Optical Coherence Tomography Features in Coronary Vasculitis: A Takayasu’s Disease Manifestation
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00091. Epub April 17, 2026.
The etiological diversity of coronary artery disease (CAD) sometimes exceeds the classical risk factors. Intracoronary imaging combined with physiological assessment allows for a more personalized treatment.
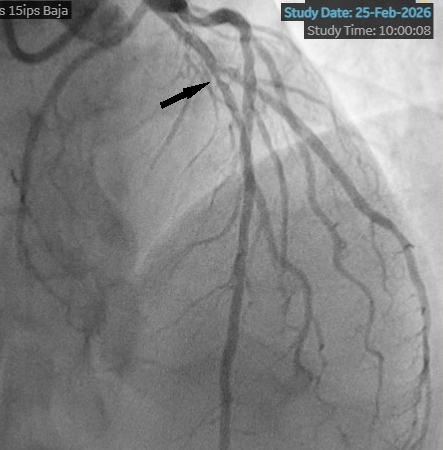
We present the case of a 53-year-old man with a history of Takayasu arteritis, Crohn’s disease, and HLA-B27-negative spondyloarthritis who presented with unstable angina, prompting coronary angiography. Angiography revealed a long, angiographically intermediate lesion in the left anterior descending artery (Figure 1).
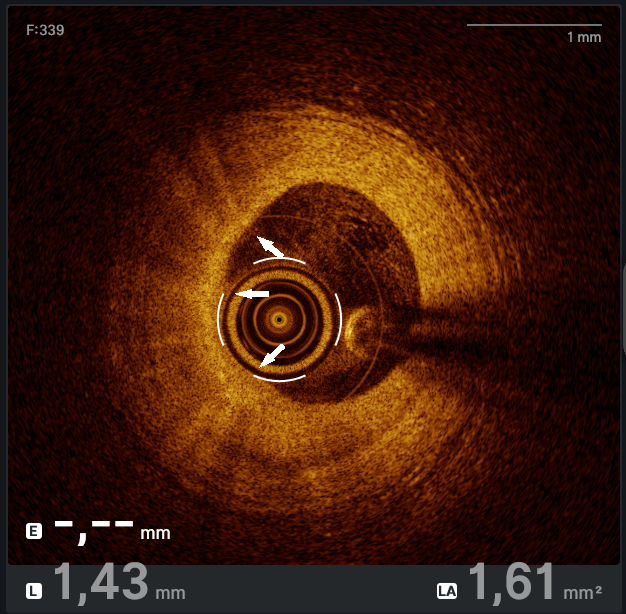
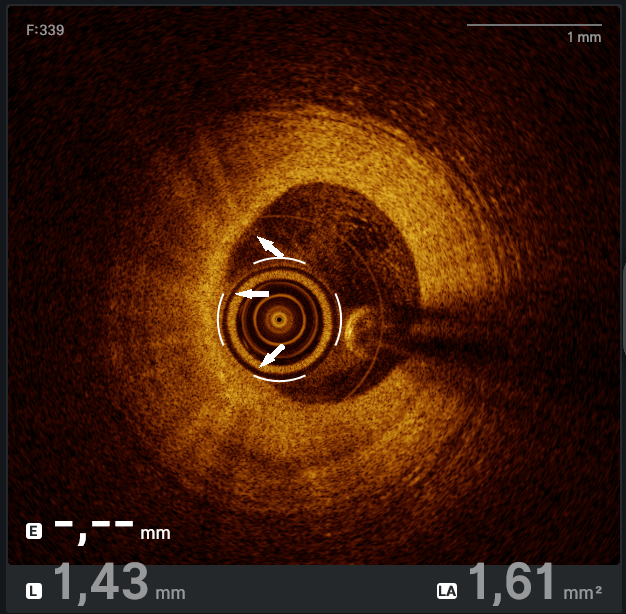
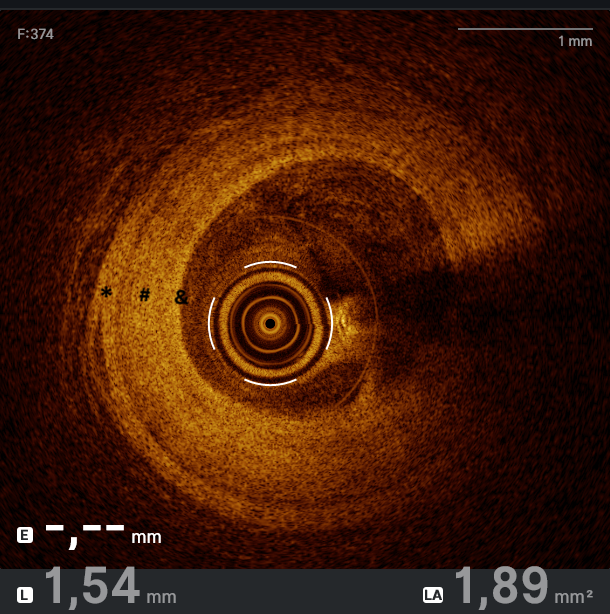
Optical coherence tomography (OCT) assessment confirmed the severity of the stenosis by area and demonstrated both punctate hyper-refringent lesions in the intima (oedema and inflammatory cells) without posterior shadowing, compatible with the active phase of vasculitis (Figure 2), as well as chronic-phase features showing intimal fibroproliferation and medial layer thickening (Figure 3). This makes up a homogeneous and diffuse thickening pattern consistent with coronary vasculitis (Video).
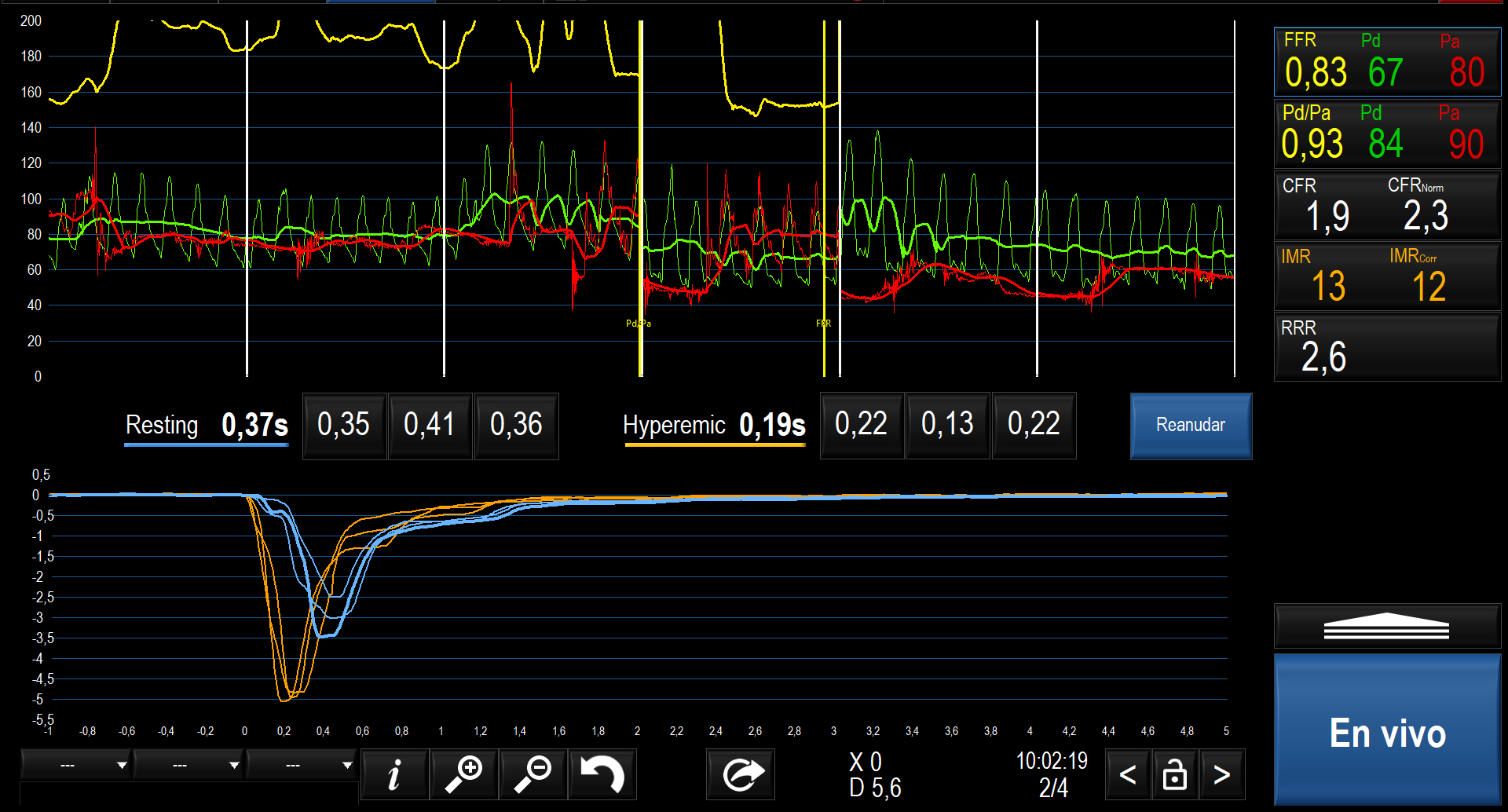
Microvascular function testing was performed and found to be normal (index of microcirculatory resistance: 13; coronary flow reserve: 2.3) (Figure 4), demonstrating that large-vessel involvement predominates in this condition, while the microcirculation remains preserved, even during the active disease phase.
Given the lesion characteristics and the patient’s high inflammatory burden and considering the documented risk of early stent failure in patients with Takayasu arteritis, percutaneous transluminal angioplasty with a drug-coated balloon (DCB) was performed. Functional indices normalized after the procedure (pre-angioplasty fraction flow reserve [FFR]: 0.76; post-angioplasty FFR: 0.98).
The standardization of intracoronary imaging techniques plays a crucial role in the thorough diagnosis of CAD. Moreover, the increasing use of DCB angioplasty emerges as a viable alternative in patients with high inflammatory burden, such as those with Takayasu arteritis, Kawasaki disease, HIV-associated vasculopathy, or cardiac graft vasculopathy.
Affiliations and Disclosures
Nicolás del Cuerpo Salinas, MD; Eduardo Arroyo Úcar, MD, PhD; Ignacio Alfaro Paniagua, MD; Marta Monteagudo Viana, MD, PhD; María Araceli Frutos García, MD
From the Cardiology Department, San Juan de Alicante University Hospital, Alicante, Spain.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention described in the manuscript and to the publication, including any and all images.
Address for correspondence: Nicolás del Cuerpo Salinas, MD, San Juan de Alicante University Hospital, Alicante, Spain. Email: Unicolas28@hotmail.com X: @nicodcs28