Stem Cell–Derived Extracellular Vesicles for Chronic Limb-Threatening Ischemia: A Preclinical Scoping Review
Abstract
Chronic limb-threatening ischemia (CLTI) is a severe lower limb arterial obstructive disease that leads to a diminished quality of life and a higher risk of limb amputation. Currently, effective treatments are limited, and revascularization remains the primary focus of research. Stem cell–derived extracellular vesicles (EVs) have emerged as a promising therapeutic option for both ischemic and degenerative diseases. Notably, stem cell–derived EVs exhibit minimal tumorigenic and immunogenic risks, making them more advantageous than direct stem cell therapy. In this scoping review, Web of Science, PubMed, and Scopus databases were searched to find eligible articles. Studies were included if they evaluated the effects of stem cell–derived EVs in treating animal models of CLTI. Thirty articles were included. EVs isolated from diverse stem cell sources significantly improved blood flow, enhanced neovascularization and muscle regeneration, reduced tissue degeneration, and lowered the risk of necrosis and limb loss. These benefits mainly result from reducing inflammation, promoting angiogenesis, and delivering pro-angiogenic microRNAs. Additionally, engineered EVs demonstrated even greater therapeutic effects. Despite these promising preclinical results, further research is needed to determine optimal dosing, delivery routes, standardization of EVs, and long-term safety before clinical application in humans.
J CRIT LIMB ISCHEM 2026:6(2):E51-E60. doi: 10.25270/jcli/CLIG-2500012
Key words: cell-free therapeutics, stem cell–derived extracellular vesicles, revascularization, chronic limb-threatening ischemia, critical limb ischemia
Introduction
Peripheral arterial disease (PAD) is a condition characterized by the narrowing or blockage of the arteries in the extremities, primarily caused by atherosclerosis in more than 90% of cases.1,2 Arterial obstruction leads to the formation of ulcers, gangrene, and chronic ischemic rest discomfort in the lower extremity, which is known as chronic limb-threatening ischemia (CLTI), the most severe form of PAD.3 Approximately 200 million people are affected by PAD worldwide, and around 10% of them experience CLTI.4,5 CLTI is usually managed by the administration of drugs that help to prevent clots and reduce cardiovascular risk, performing revascularization procedures to enhance blood flow to the affected limb, and providing local wound care to manage infection and promote recovery.6 About 22% to 25% of patients die within 1 year following a diagnosis of CLTI. About 22% to 30% undergo major limb amputation and, in approximately 20% of cases, symptoms persist. It is worth noting that only 25% of cases are successfully managed with conventional treatments or therapies.7
The gold standard treatment for CLTI is endovascular and surgical revascularization, along with pharmaceutical therapy.8,9 Although surgical and endovascular therapies have made significant progress, around 20% of patients with CLTI are found unfit for revascularization surgery.10 These patients are known as “no-option” CLTI patients. Numerous advanced treatments, such as spinal cord stimulation, hyperbaric oxygen therapy, prostanoid therapy, lumbar sympathectomy, and intermittent pneumatic compression, have been developed to treat them; however, satisfactory results are not achieved.11 Recently, deep venous arterialization (DVA) has shown promising results,12 with limb salvage rates achieved up to approximately 70%.13 However, a strong negative impact limits its utilization. The most common complications caused by DVA include site complications (hematomas or bleeding), thromboembolic events (stroke or myocardial infarction [MI]), and renal complications (contrast-induced nephropathy).14 Alternatively, biological therapies such as stem cell therapy, gene therapy, and recombinant protein transfer have been developed, and stem cell therapy showed the most promising results by promoting angiogenesis and regenerating tissue.15 However, stem cell therapy has limitations due to the potential risk of tumor formation.
On the other hand, stem cell–derived EVs have shown the potential to be used as a cell-free therapeutic option for CLTI.16 This scoping review aims to summarize the therapeutic potential of stem cell–derived EVs in animal models of limb ischemia.
Stem Cells
Stem cells are unique cells present in both embryonic and adult tissue, having the capacity for self-renewal and to differentiate into various cell types.17 Five types of stem cells have been identified based on their differentiation potential: totipotent, pluripotent, multipotent, oligopotent, and unipotent.18 Totipotent stem cells such as zygotes can differentiate into any type of cell, including the placenta. On the other hand, pluripotent stem cells (PSCs), such as embryonic stem cells and induced PSCs (iPSCs), can turn into 3 germ layer cells (ectoderm, mesoderm, and endoderm), but they cannot form extra-embryonic organs.19,20 Multipotent stem cells can differentiate into multiple cell types within a single germ layer. Oligopotent stem cells are even more restricted, forming only tissue-specific cells, while unipotent stem cells can differentiate into only one specific cell type.21 Mesenchymal stem cells (MSCs) are multipotent, nonhematopoietic progenitor cells capable of differentiating into mesodermal lineages such as adipocytes, osteocytes, and chondrocytes, as well as ectodermal cells (neurocytes) and endodermal cells (hepatocytes). These versatile cells are harvested from various anatomical sites, most notably bone marrow, adipose tissue, Wharton’s jelly, umbilical cord, placenta, and amniotic fluid.22
Extracellular Vesicles
EVs are membrane-bound vesicles that carry nucleic acids, lipids, proteins, and signaling molecules, facilitating intercellular communication. Nearly all cell types secrete EVs.23,24 EVs are classified into 3 main types based on size and biogenesis: exosomes (30-150 nm), microvesicles (50-1000 nm), and apoptotic bodies.25 Exosomes originate from inward budding of the endosomal membrane,26,27 while microvesicles form through outward budding of the plasma membrane.28 Apoptotic bodies are generated during the disintegration of apoptotic cells.29 Furthermore, EVs can be broadly classified into small EVs (sEVs) <200 nm and medium/large EVs (mEVs/lEVs) >200 nm.30
Stem cells also secrete EVs, and growing evidence indicates that these vesicles mediate many of the therapeutic effects attributed to stem cell–based therapies.31 Early studies in the 2000s reported that stem cell transplantation significantly improved cardiac regeneration following MI.32,33 However, subsequent research revealed that these benefits were largely driven by paracrine factors, including stem cell–derived EVs, rather than by direct engraftment or differentiation of transplanted stem cells.34-37 Numerous studies have since demonstrated that EVs from stem/progenitor and somatic cells promote tissue repair and regeneration in models of MI, ischemic limb injury, and chronic wounds.38
Search Strategy
The Web of Science, Scopus, and PubMed databases were searched on January 1, 2025, and an updated search was conducted on January 16, 2026, using the following keywords: (((stem cell–derived exosomes) OR (stem cell–derived extracellular vesicles)) AND ((limb ischemia) OR (acute limb ischemia) OR (critical limb ischemia) OR (chronic limb-threatening ischemia) OR (peripheral artery disease))). No date or language restrictions were applied. Two authors independently searched for articles and extracted data. Disagreements about data extraction were resolved through group discussions. Studies were included in the scoping review based on the following criteria.
Inclusion criteria
- In vivo studies in humans or animals evaluating stem cell–derived EVs for lower limb ischemia.
- Comparison of stem cell–derived EVs therapy with placebo or control.
Exclusion criteria
- Non-English publications, reviews, meta-analyses, theses, editorials, or letters.
- In vitro or in silico studies.
- EVs derived from non-stem cell sources
Results
Search results
A total of 298 articles were initially identified in Scopus (n = 95), Web of Science (n = 120), and PubMed (n = 83). After removing 129 duplicates, the titles and abstracts of 169 articles were screened. Of these, 139 were excluded (38 reviews, 8 meeting abstracts, 5 full texts unavailable, 2 non-English, 3 editorials, 2 books, and 81 irrelevant). Finally, 30 articles were included in the study.16,39-67
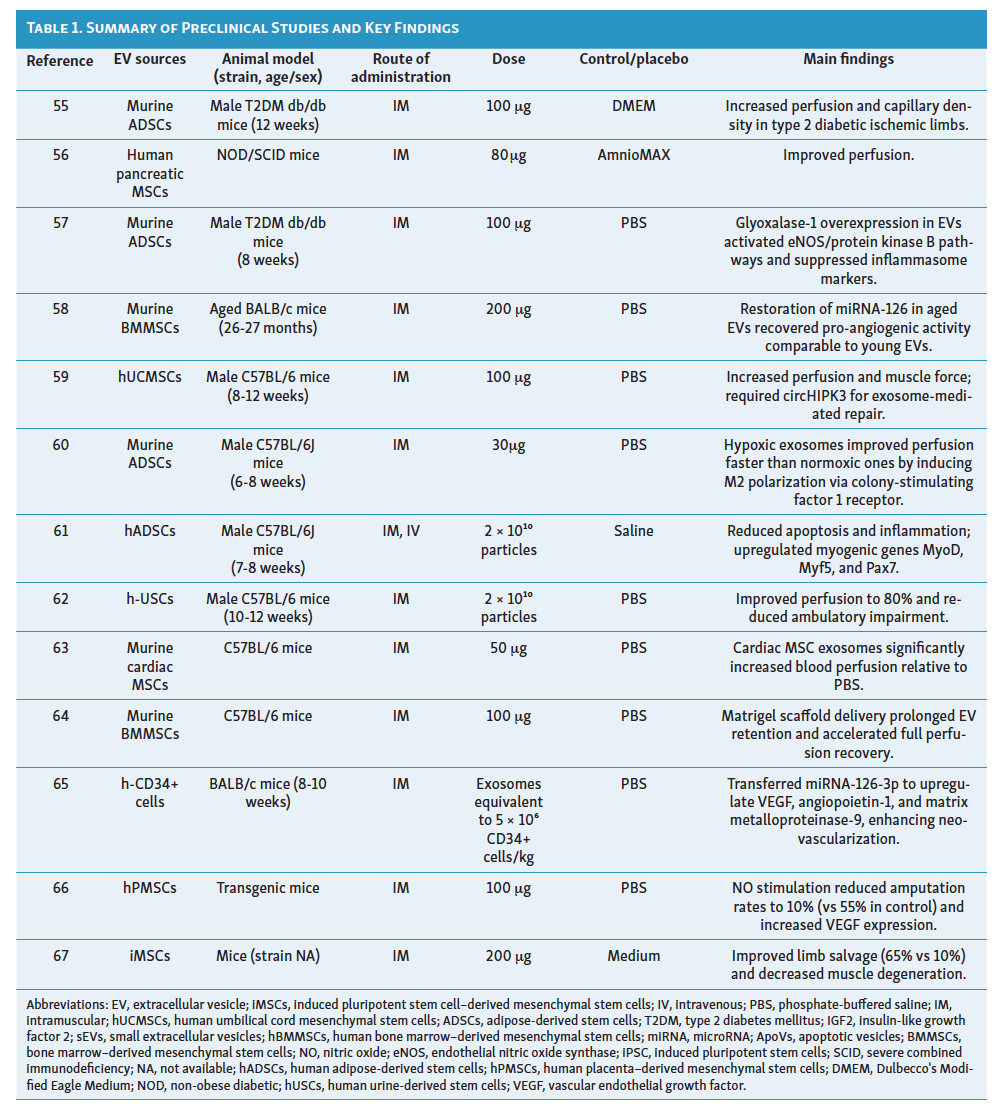
Study characteristics: sources, doses, and animal models
Various types of stem cells were utilized to isolate EVs. Adipose tissue–derived stem cells (ADSCs) were the most common source (9 studies), followed by bone marrow–derived mesenchymal stem cells (BMMSCs) (7 studies), iPSCs (5 studies), umbilical cord mesenchymal stem cells (3 studies), and placenta-derived stem cells (2 studies). Other sources included human CD34+ stem cells, urine-derived stem cells, pancreatic mesenchymal stromal cells, and murine cardiac MSCs (1 study each).
Regarding administration, only 4 studies utilized the intravenous route, while the remaining studies employed intramuscular injection. The most frequent EV dose was 100 μg (11 studies).
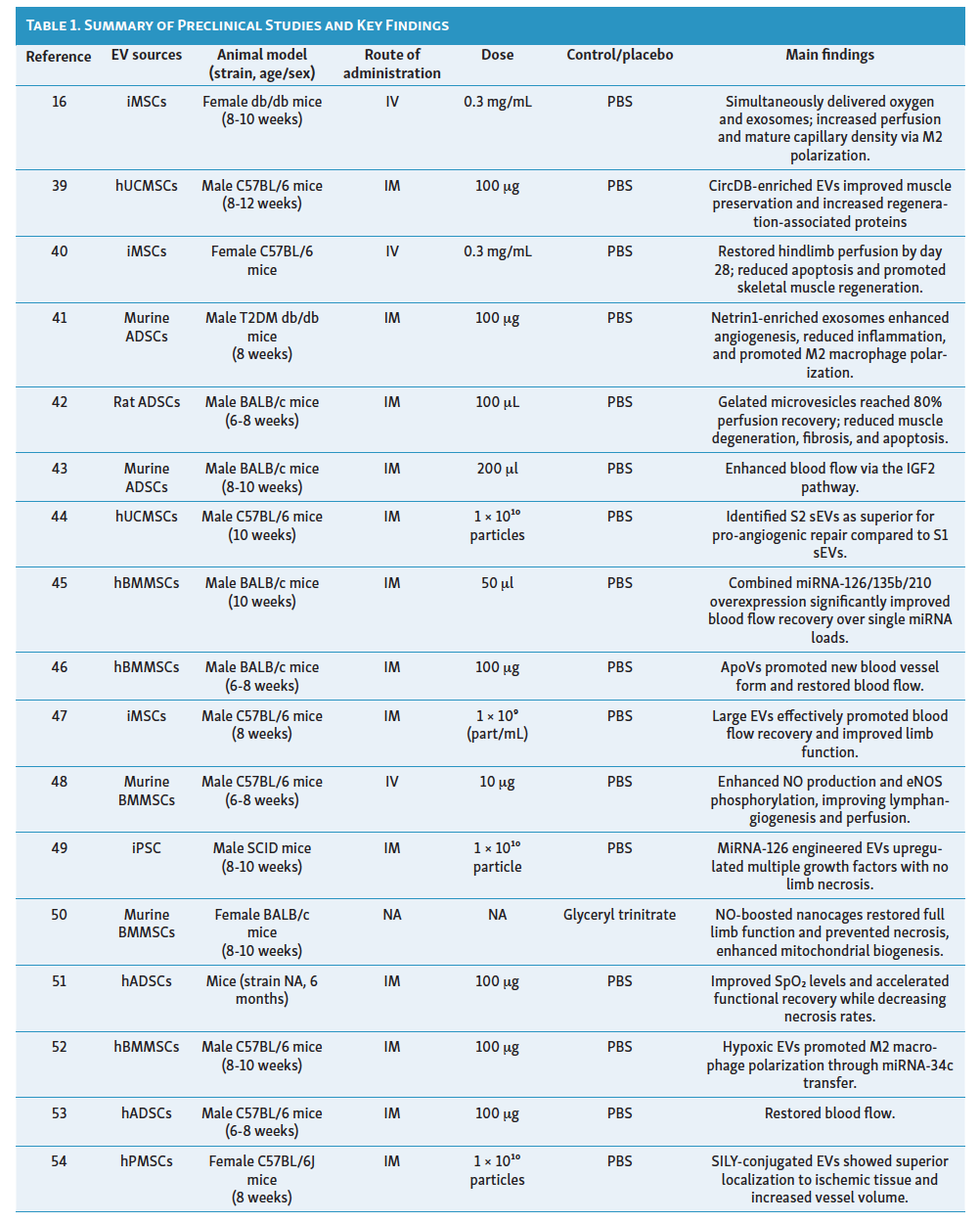
For animal models, mice were the only species used in all included preclinical research. Fourteen studies utilized C57BL/6 mice, while seven utilized BALB/c mice. In every study, limb ischemia was induced via femoral artery ligation. No clinical trial was identified. The characteristics of the included studies are presented in the Table.
Therapeutic effects of stem cell–derived extracellular vesicles
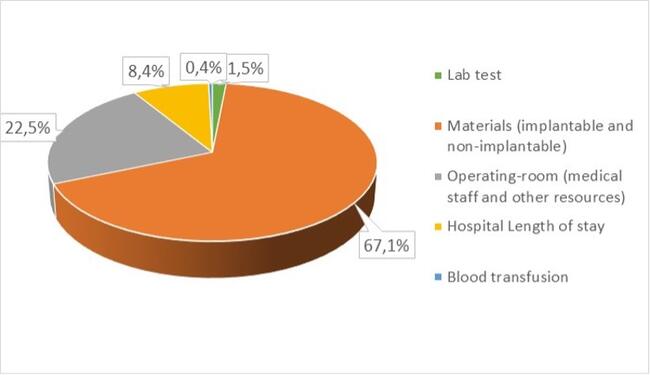
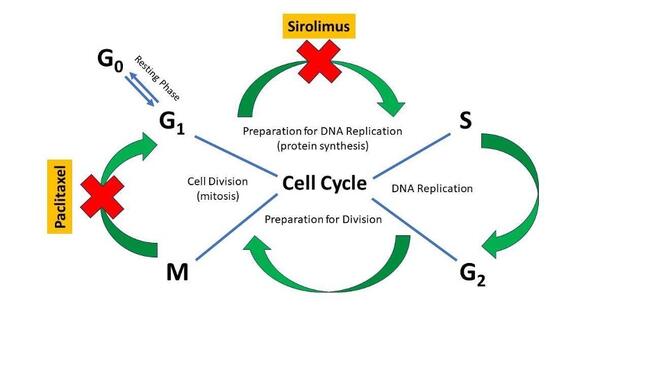
The therapeutic effects of stem cell–derived EVs are summarized in Figure 1, while the underlying mechanisms are illustrated in Figure 2.
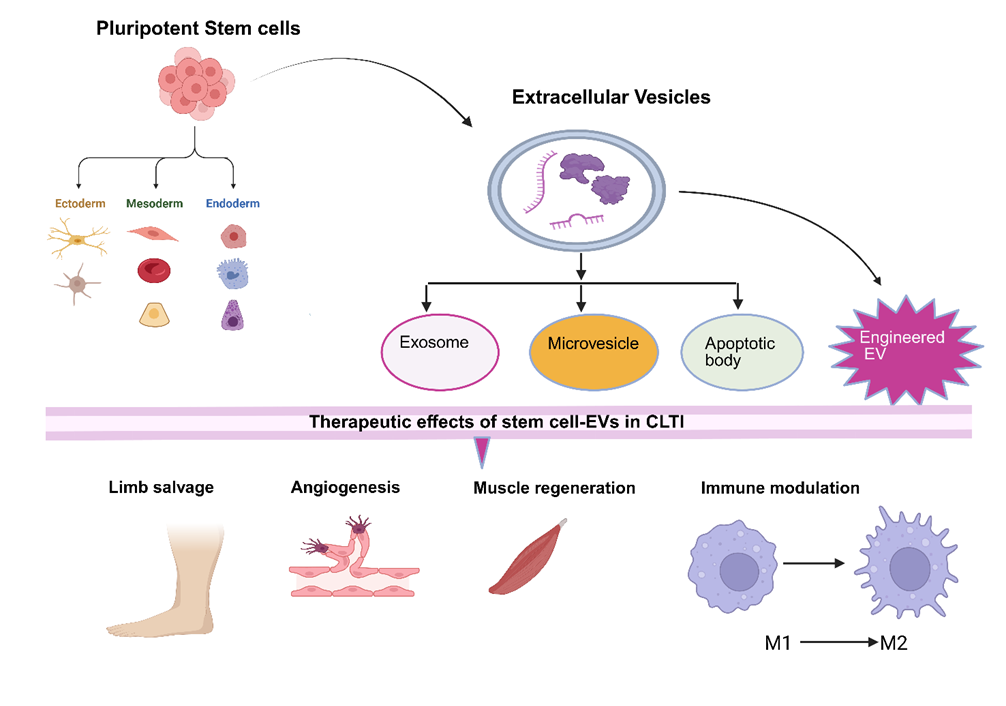
Abbreviations: EVs, extracellular vesicles; CLTI, chronic limb-threatening ischemia.
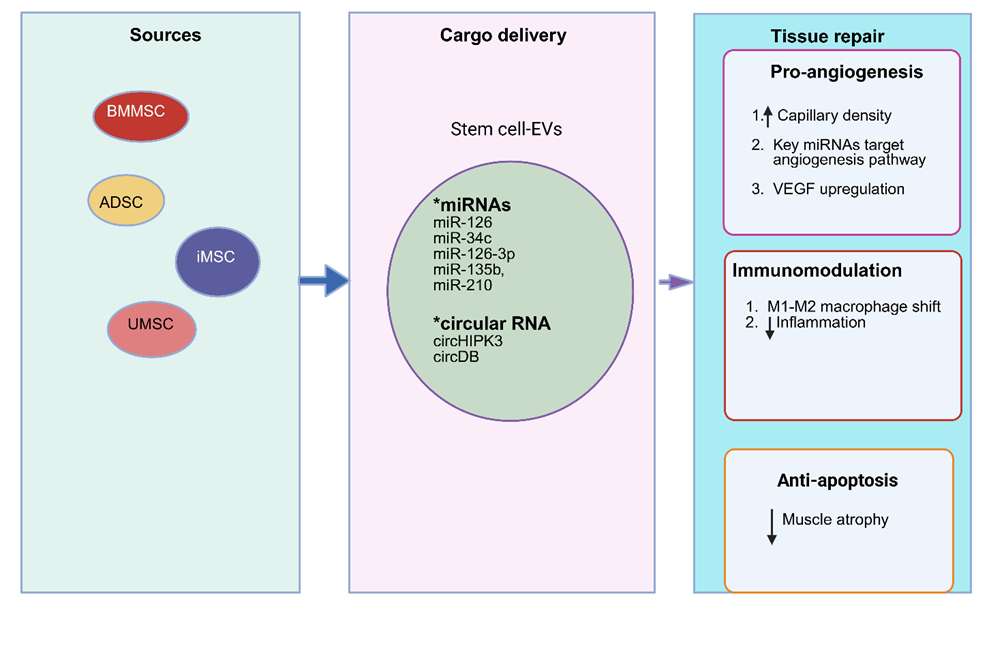
Abbreviations: BMMSC, bone marrow–derived mesenchymal stem cell; ADSC, adipose-derived stem cell; iMSC, induced pluripotent stem cell–derived mesenchymal stem cell; UMSC, umbilical cord mesenchymal stem cell; miRNA, microRNA; VEGF, vascular endothelial growth factor.
Therapeutic effects in diabetic limb ischemia models
Multiple studies demonstrated the proangiogenic and regenerative effects of stem cell–derived EVs in diabetic CLTI (D-CLTI). In type 1 diabetic mice, ADSC-exosomes (Exos) accelerated blood flow recovery, improved muscle regeneration, and enhanced neovascularization compared with phosphate-buffered saline (PBS), although limb loss rates and motor scores did not differ significantly.53 In type 2 diabetic ischemic limbs, ADSC-Exos similarly increased perfusion and capillary density relative to placebo.55 Further enhancement was achieved by overexpressing glyoxalase-1 (GLO-1) in ADSCs; GLO-1-ADSC-Exos produced greater blood perfusion, capillary formation, and muscle integrity, and suppressed inflammasome markers compared to unmodified ADSC-Exos or PBS.57
Additionally, a dual-delivery platform composed of ischemic limb–targeting exosomes and oxygen-releasing nanoparticles facilitated concurrent delivery of iPSC-derived MSC exosomes and oxygen. This simultaneous delivery significantly increased perfusion, mature capillary density, and muscle regeneration by upregulating vascular endothelial growth factor (VEGF) A and basic fibroblast growth factor mRNA, promoting M2 macrophage polarization and decreasing reactive oxygen species levels without triggering fibrosis.16
Netrin1-enriched ADSC-Exos (N-Exos) demonstrated superior therapeutic efficacy compared to unmodified ADSC-Exos in the D-CLTI model. N-Exos enhanced neovascularization, facilitated vascular remodeling, and reduced inflammation. N-Exos treatment shifted macrophage polarization toward the M2 phenotype and reduced pro-inflammatory cytokines (interlelukin [IL]-1β, IL-6, tumor necrosis factor-alpha) while enhancing anti-inflammatory cytokines (IL-4, IL-10, transforming growth factor [TGF] β1).41
Therapeutic effects of murine stem cell–derived extracellular vesicles
EVs derived from murine stem cells demonstrated significant efficacy in promoting vascular development and tissue repair. Hypoxic ADSC-Exos restored perfusion more rapidly (by day 7) than normoxic ADSC-Exos (by day 14) and induced stronger angiogenesis and arteriogenesis by promoting M2 macrophage polarization through colony-stimulating factor 1 receptor signaling.60 Another study highlighted the role of ADSC-Exos in enhancing blood flow via the insulin-like growth factor II pathway.43 Similarly, exosomes from murine cardiac mesenchymal stem cells significantly improved blood perfusion compared to PBS controls.63
A study looked at how aging affects stem cells and found that delivering microRNA-126 (miR-126) using lenti viruses into aged BMMSC-EVs helped restore their ability to promote new blood vessel growth. This led to recovery rates similar to those seen with young BMMSC-EVs.58 The research also showed that BMMSC-EVs increased nitric oxide (NO) production by activating an enzyme called endothelial NO synthase (eNOS) and reducing the levels of caveolin-1. These changes encouraged the formation of new lymphatic vessels and increased capillary density.48
Therapeutic outcomes of human stem cell–derived extracellular vesicles
Exosomes from human stem cells have shown impressive healing effects in ischemic hindlimb models. Human ADSC-Exos raised blood oxygen levels, helped muscles recover, lessened muscle damage, and reduced necrosis rates compared to PBS.51 These exosomes also lowered cell death and inflammation and increased the activity of key myogenic genes MyoD, Myf5, and Pax7.61 Hypoxic-conditioned human BMMSC-EVs provided superior perfusion and promoted M2 macrophage polarization through miR-34c transfer.52 In addition, apoptotic vesicles released by dying bone marrow stem cells (BMSC-ApoVs) helped to form new blood vessels and restored blood flow.46
Exosomes from induced pluripotent stem cell–derived mesenchymal stem cells (iMSC-Exos) reduced necrosis and enhanced limb salvage to 65% compared to 10% in controls.67 Similarly, iMSC-derived lEVs significantly improved blood flow recovery and functional improvement.47 Exosomes produced from umbilical cord mesenchymal stem cells improved running distance, muscular force, and perfusion; however, circHIPK3 silencing reduced these advantages, suggesting that circHIPK3 is necessary for repair.59 EVs produced from human urine stem cells reduced foot necrosis and raised perfusion to about 80% of normal levels.62 Similarly, human CD34+ stem cell exosomes transported miR-126-3p to upregulate VEGF, angiopoietin-1(ANG1), and matrix metalloproteinase-9, reducing necrosis,65 while human pancreas-derived MSC-EVs restored perfusion.56
Certain alterations also boosted efficacy: circular RNA DB (circDB)-enriched human umbilical cord MSC-sEVs improved muscle preservation and perfusion.39 Furthermore, 2 different subpopulations of UC-MSC-sEVs with specific roles were found. S1-sEVs showed a prominent immunomodulatory function and were characterized by high expression of CD9, HRS, and GPC1. In contrast, S2-sEVs, which were enriched with CD63 and FLOT1/2, exhibited superior pro-angiogenic properties that resulted in rapid and complete hindlimb repair and regeneration following ischemia-induced injury.44
Enhanced efficacy using engineered or modified extracellular vesicles
Several studies utilized engineering strategies to boost therapeutic outcomes.
Genetic modification: Genetically engineered iPSC-miR-126-EVs increased angiogenic genes (eg, angiopoietin, Tie-2, VEGF) and achieved strong perfusion recovery with no limb necrosis.49
BMMSC-EVs engineered to overexpress triple or double combinations of miRNAs (miR-126, miR-135b, miR-210) exhibited superior efficacy compared to single miRNA-loaded EVs.45
Bioactive scaffolds and encapsulation: Researchers developed NO-boosted BMMSC-EV nanocages (n-BANKs) that markedly enhanced limb salvage, muscle regeneration, and revascularization in ischemic mice. n-BANKs promoted full motor recovery, increased pericyte and endothelial cell content in new vessels, and strongly upregulated eNOS, leading to improved vasodilation. Unlike standard MSC-EVs, which failed to prevent limb loss, n-BANKs restored full limb function within 14 days and prevented the rapid necrosis observed in controls. Treatment also elevated chemokines associated with collateral remodeling (CXCL10, CXCL2, CCL2), increased regeneration-related cytokines (VEGFα, platelet-derived growth factor B, PGF, HB-EGF, TGFβ3), enhanced mitochondrial biogenesis gene expression, and suppressed inflammatory genes.50
Engineered collagen-binding placental chorionic villus tissue stem cells (SILY-EVs) improved localization to ischemic tissue, enhancing perfusion and muscle repair. These vesicles increased the expression of important angiogenic and myogenic genes, stimulated M2 polarization, and altered Th1/Th2 signaling (IFN-γ/IL-10).54
NO-stimulated human placental MSC exosomes improved perfusion and collateral vascular development, lowering amputation rates to 10% (compared to 55% in the PBS group). These exosomes aided repair by transferring miR-126 and upregulating important angiogenic factors such as VEGF, VEGFR2, and ANG1.66
A Matrigel scaffold facilitated the gradual release of BMMSC-EVs, extending retention and accelerating perfusion recovery.64 Rat adipose MSC-derived gelated macrovesicles enhanced blood reperfusion and limb preservation (>80%) in comparison to conventional microvesicles. Stability was improved by internal gelation, maintaining therapeutic activity even after storage.42
EVs from iMSCs cultured on HAVDI-functionalized dishes demonstrated optimal bioactivity, completely restoring perfusion by day 28.40
Discussion
This scoping review included 30 preclinical studies. All studies induced hindlimb ischemia by ligating the femoral artery of mice. Our extensive search revealed that clinical trials have not been conducted to date. Various sources of stem cells were used to isolate EVs, mostly from adipose tissue and bone marrow. The standard administration route was intramuscular (n = 26), with a common dosage of 100 μg. Therapeutic mechanisms of stem cell–derived EVs improved ischemic outcomes by facilitating blood reperfusion, stimulating angiogenesis, and promoting muscle regeneration. In diabetic models, stem cell–derived EVs countered impaired healing by activating eNOS/AKT pathways and upregulating VEGF and basic fibroblast growth factor. Mechanistically, repair was driven by the transfer of molecular cargo, including miR-126, miR-34c, and circHIPK3. Hypoxic preconditioning of BMMSC-EVs and ADSC-EVs yielded superior therapeutic outcomes compared to their normoxic counterparts. Engineered approaches demonstrated significantly superior efficacy compared with unmodified EVs. Innovations such as NO stimulation, hypoxic preconditioning, and bioactive scaffolds (eg, SILY-EVs, n-BANK nanocages) improved EV retention and localization. For instance, NO-stimulated exosomes reduced amputation rates to 10% (vs 55% in controls).
Notably, our review also highlights that different vesicle types, such as BMSC-ApoVs and lEVs, effectively promote blood flow recovery. Furthermore, we identified that EV subpopulations from the same source can have specialized roles; for instance, S1-sEVs (CD9/HRS+) drive immunomodulation while S2-sEVs (CD63/FLOT+) drive superior pro-angiogenic repair. A key finding across multiple studies was the promotion of M2 macrophage polarization, which shifts the local environment from proinflammatory to proregenerative. Macrophage polarization toward the M2 phenotype promotes angiogenesis, representing a promising therapeutic strategy for ischemic diseases.68,69 Angiogenesis, a vital process for tissue growth and repair, refers to the formation of new blood vessels from existing ones.70 Several methods have been attempted to stimulate angiogenesis in ischemic organs, including the use of VEGF and other growth factors or angiogenic proteins such as basic fibroblast growth factor and hypoxia-inducible factor-1 alpha. However, the outcomes have not been deemed satisfactory. One of the most promising experimental approaches to promote angiogenesis is cell therapy.71 A Phase II randomized clinical trial evaluated autologous, peripheral blood-derived stem cells in “no-option” PAD patients. The study demonstrated that the therapy was safe and significantly reduced major amputation rates at 3 months (0% vs 60% in controls). At the 2-year follow-up, the treated group continued to show improved hemodynamic parameters, enhanced wound healing, and increased walking ability compared to the control group.72 Similarly, allogeneic BMMSCs have been proven safe in double-blind trials, showing significant improvements in ankle-brachial index (ABI) and ankle pressure.73 In a randomized trial of 40 diabetic patients with CLTI, granulocyte colony-stimulating factor mobilized peripheral blood mononuclear cell transplantation and significantly improved ABI, transcutaneous oxygen levels, and collateral vessel development. After 12 weeks, ulcer prevalence dropped from 45% to 15% with improved limb salvage.74 In comparisons of cell sources, BMMSCs have proven superior to bone marrow–derived mononuclear cells in diabetic patients with CLTI, achieving faster ulcer healing and more significant improvements in total carbon dioxide and ABI.75 A meta-analysis of randomized controlled studies revealed that autologous stem cell therapy may have a beneficial impact on patients with PAD who have no other treatment options. However, there was no significant improvement in major limb salvage. Additionally, there were several adverse reactions.76 However, another meta-analysis of randomized controlled trials found no significant differences in major amputation rate, survival, or amputation-free survival between bone marrow–derived cell therapy and placebo therapy patients.77
While current data on stem cell–derived EVs in CLTI is preclinical, clinical trials in other therapeutic areas have confirmed their safety profile. For instance, stem cell–derived EVs administration was well-tolerated and did not induce adverse effects in patients with severe COVID-19–related acute respiratory distress syndrome78 or knee osteoarthritis.79,80 These findings, combined with the regenerative outcomes observed in our review, suggest that stem cell–derived EVs represent a safe and promising alternative treatment option for CLTI. Despite atherosclerosis being the primary driver of human CLTI, none of the included studies utilized atherosclerotic mouse models, which may limit the translatability of these findings to complex clinical cases. Furthermore, no research to date has evaluated the efficacy of stem cell–derived EVs transplantation via the intra-arterial route, a common delivery method in clinical vascular interventions.
Conclusions
Our findings indicate that stem cell–derived EVs have significant therapeutic potential in hindlimb ischemia. These stem cell–derived EVs not only restored blood perfusion and regenerated muscle tissue but also reduced the need for limb amputation and decreased necrosis. Furthermore, these effects were observed in both nondiabetic and diabetic CLTI mice. However, various types of stem cells were used to isolate the EVs, and all stem cell–derived EVs exhibited angiogenic and tissue regeneration potential. Additionally, these stem cell–derived EVs demonstrated anti-inflammatory and anti-apoptotic effects. Furthermore, stem cell–derived EVs serve as carriers for transferring various miRNAs. Innovations in EVs engineering, such as nanoparticles that carry oxygen, vesicles enriched with NO, modifications for collagen binding, and strategies to enhance miRNA content, have significantly increased their therapeutic efficacy. However, transitioning from successful preclinical findings to clinical application involves addressing existing challenges related to EV production, delivery, and regulatory processes.
Affiliations and Disclosures
Md. Mojahidur Hasan, MBBS, MMSc, and Sehreen Tory, MBBS, MMSc, are from the Department of Medical Biochemistry, Faculty of Medicine, Recep Tayyip Erdoğan University, Rize, Türkiye, and Al Mutma’innah Maa O Shishu Hospital, Rajarbag Shareef, Dhaka, Bangladesh; Yusuf Tutar, PhD, is from the Division of Biochemistry, Department of Basic Medical Sciences, Faculty of Medicine, Recep Tayyip Erdoğan University, Rize, Türkiye.
The authors have no relevant financial or non-financial interests to disclose.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Md. Mojahidur Hasan and Sehreen Tory contributed equally in conceptualization, data extraction, manuscript writing, review, and editing. Yusuf Tutar reviewed the scientific contents described in the manuscript. All authors read and approved the final submitted version of the manuscript.
Manuscript accepted April 7, 2026.
Address for Correspondence: Dr. Sehreen Tory, Department of Medical Biochemistry, Faculty of Medicine, Recep Tayyip Erdogan University, Rize, Türkiye. Email: dr.sehreentory@gmail.com
References
1. Golledge J. Update on the pathophysiology and medical treatment of peripheral artery disease. Nat Rev Cardiol. 2022;19(7):456-474. doi:10.1038/s41569-021-00663-9
2. Zamboni M, Pedriali M, Ferretto L, et al. PBMNCs treatment in critical limb ischemia and candidate biomarkers of efficacy. Diagnostics (Basel). 2022;12(5):1137. doi:10.3390/diagnostics12051137
3. Uccioli L, Meloni M, Izzo V, Giurato L, Merolla S, Gandini R. Critical limb ischemia: current challenges and future prospects. Vasc Health Risk Manag. 2018;14:63-74. doi:10.2147/VHRM.S125065
4. Conte MS, Bradbury AW, Kolh P, et al; GVG Writing Group for the Joint Guidelines of the Society for Vascular Surgery (SVS), European Society for Vascular Surgery (ESVS), World Federation of Vascular Societies (WFVS). Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1S):S1-S109. doi:10.1016/j.ejvs.2019.05.006
5. Shamaki GR, Markson F, Soji-Ayoade D, Agwuegbo CC, Bamgbose MO, Tamunoinemi B. Peripheral artery disease: a comprehensive updated review. Curr Probl Cardiol. 2022;47(11):101082. doi:10.1016/j.cpcardiol.2021.101082
6. Farber A, Menard MT, Conte MS, et al; BEST-CLI Investigators. Surgery or endovascular therapy for chronic limb-threatening ischemia. N Engl J Med. 2022;387(25):2305-2316. doi:10.1056/NEJMoa2207899
7. Kwiatkowski T, Zbierska-Rubinkiewicz K, Krzywoń JW, et al. Cellular therapies in no-option critical limb ischemia: present status and future directions. Postepy Kardiol Interwencyjnej. 2022;18(4):340-349. doi:10.5114/aic.2022.120962
8. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FGR; TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45 Suppl SS:S5-S67. doi:10.1016/j.jvs.2006.12.037
9. Wahid SFA, Ismail NA, Jamaludin WFW, et al. Autologous cells derived from different sources and administered using different regimens for ‘no‐option’ critical lower limb ischaemia patients. Cochrane Database Syst Rev. 2018;(8):CD010747. doi:10.1002/14651858.CD010747.pub2
10. Shishehbor MH, Powell RJ, Montero-Baker MF, et al; PROMISE II Investigators. Transcatheter arterialization of deep veins in chronic limb-threatening ischemia. N Engl J Med. 2023;388(13):1171-1180. doi:10.1056/NEJMoa2212754
11. Schreve MA, Vos CG, Vahl AC, et al. Venous arterialisation for salvage of critically ischaemic limbs: a systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2017;53(3):387-402. doi:10.1016/j.ejvs.2016.11.007
12. Spiliopoulos S, Davoutis E, Arkoudis N, Sritharan K, Lechareas S. Percutaneous deep venous arterialization for limb salvage in no option patients with chronic limb-threatening ischemia. J Clin Med. 2023;12(23):7324. doi:10.3390/jcm12237324
13. Saab FA, Mustapha JA, Ansari M, et al. Percutaneous deep venous arterialization: treatment of patients with end-stage plantar disease. J Soc Cardiovasc Angiogr Interv. 2022;1(6):100437. doi:10.1016/j.jscai.2022.100437
14. Schreve MA, Lichtenberg M, Ünlü Ç, et al. PROMISE international; a clinical post marketing trial investigating the percutaneous deep vein arterialization (LimFlow) in the treatment of no-option chronic limb ischemia patient. CVIR Endovasc. 2019;2(1):26. doi:10.1186/s42155-019-0067-z
15. Lozano Navarro LV, Chen X, Giratá Viviescas LT, et al. Mesenchymal stem cells for critical limb ischemia: their function, mechanism, and therapeutic potential. Stem Cell Res Ther. 2022;13(1):345. doi:10.1186/s13287-022-03043-3
16. Zhong T, Gao N, Guan Y, Liu Z, Guan J. Co-delivery of bioengineered exosomes and oxygen for treating critical limb ischemia in diabetic mice. ACS Nano. 2023;17(24):25157-25174. doi:10.1021/acsnano.3c08088
17. Suman S, Domingues A, Ratajczak J, Ratajczak MZ. Potential clinical applications of stem cells in regenerative medicine. Adv Exp Med Biol. 2019;1201:1-22. doi: 10.1007/978-3-030-31206-0_1
18. Smith A. A glossary for stem-cell biology. Nature. 2006;441(7097):1060. doi:10.1038/nature04954
19. Ghazimoradi MH, Khalafizadeh A, Babashah S. A critical review on induced totipotent stem cells: types and methods. Stem Cell Res. 2022;63:1028 doi:10.1016/j.scr.2022.102857.57
20. Martí M, Mulero L, Pardo C, et al. Characterization of pluripotent stem cells. Nat Protoc. 2013;8(2):223-253. doi:10.1038/nprot.2012.154
21. Kolios G, Moodley Y. Introduction to stem cells and regenerative medicine. Respiration. 2012;85(1):3-10. doi:10.1159/000345615
22. Margiana R, Markov A, Zekiy AO, et al. Clinical application of mesenchymal stem cell in regenerative medicine: a narrative review. Stem Cell Res Ther. 2022;13(1):366. doi:10.1186/s13287-022-03054-0
23. Cocozza F, Grisard E, Martin-Jaular L, Mathieu M, Théry C. SnapShot: extracellular vesicles. Cell. 2020;182(1):262-262.e1. doi:10.1016/j.cell.2020.04.054
24. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367(6478):eaau6977. doi:10.1126/science.aau6977
25. Zhou M, Li Y, Tang Y, et al. Apoptotic bodies for advanced drug delivery and therapy. J Control Release. 2022;351:394-406. doi:10.1016/j.jconrel.2022.09.045
26. Harding C, Heuser J, Stahl P. Endocytosis and intracellular processing of transferrin and colloidal gold-transferrin in rat reticulocytes: demonstration of a pathway for receptor shedding. Eur J Cell Biol. 1984;35(2):256-263.
27. Pan BT, Teng K, Wu C, Adam M, Johnstone RM. Electron microscopic evidence for externalization of the transferrin receptor in vesicular form in sheep reticulocytes. J Cell Biol. 1985;101(3):942-948. doi:10.1083/jcb.101.3.942
28. Tricarico C, Clancy J, D’Souza-Schorey C. Biology and biogenesis of shed microvesicles. Small GTPases. 2017;8(4):220-232. doi:10.1080/21541248.2016.1215283
29. Caruso S, Poon IKH. Apoptotic cell-derived extracellular vesicles: more than just debris. Front Immunol. 2018;9:1486. doi:10.3389/fimmu.2018.01486
30. Fyfe J, Dye D, Razak NBA, Metharom P, Falasca M. Immune evasion on the nanoscale: small extracellular vesicles in pancreatic ductal adenocarcinoma immunity. Semin Cancer Biol. 2023;96:36-47. doi:10.1016/j.semcancer.2023.09.004
31. Jung H, Jung Y, Seo J, Bae Y, Kim H, Jeong W. Roles of extracellular vesicles from mesenchymal stem cells in regeneration. Mol Cells. 2024;47(12):100151. doi:10.1016/j.mocell.2024.100151
32. Mangi AA, Noiseux N, Kong D, et al. Mesenchymal stem cells modified with Akt prevent remodeling and restore performance of infarcted hearts. Nat Med. 2003;9(9):1195-1201. doi:10.1038/nm912
33. Kawamoto A, Iwasaki H, Kusano K, et al. CD34-positive cells exhibit increased potency and safety for therapeutic neovascularization after myocardial infarction compared with total mononuclear cells. Circulation. 2006;114(20):2163-2169. doi:10.1161/CIRCULATIONAHA.106.644518
34. Timmers L, Lim SK, Arslan F, et al. Reduction of myocardial infarct size by human mesenchymal stem cell conditioned medium. Stem Cell Res. 2007;1(2):129-137. doi:10.1016/j.scr.2008.02.002
35. Gnecchi M, He H, Liang OD, et al. Paracrine action accounts for marked protection of ischemic heart by Akt-modified mesenchymal stem cells. Nat Med. 2005;11(4):367-368. doi:10.1038/nm0405-367
36. Sahoo S, Klychko E, Thorne T, et al. Exosomes from human CD34(+) stem cells mediate their proangiogenic paracrine activity. Circ Res. 2011;109(7):724-728. doi:10.1161/CIRCRESAHA.111.253286
37. Lai RC, Arslan F, Lee MM, et al. Exosome secreted by MSC reduces myocardial ischemia/reperfusion injury. Stem Cell Res. 2010;4(3):214-222. doi:10.1016/j.scr.2009.12.003
38. de Abreu RC, Fernandes H, da Costa Martins PA, Sahoo S, Emanueli C, Ferreira L. Native and bioengineered extracellular vesicles for cardiovascular therapeutics. Nat Rev Cardiol. 2020;17(11):685-697. doi:10.1038/s41569-020-0389-5
39. Jiao L, Han Q, Xu Y, et al. Extracellular vesicles-delivered circDB promotes ischemic muscle repair through the miR-34a/USP7/Notch1 signaling pathway. Regen Ther. 2025;30:616-628. doi:10.1016/j.reth.2025.08.009
40. Zhong T, Gao N, Niu H, et al. Targeted delivery of engineered extracellular vesicles to simultaneously promote vascularization and muscle regeneration in ischemic limbs. J Control Release. 2025;384:113938. doi:10.1016/j.jconrel.2025.113938
41. Jiang Y, Hu J, Cui C, et al. Netrin1-enriched exosomes from genetically modified ADSCs as a novel treatment for diabetic limb ischemia. Adv Healthc Mater. 2025;14(2):e2403521. doi:10.1002/adhm.202403521
42. Liu C, Xie W, Li X, Dong Z, Fu X. Intravesicular gelation of mesenchymal stromal cell-derived microvesicles for enhanced therapeutic angiogenesis in lower limb ischemia. J Mater Chem B. 2026;14(1):273-288. doi:10.1039/d5tb01411e
43. Li X, Chen Q, Li R, et al. Insulin growth factor 2 contributes to adipose stem cell-derived exosome mediated angiogenesis against hind-limb ischemia injury. Cytokine. 2025;193:156984. doi:10.1016/j.cyto.2025.156984
44. Liu W, Wang X, Chen Y, et al. Distinct molecular properties and functions of small EV subpopulations isolated from human umbilical cord MSCs using tangential flow filtration combined with size exclusion chromatography. J Extracell Vesicles. 2025;14(1):e70029. doi:10.1002/jev2.70029
45. Wada Y, Kudo T, Koyanagi A, et al. Angiogenic ability of extracellular vesicles derived from angio-miRNA-modified mesenchymal stromal cells. Tissue Eng Regen Med. 2025;22(7):993-1003. doi:10.1007/s13770-025-00741-w
46. Chen J, Shen Z, Chen B, et al. Apoptotic vesicles derived from bone marrow mesenchymal stem cells increase angiogenesis in a hind limb ischemia model via the NAMPT/SIRT1/FOXO1 axis. Stem Cell Res Ther. 2025;16(1):105. doi:10.1186/s13287-025-04245-1
47. Huang Z, Chen Z, Ye T, et al. Large extracellular vesicles from induced pluripotent stem cell-marrow stem cells enhance limb angiogenesis via ERK/MAPK. Nanomedicine (Lond). 2024;19(17):1525-1539. doi:10.1080/17435889.2024.2363743
48. Łabędź-Masłowska A, Vergori L, Kędracka-Krok S, et al. Mesenchymal stem cell-derived extracellular vesicles exert pro-angiogenic and pro-lymphangiogenic effects in ischemic tissues by transferring various microRNAs and proteins including ITGa5 and NRP1. J Nanobiotechnology. 2024;22(1):60. doi:10.1186/s12951-024-02304-y
49. Kmiotek‐Wasylewska K, Łabędź‐Masłowska A, Bobis‐Wozowicz S, et al. Induced pluripotent stem cell-derived extracellular vesicles enriched with miR‐126 induce proangiogenic properties and promote repair of ischemic tissue. FASEB J. 2024;38(2):e23415. doi:10.1096/fj.202301836R\
50. Guo L, Yang Q, Wei R, et al. Enhanced pericyte-endothelial interactions through NO-boosted extracellular vesicles drive revascularization in a mouse model of ischemic injury. Nat Commun. 2023;14(1):7334. doi:10.1038/s41467-023-43153-x
51. Nguyen TH, Pham PV, Vu NB. Exosomes from adipose-derived stem cells promote angiogenesis and reduce necrotic grade in hindlimb ischemia mouse models. Iran J Basic Med Sci. 2023;26(4):429-437. doi:10.22038/IJBMS.2023.67936.14857
52. Peng X, Liu J, Ren L, et al. Extracellular vesicles derived from hypoxia-preconditioned bone marrow mesenchymal stem cells ameliorate lower limb ischemia by delivering miR-34c. Mol Cell Biochem. 2023;478(7):1645-1658. doi:10.1007/s11010-023-04666-7
53. Guo J, Yang X, Chen J, et al. Exosomal miR-125b-5p derived from adipose-derived mesenchymal stem cells enhance diabetic hindlimb ischemia repair via targeting alkaline ceramidase 2. J Nanobiotechnology. 2023;21(1):189. doi:10.1186/s12951-023-01954-8
54. Hao D, Lu L, Song H, et al. Engineered extracellular vesicles with high collagen-binding affinity present superior in situ retention and therapeutic efficacy in tissue repair. Theranostics. 2022;12(13):6021-6037. doi:10.7150/thno.70448
55. Wang X, Chen S, Lu R, et al. Adipose-derived stem cell-secreted exosomes enhance angiogenesis by promoting macrophage M2 polarization in type 2 diabetic mice with limb ischemia via the JAK/STAT6 pathway. Heliyon. 2022;8(11):e11495. doi:10.1016/j.heliyon.2022.e11495
56. Cooper TT, Sherman SE, Bell GI, et al. Ultrafiltration and injection of islet regenerative stimuli secreted by pancreatic mesenchymal stromal cells. Stem Cells Dev. 2021;30(5):247-264. doi:10.1089/scd.2020.0206
57. Zhang X, Jiang Y, Huang Q, et al. Exosomes derived from adipose-derived stem cells overexpressing glyoxalase-1 protect endothelial cells and enhance angiogenesis in type 2 diabetic mice with limb ischemia. Stem Cell Res Ther. 2021;12(1):403. doi:10.1186/s13287-021-02475-7
58. Wang L, Wei J, Da Fonseca Ferreira A, et al. Rejuvenation of senescent endothelial progenitor cells by extracellular vesicles derived from mesenchymal stromal cells. JACC Basic Transl Sci. 2020;5(11):1127-1141. doi:10.1016/j.jacbts.2020.08.005
59. Yan B, Zhang Y, Liang C, et al. Stem cell-derived exosomes prevent pyroptosis and repair ischemic muscle injury through a novel exosome/circHIPK3/ FOXO3a pathway. Theranostics. 2020;10(15):6728-6742. doi:10.7150/thno.42259
60. Zhu D, Johnson TK, Wang Y, et al. Macrophage M2 polarization induced by exosomes from adipose-derived stem cells contributes to the exosomal proangiogenic effect on mouse ischemic hindlimb. Stem Cell Res Ther. 2020;11(1):162. doi:10.1186/s13287-020-01669-9
61. Figliolini F, Ranghino A, Grange C, et al. Extracellular vesicles from adipose stem cells prevent muscle damage and inflammation in a mouse model of hind limb ischemia: role of neuregulin-1. Arterioscler Thromb Vasc Biol. 2020;40(1):239-254. doi:10.1161/ATVBAHA.119.313506
62. Zhu Q, Li Q, Niu X, et al. Extracellular vesicles secreted by human urine-derived stem cells promote ischemia repair in a mouse model of hind-limb ischemia. Cell Physiol Biochem. 2018;47(3):1181-1192. doi:10.1159/000490214
63. Ju C, Li Y, Shen Y, et al. Transplantation of cardiac mesenchymal stem cell-derived exosomes for angiogenesis. J Cardiovasc Transl Res. 2018;11(5):429-437. doi:10.1007/s12265-018-9824-y
64. Gangadaran P, Rajendran RL, Lee HW, et al. Extracellular vesicles from mesenchymal stem cells activates VEGF receptors and accelerates recovery of hindlimb ischemia. J Control Release. 2017;264:112-126. doi:10.1016/j.jconrel.2017.08.022
65. Mathiyalagan P, Liang Y, Kim D, et al. Angiogenic mechanisms of human CD34(+) stem cell exosomes in the repair of ischemic hindlimb. Circ Res. 2017;120(9):1466-1476. doi:10.1161/CIRCRESAHA.116.310557
66. Du W, Zhang K, Zhang S, et al. Enhanced proangiogenic potential of mesenchymal stem cell-derived exosomes stimulated by a nitric oxide releasing polymer. Biomaterials. 2017;133:70-81. doi:10.1016/j.biomaterials.2017.04.030
67. Hu G, Li Q, Niu X, et al. Exosomes secreted by human-induced pluripotent stem cell-derived mesenchymal stem cells attenuate limb ischemia by promoting angiogenesis in mice. Stem Cell Res Ther. 2015;6(1):10. doi:10.1186/scrt546
68. Takeda Y, Costa S, Delamarre E, et al. Macrophage skewing by Phd2 haplodeficiency prevents ischaemia by inducing arteriogenesis. Nature. 2011;479(7371):122-126. doi:10.1038/nature10507
69. Jetten N, Verbruggen S, Gijbels MJ, Post MJ, De Winther MPJ, Donners MMPC. Anti-inflammatory M2, but not pro-inflammatory M1 macrophages promote angiogenesis in vivo. Angiogenesis. 2014;17(1):109-118. doi:10.1007/s10456-013-9381-6
70. Rizzi A, Benagiano V, Ribatti D. Angiogenesis versus arteriogenesis. Rom J Morphol Embryol. 2017;58(1):15-19.
71. Ouma GO, Zafrir B, Mohler ER 3rd, Flugelman MY. Therapeutic angiogenesis in critical limb ischemia. Angiology. 2013;64(6):466-480. doi:10.1177/0003319712464514
72. Szabó GV, Kövesd Z, Cserepes J, Daróczy J, Belkin M, Acsády G. Peripheral blood-derived autologous stem cell therapy for the treatment of patients with late-stage peripheral artery disease-results of the short- and long-term follow-up. Cytotherapy. 2013;15(10):1245-1252. doi:10.1016/j.jcyt.2013.05.017
73. Gupta PK, Chullikana A, Parakh R, et al. A double blind randomized placebo controlled phase I/II study assessing the safety and efficacy of allogeneic bone marrow derived mesenchymal stem cell in critical limb ischemia. J Transl Med. 2013;11:143. doi:10.1186/1479-5876-11-143
74. Ozturk A, Kucukardali Y, Tangi F, et al. Therapeutical potential of autologous peripheral blood mononuclear cell transplantation in patients with type 2 diabetic critical limb ischemia. J Diabetes Complications. 2012;26(1):29-33. doi:10.1016/j.jdiacomp.2011.11.007
75. Lu D, Chen B, Liang Z, et al. Comparison of bone marrow mesenchymal stem cells with bone marrow-derived mononuclear cells for treatment of diabetic critical limb ischemia and foot ulcer: a double-blind, randomized, controlled trial. Diabetes Res Clin Pract. 2011;92(1):26-36. doi:10.1016/j.diabres.2010.12.010
76. Gao W, Chen D, Liu G, Ran X. Autologous stem cell therapy for peripheral arterial disease: a systematic review and meta-analysis of randomized controlled trials. Stem Cell Res Ther. 2019;10(1):140. doi:10.1186/s13287-019-1254-5
77. Peeters Weem SMO, Teraa M, de Borst GJ, Verhaar MC, Moll FL. Bone marrow derived cell therapy in critical limb ischemia: a meta-analysis of randomized placebo controlled trials. Eur J Vasc Endovasc Surg. 2015;50(6):775-783. doi:10.1016/j.ejvs.2015.08.018
78. Lightner AL, Sengupta V, Qian S, et al. Bone marrow mesenchymal stem cell-derived extracellular vesicle infusion for the treatment of respiratory failure from COVID-19: a randomized, placebo-controlled dosing clinical trial. Chest. 2023;164(6):1444-1453. doi:10.1016/j.chest.2023.06.024
79. Wang Y, Kong Y, Du J, et al. Injection of human umbilical cord mesenchymal stem cells exosomes for the treatment of knee osteoarthritis: from preclinical to clinical research. J Transl Med. 2025;23(1):641. doi:10.1186/s12967-025-06623-y
80. Bolandnazar NS, Raeissadat SA, Haghighatkhah H, et al. Safety and efficacy of placental mesenchymal stromal cells-derived extracellular vesicles in knee osteoarthritis: a randomized, triple-blind, placebo-controlled clinical trial. BMC Musculoskelet Disord. 2024;25(1):856. doi:10.1186/s12891-024-07979-w