DEEPER LIMUS trial extended this concept by combining a retrievable scaffold with a sirolimus-coated balloon in Rutherford class 3-5 infrapopliteal disease (88% Rutherford 5; 36% occlusions; 54% TASC B/C), reporting a 6-month MALE-POD composite safety event rate of 11.5% and a 12-month primary patency of 89.5%, with no additional major amputations or clinically driven TLR reported through 12 months.42 Although limited by a small sample size and a single-arm design, these early studies support the feasibility of scaffold-assisted vessel preparation followed by limus-coated balloon angioplasty as a strategy to mitigate recoil and optimize drug delivery in BTK interventions.
Drug-eluting stents for the above-the-knee (femoropopliteal) segment
The first successful treatment in the femoropopliteal arterial segment with a dedicated DES was the Zilver PTX (Cook Medical). Zilver PTX applies a relatively high dose (3 µg/mm²) of paclitaxel directly to a nitinol self-expandable stent without a polymer. The Zilver PTX demonstrated sustained clinical benefits at a 5-year follow-up in an RCT compared with standard care (balloon angioplasty or BMS). Five-year primary patency was significantly higher in the DES cohort (83.1% vs 67.6%, P<.01).43
Multiple important subsequent reports have been published regarding the Zilver PTX. In the ZILVERPASS study, a randomized trial comparing Zilver PTX with bypass surgery using prosthesis graft, non-inferiority was shown in the rate of 12-month primary patency (74.5% vs 72.5%, P=.998). This result suggested that Zilver PTX can serve as an alternative to bypass surgery with prosthesis graft in complex lesions.44 Several single-arm trials in real-world complex lesions have also been conducted; however, heterogeneous patency rates (60% to 85%) were observed.45-47 This suggests that procedural quality may influence the outcome of Zilver PTX in addition to patient and lesion characteristics.
The ZEPHYR study of the Zilver PTX stent helped identify the predictors of restenosis with DES: 1) lesion length >16 cm, 2) distal external elastic membrane area ≤27 mm², and 3) minimum stent area (MSA) ≤12 mm².45 Following the ZEPHYR study, the concept of “lesion preparation” became more recognized given the ISR associated with a smaller residual MSA. Although Zilver PTX marked a significant progress, the patency rate of Zilver PTX still did not match that of coronary DES. Therefore, a new generation of peripheral DES with a novel concept emerged.
Eluvia (Boston Scientific) is a second-generation femoropopliteal-dedicated DES that uses a biocompatible fluoropolymer developed from coronary DES technology. It applies a low dose of paclitaxel (0.167 µg/mm²) using fluoropolymer to the surface of the Innova nitinol self-expandable stent (Boston Scientific). In the MAJESTIC trial, a 12-month primary patency of 96.4% was reported.48
Due to the promising results of the MAJESTIC trial, early market introduction was anticipated. The IMPERIAL trial, conducted as an FDA approval study, was an RCT comparing Eluvia with Zilver PTX. While designed to demonstrate non-inferiority, initial 12-month results reported superior primary patency (88.5% vs 79.5%, P=.0119) in the Eluvia cohort,49 though this superiority disappeared during the 24-month follow-up (83.0% vs 77.1%, P=.10).50 These extended results were confirmed by the REALDES 3-year outcomes, which again showed no difference between Eluvia and Zilver PTX in the treatment of symptomatic femoropopliteal disease (3-year patency: 65.2% Eluvia and 70% Zilver PTX, P=.74).51
The 1-year superiority of Eluvia may be explained by its durable fluoropolymer coating, creating a controlled, sustained elution profile designed to target prolonged drug availability out to approximately 12 months. In contrast, Zilver PTX is polymer-free (paclitaxel applied without a binder), which leads to much earlier drug wash-off. Preclinical pharmacokinetic data show that about 95% of paclitaxel is delivered from the stent within 24 hours, with tissue levels persisting for weeks but with far less prolonged release than polymer-based systems.52 At greater than 1-year follow-up, after elution is complete, Zilver PTX and Eluvia stents may perform similarly to BMS, resulting in comparable outcomes.
When evaluating the DES literature, it is also important to distinguish how loss of patency occurs (restenosis vs complete stent occlusion) because occlusions may present more abruptly, be more difficult to treat, and carry a greater risk of limb-threatening ischemia than nonocclusive restenosis. Thus, the finding of greater occlusive failures with Eluvia despite similar patency rates suggests that patency alone may obscure clinically meaningful differences in failure mode and supports reporting occlusions as a separate endpoint alongside patency and TLR.53
Halo sign
One concern following Eluvia stent implantation is the reported aneurysmal degeneration known as the “halo sign”. Initially reported in the CAPSICUM study, the halo sign was seen in association with subintimal guidewire passage with subsequent Eluvia placement.54 Data from multiple studies have shown no significant safety signal associated with the halo sign.53 A pooled analysis of the IMPERIAL and EMINENT studies showed no significant association between the presence of the halo sign and primary patency in 659 patients.55 A 5-year follow-up study confirmed higher patency rates with a halo sign compared to without (87% vs 59%; hazard ratio [HR] 2.48, 95% CI 1.19-5.16; P=.015), although confirmation in larger cohorts is warranted given study design limitations.53
Drug-Eluting Stents in Below-the-Knee Lesions
Given the overall lack of efficacy of drug-coated technology BTK, standard percutaneous angioplasty has become the default treatment. In cases of severe recoil or dissection requiring bailout, placement of coronary-specific DES has become the most utilized strategy. Several trials have supported this technique, including the Achilles trial, which randomized 200 patients to DES with a sirolimus-eluting stent vs PTA. At 1 year, the rate of restenosis was markedly reduced in the coronary DES arm vs PTA (22.4% vs 41.9%; P=.019).56 These results were bolstered by the YUKON and DESTINY RCTs, which similarly showed benefit of sirolimus- and everolimus-based DES over BMS.57
Balancing these strongly positive studies were the SAVAL and PADI trials, which showed a lack of benefit of DES in long lesions (SAVAL) and with long-term follow-up (PADI) in patients with BTK CLTI. In SAVAL, the neutral results for the efficacy endpoint occurred in the context of a high 12-month patency rate in the PTA arm (76%), which likely narrowed any incremental benefit achievable with DES.58,59 In the PTA arm, optimal PTA was performed rather than standard of care PTA (as in other contemporary trials such as LIFE-BTK).60 SAVAL and PADI highlight the challenging patient subset that is BTK CLTI.
Bioresorbable Drug-Eluting Stents in Below-the-Knee Arterial Disease
BTK lesions remain challenging, given increased lesion complexity and worse patient-level comorbidities (ie, diabetes and end-stage renal disease), resulting in poor post-intervention patency. Patency of BTK disease is constrained by 4 main factors: elastic recoil of the target vessel, flow-limiting dissection, restenosis due to neointimal hyperplasia, and impaired inflow or outflow. The clinical need for improved outcomes with an ideal device that can combat recoil, deliver antiproliferative drugs, and treat significant dissections, while “leaving nothing behind”, has led to the rapid development of drug-eluting bioresorbable scaffolds (DRS).
Composition of bioresorbable stents
Several DRS platforms are under study to evaluate optimal biocompatibility and degradation profile. Components of DRS for BTK interventions include scaffolds and the drug. The scaffolds may be made of polymers, usually poly-L-lactic acid, and corrodible metals such as magnesium and iron.
DRS also utilizes antiproliferative drugs, paclitaxel or rapamycin derivatives, to inhibit neointimal hyperplasia. Drug elution occurs by hydrolysis of the polymer matrix coating the scaffold backbone, followed by scaffold dissolution over several years.
Clinical studies
Bosiers et al published the first large clinical study of BRS in BTK interventions in 2005, examining an absorbable metal stent. This initial investigation showed 1-year primary patency, limb salvage, and survival rates of 73.3%, 94.7%, and 85%. The follow-up AMS INSIGHT trial, which compared the absorbable metal stent to PTA alone, showed no difference in 30-day safety endpoints and had worse 6-month patency compared to PTA alone.61
Next, Varcoe et al showed encouraging outcomes in patients with BTK disease with the ABSORB scaffold. The study reported 12-month survival of 84.8%, freedom from clinically driven TLR of 96%, and a primary patency rate of 96% at 12 months. The 5-year follow-up results of this trial continued to demonstrate favorable outcomes over PTA alone.62,63
The LIFE-BTK trial was an RCT studying the Esprit BTK DRS (Abbott) compared to PTA alone in Rutherford 4-5 BTK disease. At 12 months, 74% of patients in the scaffold group achieved the composite primary endpoint, compared with 44% in the PTA group (absolute difference 30%; 95% CI, 15%-46%; P<.001). Importantly, these benefits appeared durable at 2 years, with higher freedom from the revised composite efficacy endpoint in the DRS group vs PTA (68.8% vs 45.4%; P=.0004), driven in part by lower binary restenosis (28.5% vs 48.2%; P=.005) and lower clinically driven TLR (9.7% vs 18.6%; P=.034), while maintaining a comparable safety profile (freedom from MALE-POD 91.6% vs 95.6%; P=.16). Given the strength of these clinical trial results, the ESPRIT study potentially represents a major shift in the endovascular management of CLTI.60,64
The MOTIV BVS BTK pilot study was a single-arm, multicenter trial evaluating 76 scaffolds in 60 limbs over 36 months. The 6-month data demonstrated 99% technical success, 90% primary patency, and a 3% clinically driven TLR.65 The 3-year follow-up was recently reported, with a primary patency of 80%.66
RESOLV I was a prospective, single-arm, multicenter trial examining the Magnitude DRS bioresorbable scaffold (R3 Vascular) in infrapopliteal interventions. The study enrolled 50 patients with Rutherford category 3-5 disease. Six-month data showed 100% (n = 28/28) achievement of primary safety endpoints, defined as freedom from MALE and POD. Primary efficacy endpoints, including angiographic primary patency and freedom from TLR, were met in 93% (n = 27/29) of lesions at 6 months.67
Bioresorbable stents for BTK PAD represent an important breakthrough, providing a treatment that addresses both the need for immediate scaffolding and the need for long-term vessel health.
Liquid Drug Delivery
Various types of liquid drugs have been employed to prevent and treat restenosis-encompassing antiproliferative, anticoagulant, and anti-inflammatory agents. In the 1960s, heparin was initially utilized for thrombosis treatment using polyvinyl alcohol applied to the adventitia.68 Over subsequent decades, heparin became widely adopted as an anticoagulant to inhibit excessive platelet and smooth muscle cell aggregation, which contributes to vessel narrowing following endothelial injury.69 Historically, local drug delivery systems aimed at targeted heparin delivery have included polyvinyl alcohol, other polymer sheets, and various catheters such as the InfusaSleeve (LocalMed).70 However, the use of heparin declined over time, partly due to the high dosages required for effective therapy, which occasionally led to bleeding complications.
Although significant progress was achieved in the late 1990s and early 2000s in enhancing liquid drug delivery systems, the development and success of DES in treating lower extremity restenosis diverted almost all attention away from liquid delivery devices. Consequently, exploration of catheters such as the InfusaSleeve, Infiltrator (InterVentional Technologies), and iontophoretic catheters for treating local lesions in the peripheral vasculature nearly ceased.71,72 However, recent advances in liquid delivery systems have led to marked improvements in outcomes for endovascular treatment of infrainguinal lesions, including challenging femoropopliteal and infrapopliteal lesions.73 Current examples of liquid drug delivery systems in use include 1) the Bullfrog micro-infusion device (Mercator MedSystems), 2) the ClearWay rapid-exchange therapeutic infusion catheter (Atrium Medical), and 3) the Occlusion Perfusion Catheter (OPC) (Advanced Catheter Therapies).
The Bullfrog was created to inject therapeutic drugs directly into the adventitia, either through blood vessel walls or perivascular areas. When the balloon is sealed, the microneedle on its surface remains flat, ensuring safe passage through vessels to the target lesion. Upon low-pressure inflation (2 atm) at the target site, the microneedle penetrates the vessel wall without causing damage, allowing the selected therapeutic agent to be injected into the adventitial tissue. Several clinical studies have highlighted the potential for this liquid drug delivery device, including the Temsirolimus Adventitial Delivery to Improve Angiographic Outcomes Below the Knee (TANGO) trial, which evaluated local drug delivery following revascularization of lesions in patients presenting with CLTI.74-76 The TANGO-3 BTK randomized trial is ongoing and will evaluate delivery of temsirolimus BTK after revascularization in patients with CLTI compared to placebo infusion.
The ClearWay catheter is designed to deliver therapeutic drugs directly to target lesions in both coronary and peripheral vasculature. Drug infusion occurs through micropores in the polytetrafluoroethylene balloon, which temporarily occludes blood flow for precise drug delivery to the target site. The ClearWay catheter has been successfully used to administer liquid paclitaxel, glycoprotein IIb/IIIa inhibitors, thrombolysis agents, and urokinase.77,78
The OPC is an advanced drug-delivery device equipped with a built-in fiberoptic pressure sensor for precise targeting. It features 2 occlusion balloons that, when inflated, create a controlled “treatment chamber”. This chamber allows continuous monitoring of applied pressure and precise control over the volume of therapeutic agent administered. Clinical studies have demonstrated the effectiveness of the OPC, achieving a 96.4% rate of clinically driven TLR at 6 months.79,80
Role of Plaque Modification and Atherectomy to Enhance Drug Delivery
Atherectomy and plaque modification are important tools that may enhance vessel compliance promoting DCB expansion and may enhance wall porosity allowing for deeper penetration of antiproliferative agents. The use of DES and DCB for intra-arterial drug delivery faces the challenge of transferring drugs across calcified atherosclerotic plaques, resulting in reduced therapeutic concentration in the desired treatment area. Paclitaxel is highly hydrophobic and requires significant vascular penetration to be efficiently absorbed by surrounding tissues, gain cellular entry, and bind tightly to proteins within cells and the interstitium.75
Optimization of drug delivery through bigger balloon expansion, which may be promoted by atherectomy or plaque modification, has also been established. In an ex vivo study, scanning electron microscopy images demonstrated that the drug was mostly retained within grooves and gaps of the luminal surface of the arteries treated with the DCB-artery-ratio of 1.25:1, as compared to 1:1. The overexpansion of the artery allowed deeper penetration of the drug coating within the intimal layer, strengthening its adhesion to the luminal surface.81 Furthermore, plaque modification with arthrectomy, specialty balloons, intravascular lithotripsy, and temporary stents can enhance deep cracking of the plaque and, theoretically, improve drug delivery to deeper layers, promoting retention of the antiproliferative agent within the treated areas.
Current clinical data: atherectomy plus drug-coated balloons
Although the potential therapeutic benefit of using atherectomy with DCB is clear, clinical data has been conflicting. In 2 randomized trials, use of atherectomy was safe and effective with higher technical success rates, decreasing dissection, and overall bailout stenting. In the DEFINITIVE AR study, atherectomy plus DCB was not associated with a significant improvement in the 1-year primary outcome of percent diameter stenosis, clinically driven TLR, and freedom from major adverse events; however, the trial underscored the importance of achieving an optimal acute angiographic result, particularly residual stenosis <30% (ie, technical success). When technical success was achieved, 12-month patency was 94.1% vs 68.8% when technical success was not achieved.82,83 Cai et al revealed similar outcomes with no difference in amputation rates, 12-month and 24-month primary patency, and overall mortality rate.84 A meta-analysis, including 2 RCTs and 4 retrospective cohort studies, comparing atherectomy plus DCB vs DCB alone in the treatment of femoropopliteal lesions showed no significant difference between the 2 groups at 12 months in terms of distal embolization, perforation, hematoma, primary patency, TLR, leg amputations and mortality (relative risk for mortality: 2.18, 95% CI: 0.71-6.64, P=.17).85 Finally, Rodoplu et al retrospectively evaluated atherectomy plus DCB vs DCB alone and showed that combined usage of rotational atherectomy plus DCB for the treatment of CLTI resulted in reduced 1-year TLR (6.1% vs 17.4%, P=.001).86 Larger RCTs with longer-term follow-up are required to determine the benefits of atherectomy as an adjunctive therapy with drug-coated devices.
Katsanos Controversy
In 2018, Katsanos et al published a meta-analysis purporting to show increased mortality associated with paclitaxel-coated balloons (PCBs) in peripheral arterial angioplasty. The study included 28 RCTs with 4663 patients randomized to PCB vs PTA alone. At 1 year, the safety signals were similar; however, at 2 years, the mortality rate in the PCB arm was significantly higher than the PTA arm (7.2% vs 3.8%, relative risk 1.68; 95% CI 1.15-2.47), with a reported number needed to harm of 29 patients. The manuscript also postulated a potential dose-time relationship but failed to provide a clear causal mechanism for the results.12 The concerns surrounding DCB were bolstered by a second meta-analysis87 examining PCB use specifically in the infrapopliteal arteries for treatment of CLTI. The study-level meta-analysis showed that amputation-free survival was significantly worse with PCB use (13.7% vs 9.4%, P=.008). Particulate embolization was raised as a mechanism for the higher adverse event rate with PCB. These publications led to negative publicity and an FDA warning letter regarding the use of PCBs. The Katsanos controversy led to a significant shift in practice, with an approximate 50% reduction in the use of PCBs for PAD in the United States over the 6 months after the FDA warning.
The Katsanos meta-analysis results were challenged by several manuscripts.5 Most importantly, a large-scale meta-analysis was conducted in which much of the missing data and loss to follow-up from the initial Katsanos paper were rectified and showed no perceived mortality signal with PCBs: intent-to-treat analysis (HR 1.14, 95% CI 0.93-1.40); as-treated analysis (HR 1.13, 95% CI 0.92-1.39).88 This data led the FDA to withdraw its warning about the use of PCBs in 2023.
Conclusion
Drug-coated technologies enable the proceduralist to deliver therapeutic agents directly to specific arterial segments via multiple mechanisms. Drug technologies, with or without a scaffold, in the peripheral arteries will remain a key area of focus as we work to improve patency and optimize outcomes for our patients with PAD.
Affiliations and Disclosures
Matthew T. Finn, MD, MSc, McCall Walker, MD, Craig Walker, MD, and Pradeep Nair, MD, are from the Cardiovascular Institute of the South, Gray, Louisiana, USA; Saami K. Yazdani, PhD, is from the Department of Engineering, Wake Forest University, Winston-Salem, North Carolina, USA; Tatsuya Nakama, MD, is from the Department of Cardiology, Tokyo Bay Medical Center, Urayasu, Japan; Mahmoud Abdelghany, MD, is from the Department of Cardiology, Mediclinic City Hospital, Mohammed Bin Rashid University of Medicine and Health Sciences, Dubai, UAE; Sonal Pruthi, MD, Robert Zilinyi, MD, Daniel Snyder, MD, and Sahil A. Parikh, MD, FACC, FSCAI, are from the Department of Cardiology, Columbia University Irving Medical Center/NewYork-Presbyterian Hospital, New York, New York, USA; and Zola N'Dandu, MD, is from the Department of Cardiology, Ascension Sacred Heart, Pensacola, Florida, USA.
Acknowledgement: Thank you to Chelsea L. Finn, BSN, RN for assistance with editing this manuscript.
Dr Finn reports co-primary investigator responsibilities for trials associated with Avantec Vascular and Mercantor MedSystems. He is on the clinical event committee for a trial sponsored by R3 Vascular, and his spouse has stock in Johnson & Johnson. Dr Finn holds stock in Fastwave Medical and Peytant Solutions, and is a speaker for Nipro, Pfizer, Angiodynamics, Cardiva, and Philips.
The other authors report no financial relationships or conflicts of interest regarding the content herein.
Manuscript accepted March 30, 2026.
Address for correspondence: Matthew T. Finn, MD, MSc, Cardiovascular Institute of the South, 191 Innovation Court, Suite A, Gray, LA 70359. Email: Matthew.Finn@cardio.com
References
1. Horwitz SB. Taxol (paclitaxel): mechanisms of action. Ann Oncol. 1994;5 Suppl 6:S3-S6.
2. Moses JW, Leon MB, Popma JJ, et al; SIRIUS Investigators. Sirolimus-eluting stents versus standard stents in patients with stenosis in a native coronary artery. N Engl J Med. 2003;349(14):1315-1323. doi:10.1056/NEJMoa035071
3. Stone GW, Ellis SG, Cox DA, et al; TAXUS-IV Investigators. One-year clinical results with the slow-release, polymer-based, paclitaxel-eluting TAXUS stent: the TAXUS-IV trial. Circulation. 2004;109(16):1942-1947. doi:10.1161/01.CIR.0000127110.49192.72
4. Seghal SN, Baker H, Vézina C. Rapamycin (AY-22, 989), a new antifungal antibiotic. II. Fermentation, isolation and characterization. J Antibiot (Tokyo). 1975;28(10):727-732. doi:10.7164/antibiotics.28.727
5. Duda SH, Bosiers M, Lammer J, et al. Drug-eluting and bare nitinol stents for the treatment of atherosclerotic lesions in the superficial femoral artery: long-term results from the SIROCCO trial. J Endovasc Ther. 2006;13(6):701-710. doi:10.1583/05-1704.1
6. Rocha-Singh KJ, Jaff MR, Crabtree TR, Bloch DA; VIVA Physicians, Inc. Performance goals and endpoint assessments for clinical trials of femoropopliteal bare nitinol stents in patients with symptomatic peripheral arterial disease. Catheter Cardiovasc Interv. 2007;69(6):910-919. doi:10.1002/ccd.21104
7. Söder HK, Manninen HI, Jaakkola P, et al. Prospective trial of infrapopliteal artery balloon angioplasty for critical limb ischemia: angiographic and clinical results. J Vasc Interv Radiol. 2000;11(8):1021-1031. doi:10.1016/s1051-0443(07)61332-3
8. Parsons RE, Suggs WD, Lee JJ, Sanchez LA, Lyon RT, Veith FJ. Percutaneous transluminal angioplasty for the treatment of limb threatening ischemia: do the results justify an attempt before bypass grafting? J Vasc Surg. 1998;28(6):1066-1071. doi:10.1016/s0741-5214(98)70033-3
9. Schmidt A, Ulrich M, Winkler B, et al. Angiographic patency and clinical outcome after balloon-angioplasty for extensive infrapopliteal arterial disease. Catheter Cardiovasc Interv. 2010;76(7):1047-1054. doi:10.1002/ccd.22658
10. Kondapalli A, Danek BA, Khalili H, Jeon-Slaughter H, Banerjee S. Drug-coated balloons: current outcomes and future directions. Interv Cardiol Clin. 2017;6(2):217-225. doi:10.1016/j.iccl.2016.12.005
11. Nordanstig J, James S, Andersson M, et al. Mortality with paclitaxel-coated devices in peripheral artery disease. N Engl J Med. 2020;383(26):2538-2546. doi:10.1056/NEJMoa2005206
12. Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Karnabatidis D. Risk of death following application of paclitaxel-coated balloons and stents in the femoropopliteal artery of the leg: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. 2018;7(24):e011245. doi:10.1161/JAHA.118.011245
13. Rosenfield K. Intermediate-term (24-month) results of the TRANSCEND study; 2022.
14. Steiner S, Schmidt A, Zeller T, et al. COMPARE: prospective, randomized, non-inferiority trial of high- vs. low-dose paclitaxel drug-coated balloons for femoropopliteal interventions. Eur Heart J. 2020;41(27):2541-2552. doi:10.1093/eurheartj/ehaa049
15. Falkenberg M, James S, Andersson M, et al; SWEDEPAD trial investigators. Paclitaxel-coated versus uncoated devices for infrainguinal endovascular revascularisation in chronic limb-threatening ischaemia (SWEDEPAD 1): a multicentre, participant-masked, registry-based, randomised controlled trial. Lancet. 2025;406(10508):1103-1114. doi:10.1016/S0140-6736(25)01585-5
16. Nordanstig J, James S, Andersson M, et al; SWEDEPAD trial investigators. Paclitaxel-coated versus uncoated devices for infrainguinal endovascular revascularisation in patients with intermittent claudication (SWEDEPAD 2): a multicentre, participant-masked, registry-based, randomised controlled trial. Lancet. 2025;406(10508):1115-1127. doi:10.1016/S0140-6736(25)01584-3
17. Rosenfield K, Jaff MR, White CJ, et al; LEVANT 2 Investigators. Trial of a paclitaxel-coated balloon for femoropopliteal artery disease. N Engl J Med. 2015;373(2):145-153. doi:10.1056/NEJMoa1406235
18. Schneider PA, Laird JR, Tepe G, et al; IN.PACT SFA Trial Investigators. Treatment effect of drug-coated balloons is durable to 3 years in the femoropopliteal arteries: long-term results of the IN.PACT SFA randomized trial. Circ Cardiovasc Interv. 2018;11(1):e005891. doi:10.1161/CIRCINTERVENTIONS.117.005891
19. Tepe G, Laird J, Schneider P, et al; IN.PACT SFA Trial Investigators. Drug-coated balloon versus standard percutaneous transluminal angioplasty for the treatment of superficial femoral and popliteal peripheral artery disease: 12-month results from the IN.PACT SFA randomized trial. Circulation. 2015;131(5):495-502. doi:10.1161/CIRCULATIONAHA.114.011004
20. Krishnan P, Farhan S, Schneider P, et al. Determinants of drug-coated balloon failure in patients undergoing femoropopliteal arterial intervention. J Am Coll Cardiol. 2022;80(13):1241-1250. doi:10.1016/j.jacc.2022.06.043
21. Shishehbor MH, Scheinert D, Jain A, et al. Comparison of drug-coated balloons vs bare-metal stents in patients with femoropopliteal arterial disease. J Am Coll Cardiol. 2023;81(3):237-249. doi:10.1016/j.jacc.2022.10.016
22. Teichgräber U, Lehmann T, Aschenbach R, et al. Efficacy and safety of a novel paclitaxel-nano-coated balloon for femoropopliteal angioplasty: one-year results of the EffPac trial. EuroIntervention. 2020;15(18):e1633-e1640. doi:10.4244/EIJ-D-19-00292
23. Teichgräber U, Lehmann T, Aschenbach R, et al. Drug-coated balloon angioplasty of femoropopliteal lesions maintained superior efficacy over conventional balloon: 2-year results of the randomized EffPac trial. Radiology. 2020;295(2):478-487. doi:10.1148/radiol.2020191619
24. Teichgräber U, Lehmann T, Ingwersen M, et al. Long-term effectiveness and safety of femoropopliteal drug-coated balloon angioplasty : 5-year results of the randomized controlled EffPac trial. Cardiovasc Intervent Radiol. 2022;45(12):1774-1783. doi:10.1007/s00270-022-03265-1
25. Stabile E, Virga V, Salemme L, et al. Drug-eluting balloon for treatment of superficial femoral artery in-stent restenosis. J Am Coll Cardiol. 2012;60(18):1739-1742. doi:10.1016/j.jacc.2012.07.033
26. Bague N, Julia P, Sauguet A, et al. Femoropopliteal in-stent restenosis repair: midterm outcomes after paclitaxel eluting balloon use (PLAISIR trial). Eur J Vasc Endovasc Surg. 2017;53(1):106-113. doi:10.1016/j.ejvs.2016.10.002
27. Shishehbor MH, Zeller T, Werner M, et al. Randomized trial of Chocolate Touch compared with Lutonix drug-coated balloon in femoropopliteal lesions (Chocolate Touch study). Circulation. 2022;145(22):1645-1654. doi:10.1161/CIRCULATIONAHA.122.059646
28. Grotti S, Liistro F, Angioli P, et al. Paclitaxel-eluting balloon vs standard angioplasty to reduce restenosis in diabetic patients with in-stent restenosis of the superficial femoral and proximal popliteal arteries: three-year results of the DEBATE-ISR study. J Endovasc Ther. 2016;23(1):52-57. doi:10.1177/1526602815614555
29. Zeller T, Baumgartner I, Scheinert D, et al; IN.PACT DEEP Trial Investigators. Drug-eluting balloon versus standard balloon angioplasty for infrapopliteal arterial revascularization in critical limb ischemia: 12-month results from the IN.PACT DEEP randomized trial. J Am Coll Cardiol. 2014;64(15):1568-1576. doi:10.1016/j.jacc.2014.06.1198
30. Zeller T, Micari A, Scheinert D, et al; IN.PACT DEEP Trial Investigators. The IN.PACT DEEP clinical drug-coated balloon trial: 5-year outcomes. JACC Cardiovasc Interv. 2020;13(4):431-443. doi:10.1016/j.jcin.2019.10.059
31. Case BC, Torguson R, Zhang C, Waksman R. Overview of the virtual 2021 FDA’s Circulatory System Devices Advisory Panel on Lutonix 014 Drug-coated percutaneous transluminal angioplasty catheter for below-the-knee lesions in critical limb ischemia. Cardiovasc Revasc Med. 2021;33:55-61. doi:10.1016/j.carrev.2021.06.016
32. Jia X, Zhuang B, Wang F, et al. Drug-coated balloon angioplasty compared with uncoated balloons in the treatment of infrapopliteal artery lesions (AcoArt II-BTK). J Endovasc Ther. 2021;28(2):215-221. doi:10.1177/1526602820969681
33. Sun G, Liu J, Jia X, et al. Long-term outcomes of the AcoArt II-BTK trial: drug-coated balloon angioplasty compared with uncoated balloons for the treatment of infrapopliteal artery lesions. J Endovasc Ther. 202415266028241304303. doi:10.1177/15266028241304303
34. Zeller T. Systematic meta-analysis—a scientific gold standard for all therapies? J Crit Limb Ischem. 2022;2(1):E17-E18.
35. Narula N, Dannenberg AJ, Olin JW, et al. Pathology of peripheral artery disease in patients with critical limb ischemia. J Am Coll Cardiol. 2018;72(18):2152-2163. doi:10.1016/j.jacc.2018.08.002
36. Baumann F, Fust J, Engelberger RP, et al. Early recoil after balloon angioplasty of tibial artery obstructions in patients with critical limb ischemia. J Endovasc Ther. 2014;21(1):44-51. doi:10.1583/13-4486MR.1
37. Fanelli F, Cannavale A, Gazzetti M, et al. Calcium burden assessment and impact on drug-eluting balloons in peripheral arterial disease. Cardiovasc Intervent Radiol. 2014;37(4):898-907. doi:10.1007/s00270-014-0904-3
38. Granada JF, Ferrone M, Melnick G, et al. Downstream paclitaxel released following drug-coated balloon inflation and distal limb wound healing in swine. JACC Basic Transl Sci. 2021;6(5):416-427. doi:10.1016/j.jacbts.2021.01.012
39. Boitet A, Grassin-Delyle S, Louedec L, et al. An experimental study of paclitaxel embolisation during drug coated balloon angioplasty. Eur J Vasc Endovasc Surg. 2019;57(4):578-586. doi:10.1016/j.ejvs.2018.11.019
40. Torii S, Yahagi K, Mori H, et al. Biologic drug effect and particulate embolization of drug-eluting stents versus drug-coated balloons in healthy swine femoropopliteal arteries. J Vasc Interv Radiol. 2018;29(7):1041-1049.e3. doi:10.1016/j.jvir.2018.02.006
41. Lichtenberg MKW, Holden A, Scheinert D, et al. Retrievable scaffold therapy before paclitaxel drug-coated balloon angioplasty in infrapopliteal arteries: one-year outcomes of the DEEPER OUS study. EuroIntervention. 2025;21(16):974-976. doi:10.4244/EIJ-D-24-00996
42. Schweiger L, Gütl K, Rief P, et al. Retrievable scaffold therapy combined with sirolimus-coated balloon angioplasty for infrapopliteal artery disease: final results from the DEEPER LIMUS trial. Cardiovasc Intervent Radiol. 2025;48(3):297-303. doi:10.1007/s00270-025-03987-y
43. Dake MD, Ansel GM, Jaff MR, et al; Zilver PTX Investigators. Durable clinical effectiveness with paclitaxel-eluting stents in the femoropopliteal artery: 5-year results of the Zilver PTX randomized trial. Circulation. 2016;133(15):1472-1483; discussion 1483. doi:10.1161/CIRCULATIONAHA.115.016900
44. Bosiers M, de Donato G, Torsello G, et al. ZILVERPASS study: ZILVER PTX stent vs. bypass surgery in femoropopliteal lesions, 3 year results and economic analysis. J Cardiovasc Surg (Torino). 2023;64(4):413-421. doi:10.23736/S0021-9509.23.12607-3
45. Iida O, Takahara M, Soga Y, et al; ZEPHYR Investigators. 1-year results of the ZEPHYR registry (Zilver PTX for the femoral artery and proximal popliteal artery): predictors of restenosis. JACC Cardiovasc Interv. 2015;8(8):1105-1112. doi:10.1016/j.jcin.2015.03.022
46. Yokoi H, Ohki T, Kichikawa K, et al. Zilver PTX post-market surveillance study of paclitaxel-eluting stents for treating femoropopliteal artery disease in Japan: 12-month results. JACC Cardiovasc Interv. 2016;9(3):271-277. doi:10.1016/j.jcin.2015.09.035
47. Bosiers M, Peeters P, Tessarek J, Deloose K, Strickler S, Zilver PTX Single-Arm Study Investigators. The Zilver® PTX® Single Arm Study: 12-month results from the TASC C/D lesion subgroup. J Cardiovasc Surg (Torino). 2013;54(1):115-122.
48. Müller-Hülsbeck S, Keirse K, Zeller T, Schroë H, Diaz-Cartelle J. Long-term results from the MAJESTIC trial of the Eluvia paclitaxel-eluting stent for femoropopliteal treatment: 3-year follow-up. Cardiovasc Intervent Radiol. 2017;40(12):1832-1838. doi:10.1007/s00270-017-1771-5
49. Gray WA, Keirse K, Soga Y, et al; IMPERIAL Investigators. A polymer-coated, paclitaxel-eluting stent (Eluvia) versus a polymer-free, paclitaxel-coated stent (Zilver PTX) for endovascular femoropopliteal intervention (IMPERIAL): a randomised, non-inferiority trial. Lancet. 2018;392(10157):1541-1551. doi:10.1016/S0140-6736(18)32262-1
50. Müller-Hülsbeck S, Benko A, Soga Y, et al. Two-year efficacy and safety results from the IMPERIAL randomized study of the Eluvia polymer-coated drug-eluting stent and the Zilver PTX polymer-free drug-coated stent. Cardiovasc Intervent Radiol. 2021;44(3):368-375. doi:10.1007/s00270-020-02693-1
51. Shibata T, Iba Y, Shingaki M, et al. Editor’s choice - comparative analysis of three year results of two paclitaxel related stents for the management of femoropopliteal disease in a real world setting. Eur J Vasc Endovasc Surg. 2025;69(6):865-873. doi:10.1016/j.ejvs.2025.03.010
52. Müller-Hülsbeck S. EluviaTM peripheral stent system for the treatment of peripheral lesions above the knee. Expert Opin Drug Deliv. 2016;13(11):1639-1644. doi:10.1080/17425247.2016.1230098
53. Torsello GF, Stavroulakis K, Bisdas T, Cardona Y, Wichmann K, Torsello GB. Treatment of femoropopliteal artery disease with polymer-coated drug-eluting stent: 5-year results of a prospective, non-randomized study including the halo phenomenon. Cardiovasc Intervent Radiol. 2024;47(2):177-185. doi:10.1007/s00270-023-03652-2
54. Iida O, Takahara M, Soga Y, et al; CAPSICUM Investigators. 1-year outcomes of fluoropolymer-based drug-eluting stent in femoropopliteal practice: predictors of restenosis and aneurysmal degeneration. JACC Cardiovasc Interv. 2022;15(6):630-638. doi:10.1016/j.jcin.2022.01.019
55. Holden A, Gouëffic Y, Gray WA, Davis EJ, Weinberg I, Jaff MR. Hypoechoic halo imaging findings following femoropopliteal artery stent implantation: risk factors and clinical outcomes. JACC Cardiovasc Interv. 2023;16(13):1654-1664. doi:10.1016/j.jcin.2023.04.037
56. Scheinert D, Katsanos K, Zeller T, et al; ACHILLES Investigators. A prospective randomized multicenter comparison of balloon angioplasty and infrapopliteal stenting with the sirolimus-eluting stent in patients with ischemic peripheral arterial disease: 1-year results from the ACHILLES trial. J Am Coll Cardiol. 2012;60(22):2290-2295. doi:10.1016/j.jacc.2012.08.989
57. Bosiers M, Scheinert D, Peeters P, et al. Randomized comparison of everolimus-eluting versus bare-metal stents in patients with critical limb ischemia and infrapopliteal arterial occlusive disease. J Vasc Surg. 2012;55(2):390-398. doi:10.1016/j.jvs.2011.07.099
58. van Overhagen H, Nakamura M, Geraghty PJ, et al. Primary results of the SAVAL randomized trial of a paclitaxel-eluting nitinol stent versus percutaneous transluminal angioplasty in infrapopliteal arteries. Vasc Med. 2023;28(6):571-580. doi:10.1177/1358863X231199489
59. Konijn LCD, Wakkie T, Spreen MI, et al. 10-year paclitaxel dose-related outcomes of drug-eluting stents treated below the knee in patients with chronic limb-threatening ischemia (the PADI trial). Cardiovasc Intervent Radiol. 2020;43(12):1881-1888. doi:10.1007/s00270-020-02602-6
60. Varcoe RL, DeRubertis BG, Kolluri R, et al; LIFE-BTK Investigators. Drug-eluting resorbable scaffold versus angioplasty for infrapopliteal artery disease. N Engl J Med. 2024;390(1):9-19. doi:10.1056/NEJMoa2305637
61. Bosiers M, Peeters P, D’Archambeau O, et al; AMS INSIGHT Investigators. AMS INSIGHT—absorbable metal stent implantation for treatment of below-the-knee critical limb ischemia: 6-month analysis. Cardiovasc Intervent Radiol. 2009;32(3):424-435. doi:10.1007/s00270-008-9472-8
62. Varcoe RL, Schouten O, Thomas SD, Lennox AF. Experience with the Absorb everolimus-eluting bioresorbable vascular scaffold in arteries below the knee: 12-month clinical and imaging outcomes. JACC Cardiovasc Interv. 2016;9(16):1721-1728. doi:10.1016/j.jcin.2016.06.005
63. Varcoe RL, Menting TP, Thomas SD, Lennox AF. Long-term results of a prospective, single-arm evaluation of everolimus-eluting bioresorbable vascular scaffolds in infrapopliteal arteries. Catheter Cardiovasc Interv. 2021;97(1):142-149. doi:10.1002/ccd.29327
64. DeRubertis BG, Varcoe RL, Krishnan P, et al. Drug-eluting resorbable scaffold versus balloon angioplasty for below-the-knee peripheral artery disease: 2-year results from the LIFE-BTK trial. Circulation. 2025;152(15):1076-1086. doi:10.1161/CIRCULATIONAHA.125.075080
65. Lim E, Varcoe RL. Current status of and future prospects for drug-eluting stents and scaffolds in infrapopliteal arteries. J Clin Med. 2024;13(6):1757. doi:10.3390/jcm13061757
66. Bosiers MJ, Rand T, Uberoi R, et al. MOTIV bioresorbable scaffold in below-the-knee artery disease: European post-market pilot BTK trial: 36-month results. Cardiovasc Intervent Radiol. 2025;48(11):1576-1586. doi:10.1007/s00270-025-04202-8
67. R3 Vascular receives IDE approval for ELITE-BTK pivotal trial of Magnitude scaffold. Endovascular Today. November 13, 2024. Accessed January 22, 2025. https://evtoday.com/news/r3-vascular-receives-ide-approval-for-elite-btk-pivotal-trial-of-magnitude-scaffold
68. Teomim D, Fishbien I, Golomb G, Orloff L, Mayberg M, Domb AJ. Perivascular delivery of heparin for the reduction of smooth muscle cell proliferation after endothelial injury. J Control Release. 1999;60(1):129-142. doi:10.1016/s0168-3659(99)00071-1
69. Edelman ER, Adams DH, Karnovsky MJ. Effect of controlled adventitial heparin delivery on smooth muscle cell proliferation following endothelial injury. Proc Natl Acad Sci U S A. 1990;87(10):3773-3777. doi:10.1073/pnas.87.10.3773
70. Baumbach A, Oberhoff M, Herdeg C, et al. Local delivery of a low molecular weight heparin following stent implantation in the pig coronary artery. Basic Res Cardiol. 2000;95(3):173-178. doi:10.1007/s003950050179
71. Kim WH, Hong MK, Kornowski R, Tio FO, Leon MB. Saline infusion via local drug delivery catheters is associated with increased neointimal hyperplasia in a porcine coronary in-stent restenosis model. Coron Artery Dis. 1999;10(8):629-632. doi:10.1097/00019501-199912000-00012
72. Mitchel JF, Azrin MA, Fram DB, Bow LM, McKay RG. Localized delivery of heparin to angioplasty sites with iontophoresis. Cathet Cardiovasc Diagn. 1997;41(3):315-323. doi:10.1002/(sici)1097-0304(199707)41:3<315::aid-ccd13>3.0.co;2-m
73. Todd M, Nair PK, Ohayon J, Pettigrew RI, Yazdani SK. Liquid drug delivery approaches for the treatment of occlusive arterial disease: a systematic review. J Endovasc Ther. 2024;31(2):203-213. doi:10.1177/15266028221120755
74. Owens CD, Gasper WJ, Walker JP, Alley HF, Conte MS, Grenon SM. Safety and feasibility of adjunctive dexamethasone infusion into the adventitia of the femoropopliteal artery following endovascular revascularization. J Vasc Surg. 2014;59(4):1016-1024. doi:10.1016/j.jvs.2013.10.051
75. Razavi MK, Donohoe D, D’Agostino RB Jr, Jaff MR, Adams G, DANCE Investigators. Adventitial drug delivery of dexamethasone to improve primary patency in the treatment of superficial femoral and popliteal artery disease: 12-month results from the DANCE clinical trial. JACC Cardiovasc Interv. 2018;11(10):921-931. doi:10.1016/j.jcin.2017.12.015
76. Haghighat L, Altin SE, Attaran RR, Mena-Hurtado C, Regan CJ. Review of the latest percutaneous devices in critical limb ischemia. J Clin Med. 2018;7(4):82. doi:10.3390/jcm7040082
77. Latif F, Hennebry TA. Successful revascularization of re-stenosis of lower extremity arteries with localized delivery of paclitaxel. Catheter Cardiovasc Interv. 2008;72(2):294-298. doi:10.1002/ccd.21598
78. Maluenda G, Sizemore BC, Revtyak G, et al; ClearWay Registry Investigators. Intracoronary glycoprotein IIb/IIIa inhibitor infusion via a perfusion coronary catheter to decrease thrombus burden: results from the ClearWay™ Multicenter Registry. Cardiovasc Revasc Med. 2013;14(5):280-283. doi:10.1016/j.carrev.2012.12.006
79. Bunch F, Nair P, Aggarwala G, et al. A universal drug delivery catheter for the treatment of infrapopliteal arterial disease using liquid therapy. Catheter Cardiovasc Interv. 2020;96(2):393-401. doi:10.1002/ccd.28739
80. Bunch F, Walker C, Kassab E, Carr J. A universal drug delivery catheter for the treatment of infrapopliteal arterial disease: results from the multi-center first-in-human study. Catheter Cardiovasc Interv. 2018;91(2):296-301. doi:10.1002/ccd.27176
81. Villar-Matamoros E, Stokes L, Lloret A, Todd M, Tillman BW, Yazdani SK. Understanding the mechanism of drug transfer and retention of drug-coated balloons. J Cardiovasc Pharmacol Ther. 2022;27:10742484221119559. doi:10.1177/10742484221119559
82. Covidien presents 12-month DEFINITIVE AR results. Endovascular Today. November 4, 2014. Accessed February 17, 2026. https://evtoday.com/news/covidien-presents-12-month-definitive-ar-results
83. Zeller T, Langhoff R, Rocha-Singh KJ, et al; DEFINITIVE AR Investigators. Directional atherectomy followed by a paclitaxel-coated balloon to inhibit restenosis and maintain vessel patency: twelve-month results of the DEFINITIVE AR study. Circ Cardiovasc Interv. 2017;10(9):e004848. doi:10.1161/CIRCINTERVENTIONS.116.004848
84. Suriyanto MGRI, Pranata R, Kamarullah W, et al. The efficacy and safety of atherectomy combined with drug-coated balloon angioplasty vs. drug-coated balloon angioplasty for the treatment of lower extremity artery disease: a systematic review and meta-analysis. Front Cardiovasc Med. 2024;11:1472064. doi:10.3389/fcvm.2024.1472064
85. Lin F, Wang H, Ding W, Chen G, Zhang Z. Atherectomy plus drug-coated balloon versus drug-coated balloon only for treatment of femoropopliteal artery lesions: a systematic review and meta-analysis. Vascular. 2021;29(6):883-896. doi: 0.1177/1708538120985732
86. Rodoplu O, Er Z, Erdinc I, Ozturk C. Atherectomy followed by drug-coated balloon angioplasty for below knee lesions in diabetic patients. Cir Cir. 2022;90(S2):29-35. doi:10.24875/CIRU.22000131
87. Katsanos K, Spiliopoulos S, Kitrou P, Krokidis M, Paraskevopoulos I, Karnabatidis D. Risk of death and amputation with use of paclitaxel-coated balloons in the infrapopliteal arteries for treatment of critical limb ischemia: a systematic review and meta-analysis of randomized controlled trials. J Vasc Interv Radiol. 2020;31(2):202-212. doi:10.1016/j.jvir.2019.11.015
88. Parikh SA, Schneider PA, Mullin CM, Rogers T, Gray WA. Mortality in randomised controlled trials using paclitaxel-coated devices for femoropopliteal interventional procedures: an updated patient-level meta-analysis. Lancet. 2023;402(10415):1848-1856. doi:10.1016/S0140-6736(23)02189-XAff