Controlled Antegrade and Retrograde Tracking (CART) Technique Via Epicardial Collaterals: Feasible and Safe
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00039. Epub April 21, 2026.
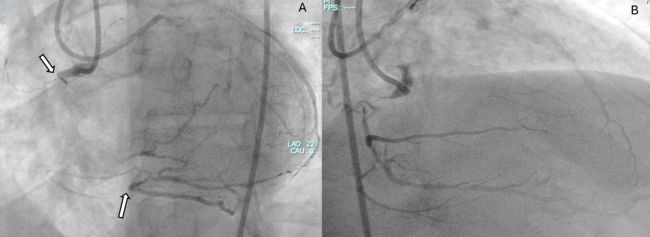
A 59-year-old man with exertional angina and coronary angiography showing chronic total occlusion (CTO) of the right coronary artery (RCA) with collateral filling from the left anterior descending artery (LAD) (Figure 1). Dual injection revealed an ambiguous proximal cap, a very long occlusion, and the distal cap at the bifurcation (Video 1).
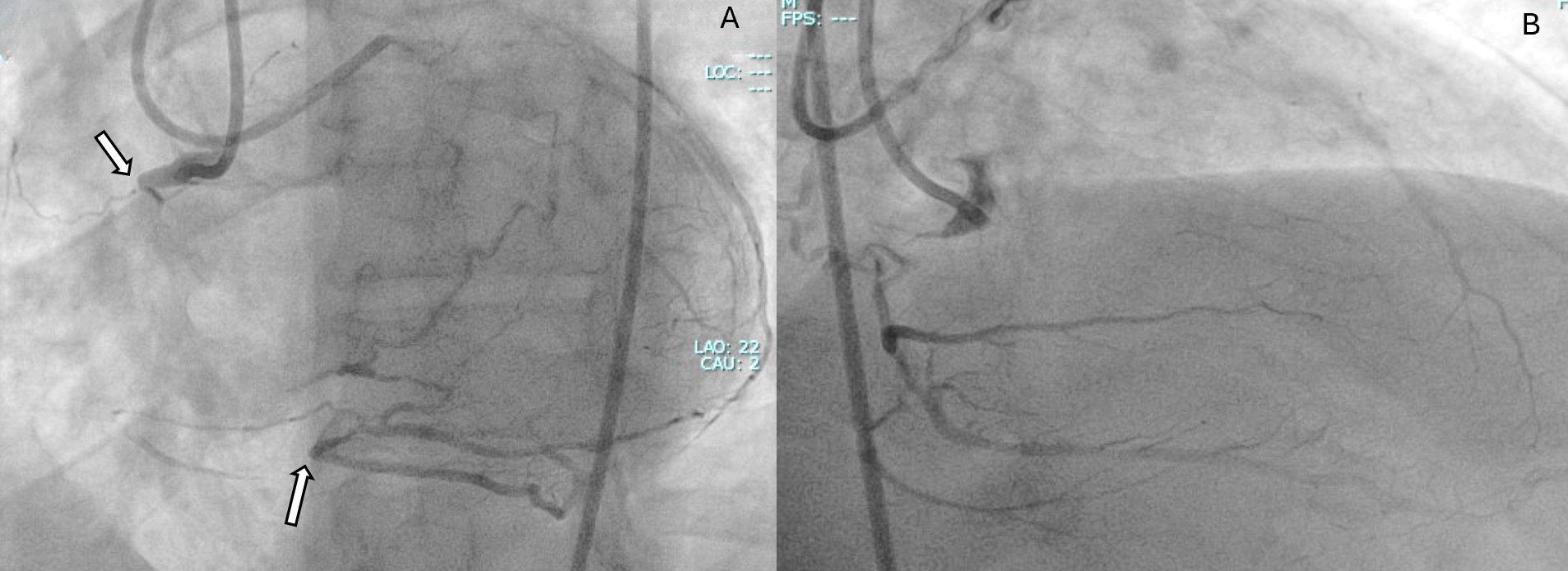
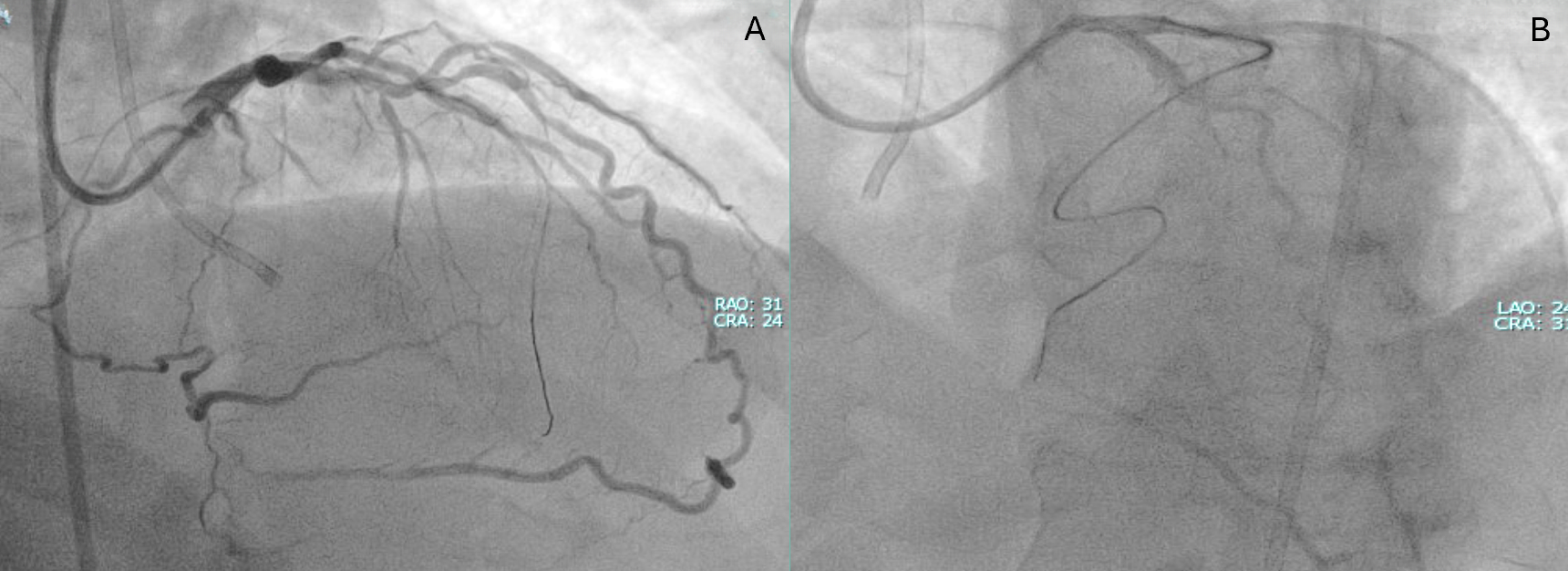
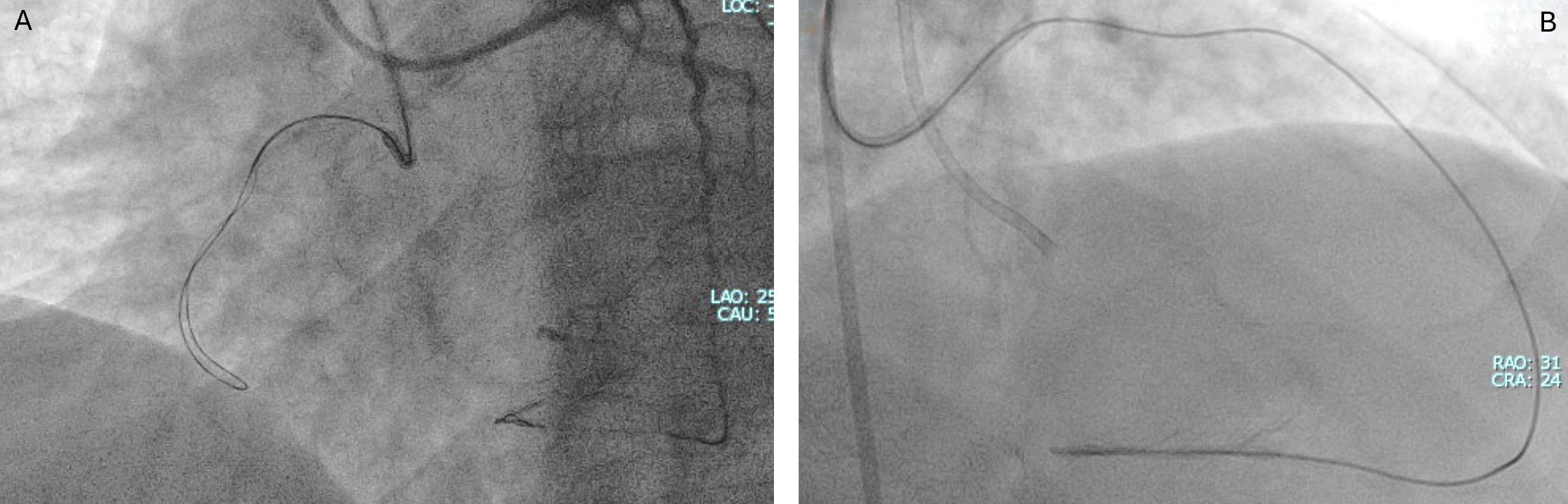
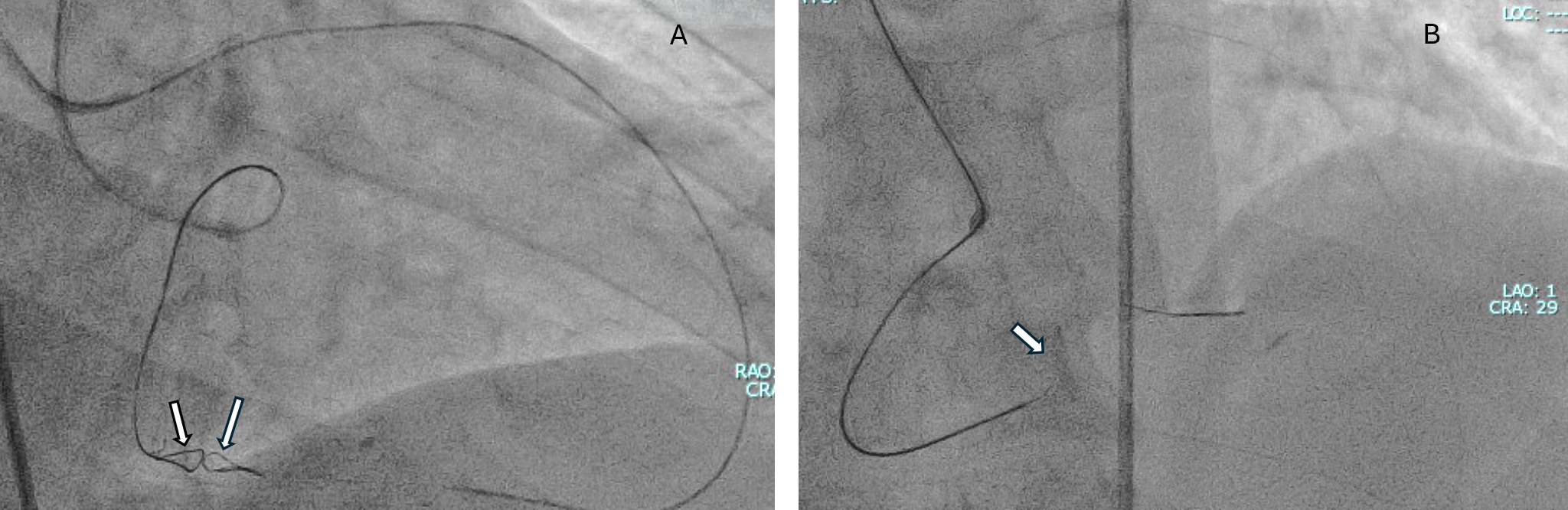
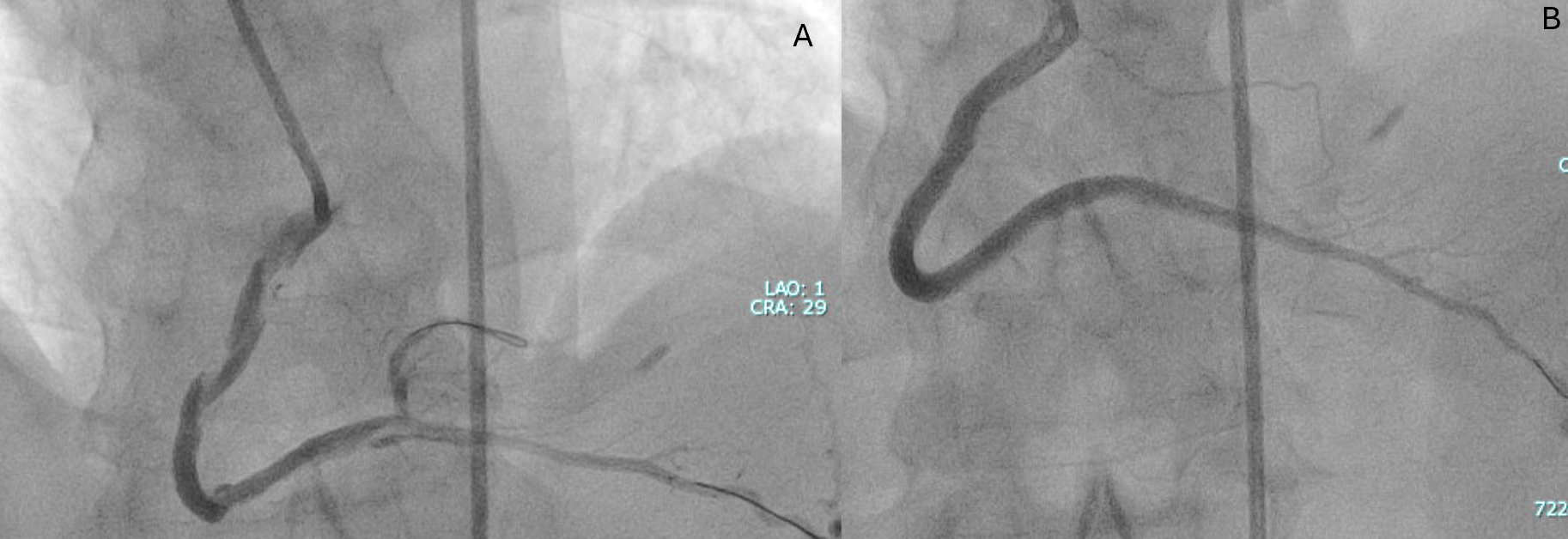
A primary retrograde strategy was selected but septal collateral wiring was unsuccessful. Epicardial collaterals from the LAD were subsequently crossed (Figure 2, Video 2); however, a retrograde wire (Confianza Pro 12; ASAHI INTECC) failed to puncture the distal cap. Antegrade wire (Gladius MG; ASAHI INTEC) knuckle was used until just before it reached the distal cap (Figure 3, Videos 3 and 4). A 3.0 x 20-mm TREK balloon (Abbott) was delivered retrogradely through the epicardial collateral and inflated at the bifurcation (Video 5). Next, an antegrade wire (Gladius EX; ASAHI INTECC) was delivered into the distal true lumen of the posterior descending artery (Figure 4, Video 6). The RCA was successfully stented with an XIENCE Pro drug-eluting stent (Abbott), with restoration of Thrombolysis in Myocardial Infarction 3 flow (Figure 5, Video 7).
Epicardial collateral manipulation carries a recognized risk of perforation and tamponade. In this case, the Controlled Antegrade and Retrograde Tracking (CART) technique via epicardial channel served as a definitive bailout strategy after failure of septal retrograde and reverse CART techniques, enabling successful recanalization. This case shows that, through suitable epicardial collaterals, CART is feasible and can be used for a successful CTO-PCI outcome.
Affiliations and Disclosures
Tarek Abdeldayem, MD1; Mustafa Tigen, MD2; Omer Gogtekin, MD3; Mohaned Egred, BSc (Hons), MB, ChB, MD, FRCP, FESC1,4
From the 1Cardiothoracic Centre, Freeman Hospital, Newcastle upon Tyne, United Kingdom; 2Marmara University, School of Medicine, Department of Cardiology, Istanbul, Turkey; 3Memorial Hospital, Istanbul, Turkey; 4School of Medicine, University of Sunderland, Sunderland.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: Consent was obtained from the patient for the procedure and all that followed.
Address for correspondence: Mohaned Egred, BSc (Hons), MB, ChB, MD, FRCP, FESC, Freeman Hospital, Newcastle upon Tyne NE7 7DN, United Kingdom. Email: m.egred@nhs.net; X: @mohanedegred