Direct Cost of Percutaneous Deep Vein Arterialization: A Retrospective Analysis From a Single Center in Italy
Abstract
Objectives: To evaluate health care resource utilization and hospital costs associated with percutaneous deep vein arterialization (pDVA) in patients with chronic limb-threatening ischemia (CLTI) and to estimate the total hospital costs of the treatment pathway leading to limb healing. Methods: A single-center retrospective cohort study using hospital electronic health records was conducted. Adult patients with Rutherford class 5 or 6 CLTI, ineligible for surgical or endovascular revascularization, who underwent pDVA between March 2019 and August 2021, were included. A cost analysis was conducted from the hospital’s perspective to estimate pDVA-related and follow-up hospital costs from the index procedure to 1-year follow-up. Results: The analysis included 19 adult patients and a total of 22 limbs not eligible for surgical or endovascular arterial revascularization. The average pDVA hospitalization cost to perform pDVA in a single limb was estimated at €19,997 (US $23,279), compared with a median diagnosis-related group (DRG) reimbursement of €13,325 (US $15,512). Materials accounted for 67.1% of costs, followed by operating room expenses (22.5%) and length of stay (8.4%). At 12 months, 45% of limbs were healed, while during the follow-up 23% underwent amputation. The mean follow-up cost per healed limb was €25,158 (US $29,286); combined with pDVA costs (€19,523 [US $22,727]), the total cost for limb healing was €44,681 (US $52,013). Mean DRG reimbursement for healed limbs was €63,508 (US $73,930), yielding a positive hospital margin of €18,827 (US $21,917). Conclusions: Although pDVA is associated with high material costs, this single-center exploratory analysis suggests that completing the entire treatment pathway may be economically feasible from the hospital’s perspective.
J CRIT LIMB ISCHEM 2026:6(2):E70-E77. doi: 10.25270/jcli/CLIG-2600003
Key words: percutaneous deep vein arterialization, economic evaluation, retrospective analysis, chronic limb-threatening ischemia
Introduction
Chronic limb-threatening ischemia (CLTI) represents the most severe form of peripheral arterial disease (PAD) in combination with ischemic rest pain, nonhealing foot wounds, and/or gangrene that persists for more than 2 weeks.1 CLTI affects approximately 11% of patients with PAD, and its incidence continues to rise rapidly,2 driven by an aging population and the growing incidence of diabetes mellitus and other correlated risk factors, such as smoking, hypertension, and dyslipidemia.3 From the literature referring to national context, it emerges that despite serious implications associated with CLTI, it continues to be insufficiently recognized and is frequently diagnosed only at an advanced stage.4 The persistently high rates of late presentation and delayed therapeutic intervention continue to represent critical factors contributing to the elevated incidence of major amputations.5 Revascularization (endovascular intervention or open surgery) has been established as the standard of care for patients with CLTI. Despite significant advancements in revascularization techniques, surgical or endovascular revascularization may still be impractical for some patients, resulting in reductions in quality of life, higher risk of major amputation, and increased morbidity and mortality. Even when technically feasible, severe comorbidities and limited life expectancy can make the procedure unsuitable.6 In approximately 15% to 20% of patients with CLTI, studies have shown that revascularization is either not feasible or proves ineffective.7 This condition, known as no-option CLTI, is most common in patients with diabetes and end-stage renal disease, who often present with severe calcification in the arteries below the knee and ankle.7
The primary treatment goals for patients with CLTI are to relieve ischemic pain, reduce the risk of limb loss, and improve overall quality of life. Achieving these goals typically involves a combination of conservative management, which includes pharmacotherapy, control of cardiovascular risk factors, and professional wound care in cases of tissue loss.6
Over the past decade, several alternative treatments have been explored for patients at risk of major amputation, including stem cell therapy, vasoactive agents, and spinal cord stimulation. However, reviews of these indirect revascularization approaches have demonstrated limited effectiveness. Both stem cell and vasoactive therapies have failed to show a significant reduction in major amputation rates, while spinal cord stimulation has shown only modest benefits.7 Emerging treatment alternatives have shown promising results for patients with no-option CLTI who have failed both conventional endovascular and open surgical treatments. One innovative approach involves the use of percutaneous techniques to achieve revascularization through deep vein arterialization (DVA). Percutaneous DVA (pDVA) involves creating a percutaneous anastomosis between a proximal arterial inflow site and a retrograde venous outflow pathway, enabling blood flow to perfuse lower extremity wounds.8
Recent studies have identified pDVA as a promising treatment option for patients with no-option CLTI, demonstrating improved amputation-free survival (AFS) and higher limb salvage rates compared to standard of care.9 Several studies also highlighted the substantial economic burden of major amputations, particularly the direct costs of surgery, rehabilitation, and long-term home care, indicating the importance of effective limb salvage strategies. While no studies to date have comprehensively quantified the indirect costs of amputation in patients with CLTI, their impact is widely acknowledged. Indirect costs are largely driven by loss of productivity, affecting not only the patients but also their families, caregivers, and the broader socioeconomic system.
The aim of this study is to update the previously published analysis about the estimation of the Healthcare Resource Utilization (HRU) and average costs incurred by the hospital for a single-limb pDVA procedure hospitalization using data coming from a single center in Italy.10 The study also aims to estimate the average hospital costs for the treatment pathway to get complete healing and regained mobility. pDVA-related hospital costs and follow-up costs for healed limbs incurred by the hospital will also be compared with the national DRG reimbursement tariff associated with each hospital admission to explore efficiency in hospital care provision.
Materials and Methods
This study was designed as a retrospective cohort analysis using electronic health records registered from the hospital system of a single center in Italy. The analysis focused on adult patients classified as Rutherford Class 5 or 6 who were not eligible for surgical or endovascular arterial revascularization, as these stages reflect the most severe presentations of CLTI. The overall clinical profile of the cohort of patients was delineated by considering several characteristics: history of previous revascularization, hypertension, diabetes mellitus, hyperlipidemia, cardiovascular disease (history of heart disease), left ventricular ejection fraction, chronic renal disease, median glomerular filtration rate, and corticosteroid therapy. These patients underwent a pDVA procedure between March 2019 and August 2021. An off-the-shelf pDVA technique was used, as the LimFlow system was not available in Italy. The date on which the pDVA procedure was performed was designated as the “index date” for each patient. This index date was used as a reference point for all subsequent analyses, including HRU and cost assessments. By standardizing the index date, the study ensured consistency in measuring clinical outcomes, resource use, and cost implications relative to the pDVA procedure. The only intervention performed during the index procedure was the pDVA. No additional surgical, endovascular, or adjunctive procedures were carried out during the same hospitalization. This standardization allowed for a focused evaluation of the costs and resource utilization directly related to the pDVA procedure, avoiding potential confounding from other concurrent procedures that might influence the overall cost. The hospital cost associated with the treatment pathway to get complete healing and regained mobility was calculated from the index date (date of pDVA procedure) to 1-year follow-up. pDVA procedure and HRU associated costs were evaluated using, where available, the actual hospital costs; otherwise, data from the literature and national tariff were used. It is important to highlight that this analysis is based on Italian pricing, and therefore the economic results may differ in other countries. Finally, a deterministic sensitivity analysis was conducted to assess the uncertainty of some parameters included in the analysis on the results.
Percutaneous deep vein arterialization technique
Through the ipsilateral common femoral artery, percutaneous arteriovenous connection was established using an intravascular ultrasound-guided needle catheter (Pioneer Plus, Philips). Following this, venous valve disruption was carried out to allow retrograde arterial flow into the foot. To direct flow distally, covered stents of 5.0 mm in diameter and 0.018″ (Gore Viabahn endoprosthesis, W. L. Gore & Associates) were deployed from the artery into the vein, typically extending to the level of the common plantar vein. Final angiography confirmed the successful establishment of arterial flow into the venous system of the foot. All patients received postprocedural medical therapy consisting of an oral anticoagulant, maintained at an international normalized ratio between 1.5 and 2.0, in combination with a single antiplatelet agent.11
Cost categories
The analysis included several key cost categories to ensure a complete view of resource utilization and expenditure. The main cost categories considered were:
- implantable and non-implantable material during the procedure;
- operating room for the procedure;
- hospital length of stay;
- lab testing and imaging in preparation and during the hospital stay;
- wound dressings;
- blood transfusions.
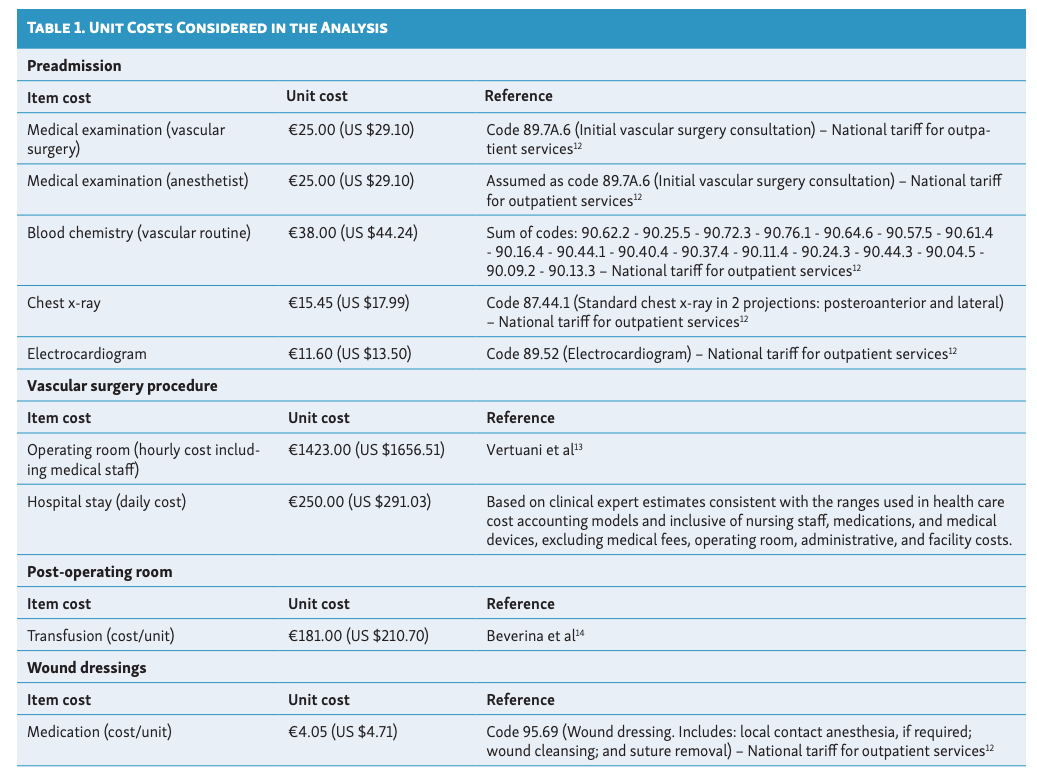
The cost associated with the operating room costs included the operating room cost and staff cost for the duration of the procedure. The last-mentioned cost item included blood tests, imaging studies, and other diagnostic procedures required to support clinical decision-making before, during, and after the procedure. The analysis of laboratory testing costs was limited to the material components of the service and did not include the costs of the physician’s time, nursing support, or technician labor required to conduct the testing. Costs associated with laboratory tests and materials used during the procedure were obtained directly from the single center’s data. Unit cost of preadmission visits or tests, medication, single hospital stays, transfusions, hourly cost of the operating room, and the cost of wound dressings were sourced from the national tariff for outpatient service or from the literature (Table 1). All costs are referred to single limb, or more precisely, to the procedures performed per limb. Follow-up–related costs included all procedures undergone by each patient to manage the limb.
Results
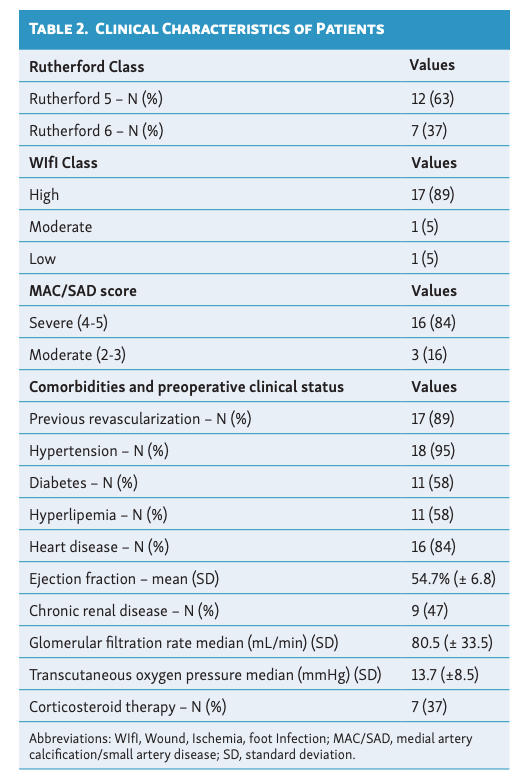
The cohort included 19 patients (16 men and 3 women) and a total of 22 limbs (11 right and 11 left). The majority of patients presented with Rutherford Class 5 (63%), a high Wound, Ischemia, foot Infection (WIfI) class (89%), and a severe medial artery calcification/small artery disease (MAC/SAD) score (84%). Clinical characteristics of patients are reported in Table 2.
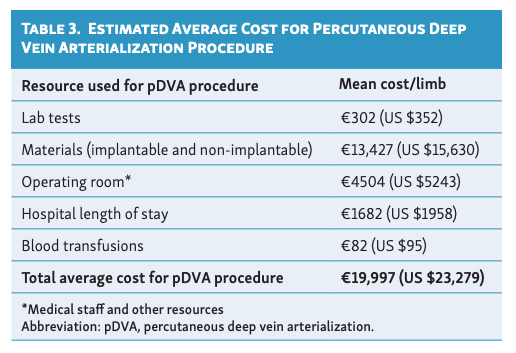
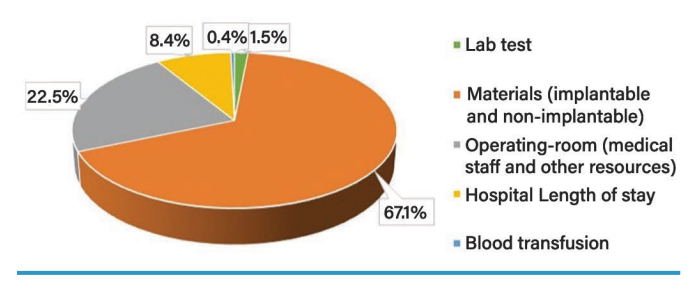
The average length of stay was 6.73 days, and the procedure time was 189.91 minutes. DRGs associated with the arterialization included DRG 110, ‘Major interventions on the cardiovascular system with CC’, and DRG 111, ‘Major interventions on the cardiovascular system without CC’. The average cost per hospitalization to perform pDVA in a single limb was estimated at €19,997 (US $23,279), and the median DRG linked to the hospital at each hospitalization was €13,325 (US $15,512). In total, 10 units of blood transfusions were used to treat the 22 limbs. The average lab testing cost was €302 (US $352) per hospitalization (€115 [US $134] before hospitalization and €187 [US $215] during); the average cost for devices (implantable and non-implantable) was €13,427 (US $15,630). The overhead costs of the operating room and the health care professionals involved totaled €4504 (US $5243) per procedure. The mean cost per procedure of hospital length of stay was €1682 (US $1958), while the mean cost per limb of blood transfusions was €82 (US $95). None of the patients needed intensive care units but only short intense observation after pDVA. Considering all the cost items listed above, the total average cost for pDVA procedure was estimated equal to €19,997 (US $23,279) (Table 3). The largest portion of the pDVA cost (67.1%) is attributed to materials (implantable and non-implantable), followed by operating room expenses (22.5%) and hospital length of stay (8.4%) (Figure 1). Lab tests and blood transfusions contribute minimally, at 1.5% and 0.4%, respectively (Figure 1).
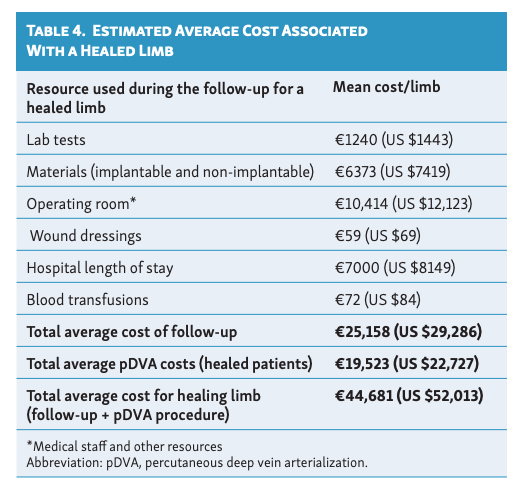
At 12-month follow-up, 45% of limbs were healed and patients were back to walking (10 patients, 10 limbs). During this follow-up, 23% underwent an amputation of the thigh or leg (5 patients, 5 limbs), 3 patients died, and 3 patients were lost to follow-up. All patients underwent minor amputations at various stages. Following arterialization, patients whose limbs were healed at 1 year underwent an average of 2.5 revascularization procedures and 3.6 foot surgery interventions per patient during the follow-up. On average, during the treatment pathway to get to complete healing (considered from the date of pDVA procedure [index date] to 1-year follow-up), the patient underwent 6 hospital admissions, with an average length of stay for admission of about 4.7 days each. The procedures primarily performed during the admissions were percutaneous transluminal angioplasty (alone or in combination with other interventions, about 36% of procedures), cutaneous or dermal graft (about 15%), debridement plus cutaneous or dermal graft (about 15%), and debridement alone (about 10%). Additionally, each patient received an average of 14.6 wound dressings and 0.4 blood transfusions during the follow-up. The average total cost associated with follow-up for a healed limb (from the index date to 1 year of follow-up) was estimated equal to €25,158 (US $29,286); adding to this cost, the average pDVA cost calculated only for healed patients (€19,523 [US $22,727]) and the mean total cost of treatment for a healing limb was roughly €44,681 (US $52,013). Because the mean DRG reimbursement for a healing limb was estimated equal to €63,508 (US $73,930), calculated as the average value of the reimbursement tariffs associated with the procedures performed from the index date to 1 year of follow-up), from a hospital perspective the treatment of a patient until limb healing has a positive margin of €18,827 (US $21,917). The estimated costs to achieve healed limb are presented in Table 4.
Sensitivity analysis
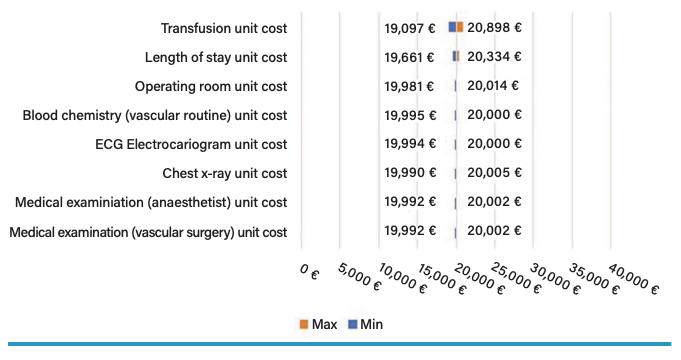
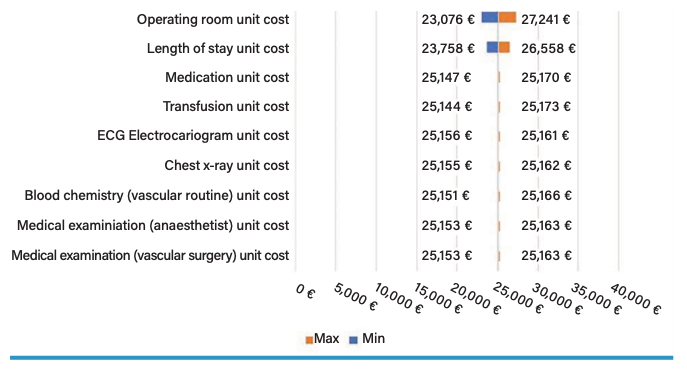
The deterministic sensitivity analysis was conducted to evaluate alternative values for some parameters included in the analysis, especially for those with greater uncertainty, to test their impact on the results. The analysis was conducted by varying the unit costs used for resource evaluation by ±20% (value recommended in the literature in the absence of information on variability).15 The tornado graph shows that the parameter with the greatest impact, although still negligible, on the estimated cost of the pDVA procedure (base-case = €19,997 [US $23,279]) is the unit cost of transfusion; a 20% increase in this cost leads to an increment of the estimated cost for a pDVA procedure of about 4.5% (€20,898 vs €19,997 [US $24,327 vs $23,279] estimated in the base-case) (Figure 2). With regard to the estimated follow-up cost (base-case = €25,158 [US $29,286]), the parameters that have the greatest impact on the cost estimate are the operating room cost and the daily cost of hospital stay; a 20% increase in the operating room cost or in the daily cost of hospital stay leads to an increment of the cost of follow-up for healing limb of about 8.3% (€27,241 vs €25,158 [US $31,711 vs $29,286] estimated in the base-case) and 5.6% (€26,558 vs €25,158 [US $30,916 vs $29,286]) (Figure 3).
Discussion
This study aims to update a previously published analysis on the estimation of HRU and the average costs associated with a single-limb pDVA procedure hospitalization, based on data from a single center in Italy.10 Additionally, this study seeks to estimate the average hospital costs along the treatment pathway leading to complete limb healing. Both the hospital costs related to the pDVA procedure and the follow-up costs for a healed limb were compared to the DRG reimbursement tariffs for each hospital stay in order to assess the efficiency of hospital care delivery. The analysis estimated an average cost per hospitalization to perform pDVA in a single limb equal to €19,997 (US $23,279) and a median DRG tariff for this hospitalization equal to €13,325 (US $15,512). Considering the entire 1-year follow-up to achieve limb healing, the mean total cost of the whole treatment pathway is roughly €44,681 (US $52,013), while the mean DRG reimbursement for healing limb is estimated equal to €63,508 (US $73,930). From a hospital perspective, the treatment of a patient until limb healing has a positive margin of €18,827 (US $21,917).
All patients underwent tension-free surgery, removing at the first treatment just the necrotic tissue and during the following treatments a secondary intention wound healing using dermal substitutes and autologous skin. No patients had amputation followed by direct suture.
A recent systematic review conducted by So et al16 provided a summary of the evidence currently available in terms of efficacy and durability for pDVA. The reviewed studies, with a median follow-up of 12 months, predominantly enrolled patients classified as no-option CLTI. All patients had previously undergone revascularization without achieving positive results or experienced progressive ischemia. Additionally, some of them were considered unsuitable for these procedures.16 Primary outcomes included technical success and major amputation rate. The studies reported a 97% technical success rate, defined as the successful creation of a functional DVA circuit with arterial-to-venous flow. The major amputation rate (defined as lower limb amputation above the level of the ankle joint) associated with pDVA was 21.8%,16 significantly lower than the 40% observed at 6 months post-presentation for patients with CLTI who are unreconstructable or in whom attempts at reconstruction have failed.17 Regarding the secondary outcomes, the studies measured wound healing, achieved in 69.5% of patients at 6 months. The overall complication rate was 13.8%, with postoperative bleeding and infections being the most common issues. Durability remained a challenge, as 37.4% of patients required reinterventions, such as thrombectomy or tributary ligation, to maintain patency. The all-cause mortality rate was 15.7%, compared with 25% at 1 year for patients with CLTI, with most deaths linked to perioperative complications such as pneumonia or myocardial infarction.16
Another systematic review and meta-analysis conducted by Ucci et al2 aimed to determine outcomes of surgical foot vein arterialization (sFVA) and percutaneous FVA (pFVA) at 6 and 12 months post-procedure. The studies included in the review and meta-analysis demonstrated that the pooled limb salvage rates at 6 and 12 months were 78.1% and 74.1% for the sFVA group and 81.7% and 78.6% for the pFVA group, respectively.2 Wound healing rates were not reported for the sFVA group. In the pFVA group, the pooled wound healing rates were 48.1% at 6 months and 64.5% at 12 months.2 Powell et al9 instead compared transcatheter arterialization of deep veins (TADV) with standard of care in patients with CLTI through a propensity-matched analysis. The primary endpoint was 6-month AFS. The study showed that TADV significantly improved 6-month AFS (66.1% vs 39.1%), with a 29% absolute and 45% relative event rate reduction.9 Despite the fact that available studies in the literature are limited in size and follow-up, these studies concluded that pDVA represents a promising therapy for patients with no-option CLTI.
Major amputation has the largest impact on the total patient treatment costs, followed by the costs of rehabilitation and materials. Recent studies conducted in Europe have attempted to capture the costs associated with patients experiencing CLTI who undergo major amputation, especially in the post-amputation phase in terms of rehabilitation. Costs associated with major amputations include services such as home health aides and impacts on family dynamics and workplace productivity, as well as long-term health care expenses.9 The cost-effectiveness analysis conducted by Vadia et al18 in patients with early-stage CLTI from the German payer perspective estimated a cost for amputation procedures in early-stage CLTI equal to €11,585 (US $13,486). This cost was calculated using reimbursement tariffs of 3 DRGs corresponding to lower limb amputation. Additionally, rehabilitation costs for inpatient disease-related rehabilitation were estimated at €3202 (US $3727), based on the German rehabilitation fund report for 2019.18 Another cost-effectiveness analysis conducted by Wakkie et al19 in patients with CLTI and infrapopliteal lesions based on data coming from a single health care insurance company in the Netherlands estimated a cost for a major amputation equal to €16,000 (US $18,626). In terms of rehabilitation costs, the study estimated a cost per patient equal to €15,750 (US $18,335) in the first year following amputation, €7375 (US $8585) in the second year, and €3600 (US $4191) in the third year.19 These expenses cover a range of services, including specialized medical rehabilitation for lower limb amputation, geriatric rehabilitation, home care, nursing aides, and paramedical services such as physical and occupational therapy.20
Finally, a study conducted by Pietzsch et al20 aimed to perform an exploratory cost-effectiveness analysis comparing pDVA to conventional “status quo” treatments within the United States health care system. Among the cost categories analyzed, estimates were also provided for patients undergoing amputation and subsequent rehabilitation. Specifically, the cost of amputation was approximately US $29,847 (€25,640), while post-amputation rehabilitation was estimated at around US $16,418 (€14,104).20 The cost of a prosthesis following amputation was estimated at US $13,627 (€11,706), with an additional annual maintenance cost of US $1022 (€878).20
Study Limitations
The main limitation of this study is the generalizability of the results because we used data mainly coming from a single hospital center. Furthermore, an additional factor contributing to the limited generalizability of the results is that the assessment of economic sustainability is based exclusively on healed limbs, which may exhibit a different pattern of resource utilization compared to unsuccessful cases. Costs were not reported for patients who underwent amputation, as this subgroup is much smaller than the cohort of patients who achieved wound healing and, of primary relevance, the follow-up durations are not directly comparable (the amputation occurred at different follow-up time points). Additionally, multiple data sources were used for costing, some of which enhanced the generalizability of the estimates (eg, national tariff for outpatient service) whereas others, conversely, constrained it (referring to the single center from which the data for this study were obtained). Real-world estimates provided about the procedure duration (in minutes), number of wound dressings, length of stay, and the number of blood units transfused refer to a single hospital center from which the data for this analysis were sourced and processed. Nonetheless, these estimates are not affected by selection bias, and thus not by the exclusion of more complex patients, since patients were enrolled consecutively as they presented. Regarding unit costs used for the analysis, the majority were sourced from the national tariff for outpatient service or from the literature (unit costs of preadmission visits or tests, wound dressings, operating room, hospital stay, and transfusions), while costs associated with laboratory tests and materials used during the procedure were obtained directly from the single center’s data. These aspects must be considered in the interpretation of these study findings, especially in terms of generalization of the results, because these costs vary depending on the different hospitals and countries. Reimbursement tariffs for inpatient care also vary between regions in the national context; therefore, this variability should be considered when comparing the estimated procedure cost with the corresponding reimbursement tariff. Finally, home care cost was not considered in the follow-up cost estimates due to lack of information. Nonetheless, this cost-analysis analysis represents an attempt to provide an estimate of costs incurred by hospital facilities for the pDVA procedure and the management of patients with CLTI using real-world data; as a result, the analysis could assist decision-makers in gaining a clearer understanding of potential economic value, in addition to clinical benefits, of the pDVA and healing process. Appropriate reimbursement policies should be established to ensure that eligible patients have access to this potentially limb-saving treatment. It would be interesting to assess the cost incurred by the Italian National Health Service for patients who undergo amputation to compare them with the estimates obtained in this study. It should be noted that the estimated costs could be slightly overestimated, as the cost of length of stay includes fixed costs and costs associated with all resources on average used during the patient’s admission; therefore, it also includes the cost of operating room use and medical staff involved in each single procedure.
Finally, the surgical procedure would involve lower material costs against the endovascular procedure. However, regardless of the costs, the reason for performing the procedure endovascularly is that the patients are frail, and therefore the least invasive approach possible is preferred.
Conclusions
pDVA is an expensive procedure and costs are mainly driven by materials used during the technique. This exploratory analysis based on data coming from a single-center study shows that completing the full treatment pathway up to patient healing appears to be economically sustainable from the hospital’s perspective. However, these findings should be interpreted with caution given the small sample size and the preliminary nature of the data.
Affiliations and Disclosures
Bruno Migliara, MD, PhD, and Giovanni Feriani, MD, are from the Vascular and Endovascular Unit, Pederzoli Hospital, Verona, Italy; Daniela Cazzato, PhD, Andrea Marcellusi, PhD, and Chiara Bini, MSc, are from the Centre for Economics and International Studies-Economic Evaluation and Health Technology Assessment, Faculty of Economics, University of Rome “Tor Vergata”, Rome, Italy; Cristian Nicoletti, MD, is from the Diabetic Foot Surgery Unit, Pederzoli Hospital, Verona, Italy; and Nicola Raschellà is from the Management Control Unit, Pederzoli Hospital, Verona, Italy.
Dr Migliara received a grant from W. L. Gore; all other authors report no financial relationships or conflicts of interest regarding the content herein.
This study was initiated and funded by W. L. Gore.
Manuscript accepted April 16, 2026.
Address for correspondence: Chiara Bini, MSc, Centre for Economics and International Studies-Economic Evaluation and Health Technology Assessment, Faculty of Economics, University of Rome “Tor Vergata”, via Columbia 2, 00133 Rome, Italy. Email: chiara.stat@gmail.com
References
1. Conte MS, Bradbury AW, Kolh P, et al; GVG Writing Group for the Joint Guidelines of the Society for Vascular Surgery (SVS), European Society for Vascular Surgery (ESVS), and World Federation of Vascular Societies (WFVS). Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1):S1-S109.e33. doi:10.1016/j.ejvs.2019.05.006
2. Ucci A, Perini P, Freyrie A, et al. Endovascular and surgical venous arterialization for no-option patients with chronic limb-threatening ischemia: a systematic review and meta-analysis. J Endovasc Ther. 2025;32(5):1301-1316. doi:10.1177/15266028231210220
3. Nativel M, Potier L, Alexandre L, et al. Lower extremity arterial disease in patients with diabetes: a contemporary narrative review. Cardiovasc Diabetol. 2018;17(1):138. doi:10.1186/s12933-018-0781-1
4. Colella R, Zanetti C, De Mola A, et al. Nursing’s role in prevention interventions and therapeutic education for patients with critical limb-threatening ischemia: a scoping review protocol. International Journal of Wound Research. 2025;1(1):47-52. doi:10.64115/ijwr-2025-6
5. Ventoruzzo G, Mazzitelli G, Ruzzi U, Liistro F, Scatena A, Martelli E. Limb salvage and survival in chronic limb-threatening ischemia: the need for a fast-track team-based approach. J Clin Med. 2023;12(18):6081. doi:10.3390/jcm12186081
6. Berchiolli R, Bertagna G, Adami D, Canovaro F, Torri L, Troisi N. Chronic limb-threatening ischemia and the need for revascularization. J Clin Med. 2023;12(7):2682. doi:10.3390/jcm12072682
7. Migliara B. Treatment of no-option CLI patients. J Vasc Endovasc Ther. 2018;3:15. doi:10.21767/2573-4482.18.03.15
8. Sprengers RW, Teraa M, Moll FL, de Wit GA, van der Graaf Y, Verhaar MC; JUVENTAS Study Group; SMART Study Group. Quality of life in patients with no-option critical limb ischemia underlines the need for new effective treatment. J Vasc Surg. 2010;52(4):843-849, 849.e1. doi:10.1016/j.jvs.2010.04.057
9. Powell RJ, Mullin CM, Clair DG, Shishehbor MH, Dua A. Comparison of transcatheter arterialization of deep veins to standard of care in patients with no-option chronic limb threatening ischemia. Ann Vasc Surg. 2024;99:50-57. doi:10.1016/j.avsg.2023.08.010
10. ISPOR Europe 2022. Direct cost of percutaneous Deep Vein Arterialization (pDVA) in an Italian Center. Abstract #118379. November 2022. Accessed December 20, 2024. Available at: https://www.ispor.org/docs/default-source/euro2022/di-stasi-f-poster-ispor-22118379-pdf.pdf?sfvrsn=2679bc7b_0
11. Migliara B, Feriani G, Mirandola M, Griso A, Cappellari TF, Nicoletti C. Percutaneous deep venous arterialization using an IVUS-guided technique in no-option patients with chronic limb-threatening ischemia: 24-month results. Cardiovasc Intervent Radiol. 2024;47(12):1727-1736. doi:10.1007/s00270-024-03828-4
12. Gazzetta Ufficiale. Ministero della Salute. Definizione delle tariffe relative all’assistenza specialistica ambulatoriale e protesica. November 25, 2024. Accessed October 13, 2025. Available at: https://www.gazzettaufficiale.it/atto/serie_generale/caricaDettaglioAtto/originario?atto.dataPubblicazioneGazzetta=2024-12-27&atto.codiceRedazionale=24A06929&elenco30giorni=true
13. Vertuani S, Nilsson J, Borgman B, et al. A cost-effectiveness analysis of minimally invasive versus open surgery techniques for lumbar spinal fusion in Italy and the United Kingdom. Value Health. 2015;18(6):810-816. doi:10.1016/j.jval.2015.05.002.
14. Beverina I, Razionale G, Ranzini M, Aloni A, Finazzi S, Brando B. Early intravenous iron administration in the emergency department reduces red blood cell unit transfusion, hospitalisation, re-transfusion, length of stay and costs. Blood Transfus. 2020;18(2):106-116. doi:10.2450/2019.0248-19
15. Gray AM, Clarke PM, Wolstenholme J, Wordsworth S. Applied Methods of Cost-effectiveness Analysis in Healthcare. Vol 3. Oxford University Press; 2010.
16. So SE, Chan YC, Cheng SW., Efficacy and durability of percutaneous deep vein arterialization: a systematic review. Ann Vasc Surg. 2024;105:89-98. doi:10.1016/j.avsg.2024.01.008
17. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FGR; TASC II Working Group. Inter-society consensus for the management of peripheral arterial disease (TASC II). J Vasc Surg. 2007;45 Suppl S:S5-S67. doi:10.1016/j.jvs.2006.12.037
18. Vadia R, Malyar N, Stargardt T. Cost-utility analysis of early versus delayed endovascular intervention in critical limb-threatening ischemia patients with rest pain. J Vasc Surg. 2023;77(1):299-308.e2. doi:10.1016/j.jvs.2022.07.007
19. Wakkie T, Konjin LCD, van Herpen NPC, et al. Cost-effectiveness of drug-eluting stents for infrapopliteal lesions in patients with critical limb ischemia: the PADI trial. Cardiovasc Intervent Radiol. 2020;43(3):376-381. doi:10.1007/s00270-019-02385-5
20. Pietzsch JB, Ederhof M, Geisler BP, Schneider PA. Cost-effectiveness of percutaneous deep vein arterialization for patients with no-option chronic limb-threatening ischemia: an exploratory analysis based on the PROMISE I study. J Crit Limb Ischem. 2021;1(4):E148-E157.