


Impact of Ultra-High-Pressure OPN NC Balloons in Complex Coronary Interventions: Indications, Safety, and Efficacy
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00071. Epub May 27, 2026.
Abstract
Objectives. The OPN super high-pressure noncompliant (NC) balloon (SIS Medical AG) can safely reach inflation pressures of 45 to 50 atm, offering a valuable option for complex coronary interventions. This study aimed to evaluate its safety and efficacy in a real-world setting.
Methods. The authors conducted an observational, single-center registry including consecutive patients treated with the OPN balloon over 13 years. Procedural indication, safety, and efficacy were assessed using quantitative coronary angiography (QCA). Major adverse cardiovascular events (MACE)—defined as cardiovascular death, myocardial infarction, or target lesion revascularization—were analyzed at 1-year follow-up.
Results. A total of 275 patients (289 lesions) were included. The cohort was highly complex (mean age 70 ± 10 years, 66% multivessel disease, 66% diabetes, 35% in-stent restenosis [ISR]). The main indication was plaque preparation (68%), followed by stent optimization (32%). Procedural success was 95%, with one-third of lesions requiring inflation pressures of greater than or equal to 40 atm. QCA demonstrated a significant increase in minimal lumen diameter (1.31 ± 0.66 mm to 2.13 ± 0.62 mm, P < .001) and a reduction in diameter stenosis (51% to 24%, P < 0.001). Safety outcomes were excellent, with very low complication rates. At 1 year, MACE occurred in 3.8% of patients (stent thrombosis 0.7%). Outcomes were similar between de novo and ISR lesions. Diabetes and chronic kidney disease independently predicted MACE.
Conclusions. In routine clinical practice, the OPN NC balloon demonstrated high efficacy and an excellent safety profile, achieving significant luminal gain at ultra-high pressures. These findings support its role for lesion preparation and stent optimization.
Introduction
The global rise in coronary artery disease (CAD) has led to an increased number of percutaneous coronary interventions (PCI), reflecting its pivotal role in CAD management.1,2 With an aging population, the prevalence of heavily calcified coronary lesions has also grown, affecting approximately one-third of patients undergoing PCI, thereby emphasizing the need for effective and simplified treatment strategies for these complex cases.3,4
Severe calcification poses significant challenges during PCI by increasing vessel stiffness, reducing arterial compliance, and complicating optimal stent deployment.1,3,5 Calcified plaques are associated with higher rates of device failure, including balloon rupture or entrapment, and independently increase the risk of periprocedural major adverse cardiovascular events (MACE) as well as long-term complications such as in-stent restenosis (ISR), stent thrombosis, target lesion revascularization (TLR), myocardial infarction (MI), and mortality.3,4,6
Successful management of these lesions often requires advanced plaque modification techniques and dedicated devices to improve procedural success and minimize adverse outcomes.2,3 Optimizing PCI is critical to achieving favorable outcomes, as achieving a higher stent expansion has been associated with a decrease in target lesion failure (TLF).4 Intravascular imaging (IVI) has become essential in guiding plaque modification and stent optimization to improve clinical outcomes and reduce MACE.2,3,5,7
A wide range of calcium plaque modification techniques has been developed to address these complex lesions.5 Balloon-based approaches include noncompliant (NC) balloons, cutting (CB) balloons, scoring balloons (SB), and OPN NC super high-pressure noncompliant balloons (SIS Medical AG), while atherectomy devices comprise rotational (RA), orbital (OA), and laser-based systems, such as excimer laser coronary atherectomy (ELCA).5,8,9 More recently, intravascular lithotripsy (IVL) has emerged as a novel technique that utilizes acoustic shockwaves delivered via a balloon-based system to fracture calcified plaques, thereby enhancing vessel compliance.5,10
The choice of plaque modification technique depends on lesion complexity, calcium characteristics, operator expertise, and device availability, often requiring a tailored combination of modalities. Despite its availability for over a decade, the OPN NC super high-pressure balloon—a twin-layer balloon capable of inflations up to 55 atm—has not been widely adopted and lacks specific regulatory indications for calcium modification in native coronary disease.3,8,11
Evidence of OPN NC super high-pressure balloon use has been previously published in relatively small case series and registries, with little more than 1000 patients reported overall.9,11-19 Moreover, there is a lack of systematic data using IVI describing the calcium modification effect pre-stent deployment.1,3,5,9 A deeper understanding of its mechanism and clinical impact would inform optimal patient selection and expected outcomes. The aim of this study was to evaluate the indication for the use, safety, and efficacy of the OPN NC balloon in real-world settings.
Methods
The authors analyzed data from an observational, investigator-initiated, single-center registry that included consecutive patients over 13 years (2010-2023) who were treated with the OPN balloon. The indications for use, safety (periprocedural complications and in-hospital major adverse events [MAE]), and efficacy (procedural success and major cardiovascular events [MACE] at 1-year follow-up) were assessed.
Institutionally, all patients undergoing PCI had an in-person visit at 30 days, 6 months, and 1 year per protocol, in which clinical, analytical, and complementary test data were determined. There were no patients with loss of follow-up except for death or transfer to another country/autonomous community and absence of contact telephone number (<1%). All events were evaluated by a committee consisting of 2 interventional cardiologists and 1 clinical cardiologist. The quantitative coronary angiography (QCA) was performed in our local core lab, usually by 2 trained interventional cardiologists.
Informed consent was obtained verbally during the procedure and subsequently in writing from the patient or their legal representative after the procedure. The study was performed in accordance with the Declaration of Helsinki and with Good Clinical Practice guidelines and was approved by the local ethics committee.
The device
The OPN NC super high-pressure balloon is a twin-layer balloon that allows the use of very high-pressure inflations. Although according to the instructions for use the rated burst pressure is at 35 atm, recent studies and daily practice show safety at greater than 40 atm up to 55 atm.15 In order to avoid guidewire entrapment, it is recommended to use guidewires with a short spring coil segment with a hydrophobic coating, such as the Grand Slam or the Miracle family of guidewires (ASAHI INTECC) or BMW (Abbott) and allow adequate deflation time.20
The OPN NC technology has shown promise where other technologies have limitations. It has a low profile that confers high deliverability, ensuring uniform stent expansion and avoiding the “dog-bone effect” over a wide range of pressures without requiring a learning curve, as it is used like other balloon techniques. It also has a low price compared with other modification plaque alternatives.11,15,16
Nevertheless, there are certain limitations related to the double-layer design. It is bulkier and stiffer, making it more difficult to deliver the balloon and recross lesions after inflation.3,11 Also, the risk of coronary perforation is higher especially with predilatation, so a careful sizing and technique is essential to mitigate those risks.3,15 We recommend a decrease of 0.5 mm for predilatation and a 1:1 ratio in postdilatation or ISR.
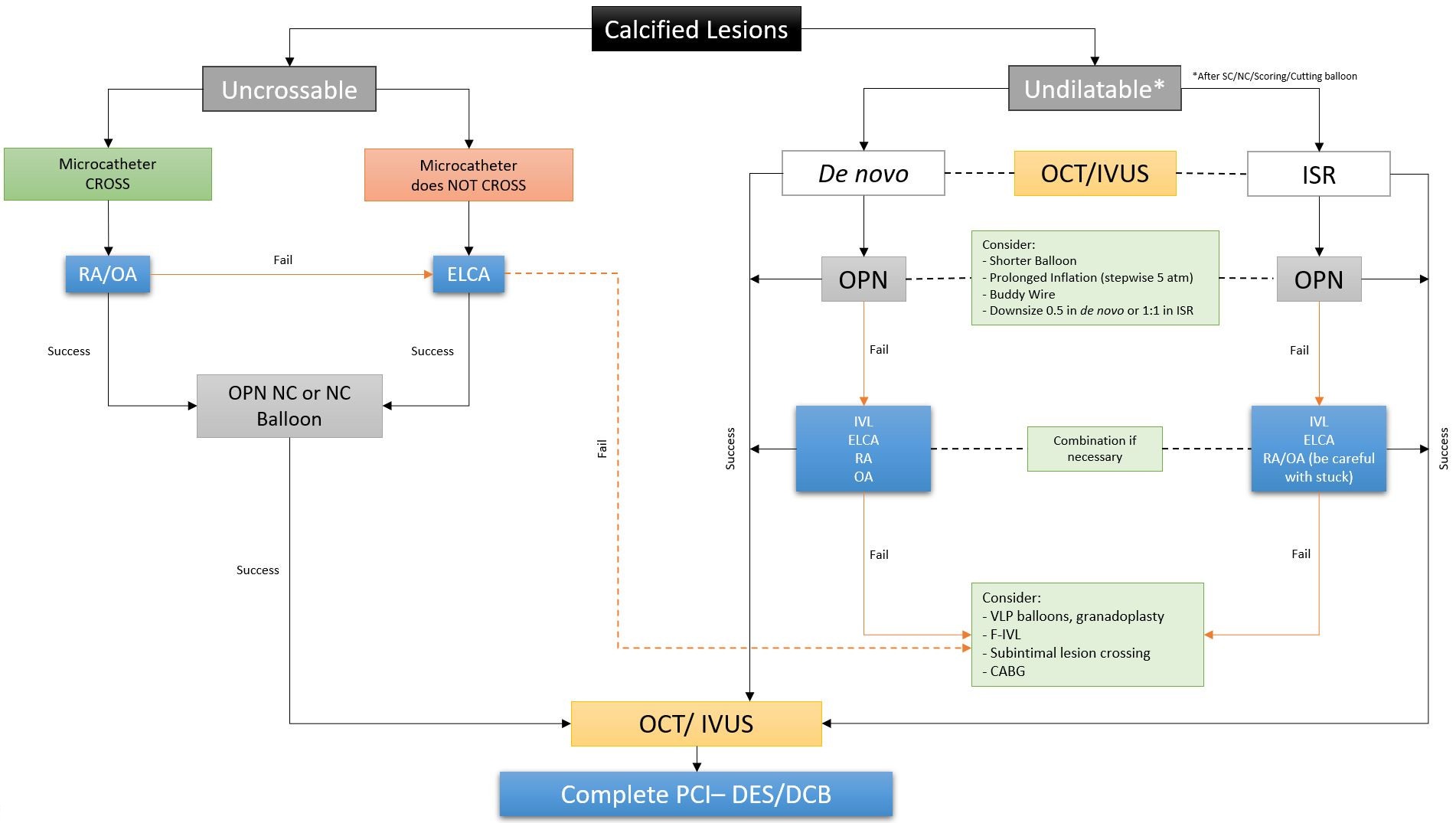
Plaque preparation algorithm
Although it was not mandatory, in our center we followed an institutional progressive algorithm in the approach to this type of calcified complex lesions (Figure 1). This algorithm has been adapted and modified (as this is an observational registry spanning more than a decade) based on the best available evidence to date and the local availability of different plaque modification techniques and/or materials, such as intracoronary imaging techniques. These devices were used in cases in which NC, cutting, or scoring balloons failed to predilate calcified de novo lesions (full balloon expansion in 2 orthogonal fluoroscopic views) or in cases of stent underexpansion assessed by intracoronary imaging and/or stent enhanced technology (StentBoost [Philips Medical System]). It is important to note that our institution is a reference center to which patients with prior suboptimal stents implantations at other centers were sent because of the lack of material availability.
Endpoints
Successful stent implantation was defined as a final residual stenosis of less than 30% by QCA and distal Thrombolysis in Myocardial Infarction 3 flow. Successful plaque preparation was defined as full balloon expansion in 2 orthogonal fluoroscopic views. Clinical success was defined as procedural success and no in-hospital major adverse cardiac events. In-hospital MAE was defined as a composite of death, MI, unplanned revascularization, cardiogenic shock, ventricular arrhythmia, or stroke. Moreover, MACE during follow-up was defined as a composite of death, MI, and unplanned revascularization. QCA to assess luminal gain was performed prior to and post-OPN NC balloon use. According to the study protocol, all patients were clinically followed at 12 months.
Statistical analysis
Continuous variables are described as mean ± standard deviations or as median and interquartile range, as appropriate. The Student's t-test for paired data was used to compare means for each patient. Categorical variables are expressed as counts (percentage) and were compared with the use of Pearson’s chi-square test or Fisher’s exact test, as appropriate. A Cox regression model was designed to search for independent factors related to MACE at follow-up in the entire cohort. For this purpose, variables presenting a P-value of less than 0.1 in the univariate analysis were included. In addition, variables that had been identified in previous studies as prognostic variables were also included in the model. Survival analysis was performed using the Kaplan-Meier method. Hazard ratios (HR) with 95% confidence intervals (CI) were calculated. A P-value of less than 0.05 was considered statistically significant. All statistical analyses were performed using SPSS 25.0 (IBM).
Results
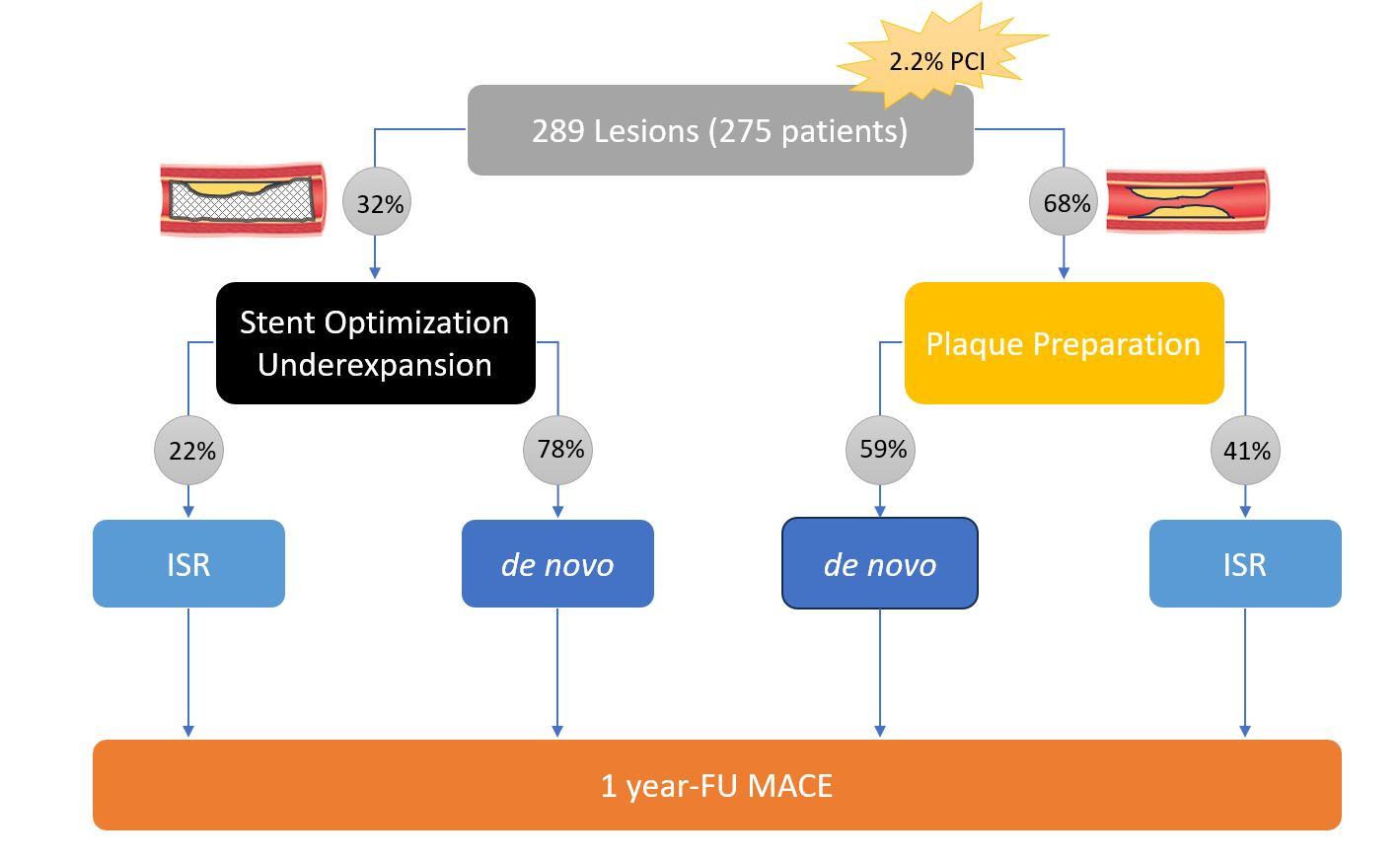
A total of 275 patients with 289 coronary lesions treated with OPN NC balloons were included. From a total of 12 610 PCI performed during the study period, we performed 93 cases (32%) with unexpandable stents and 196 (68%) with plaque modification before stent implantation; 100 (35%) were in ISR cases. Overall, the use of OPN NC balloons accounted for up to 2.2% of PCIs (Figure 2).
Baseline clinical characteristics are summarized in Table 1. Because of their extensive CAD and comorbidities, most patients were considered complex and high-risk intervention (CHIPs). The mean age was 70 ± 9.9 years, and 225 (78%) were male. Multivessel CAD was present in 182 (66%) patients. Cardiovascular risk factors were prevalent, with hypertension observed in 237 (86%), diabetes mellitus in 182 (66%), and a history of smoking in 170 (62%) of the cohort.
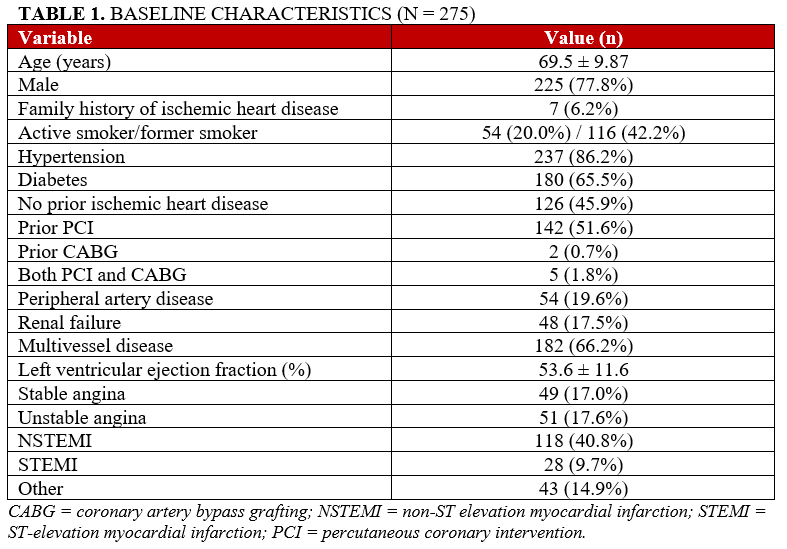
The most frequent clinical presentation was non-ST-elevation myocardial infarction (NSTEMI) in 118 cases (41%), followed by unstable angina in 51 (18%) and stable angina in 49 (17%). ST-elevation myocardial infarction (STEMI) was observed in 28 cases (10%).
Procedural and angiographic characteristics
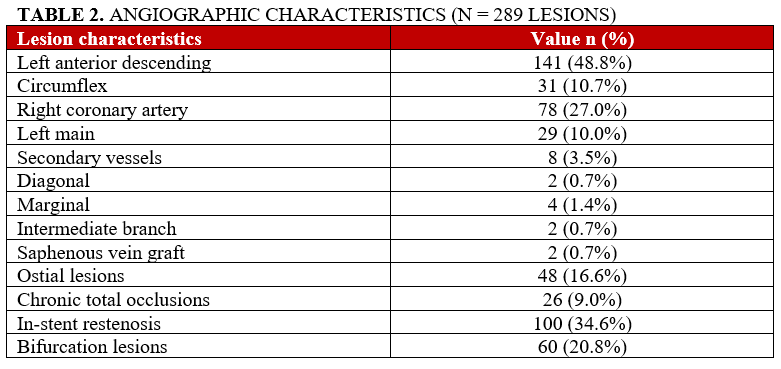
Angiographic and procedural data are detailed in Tables 2 and 3. The most commonly treated vessel was the left anterior descending artery (141[49%]), followed by the right coronary artery (78 [27%]) and the left main coronary artery (29 [10%]). Overall, ISR accounted for 100 (35%) treated lesions; 196 (41%) of these were in the plaque preparation group and 93 (22%) were in the stent optimization group. Bifurcation and ostial lesions were present in 60 (21%) and 48 (17%) cases, respectively. In around 26 cases (9%), a chronic total occlusion (CTO) lesion was treated.
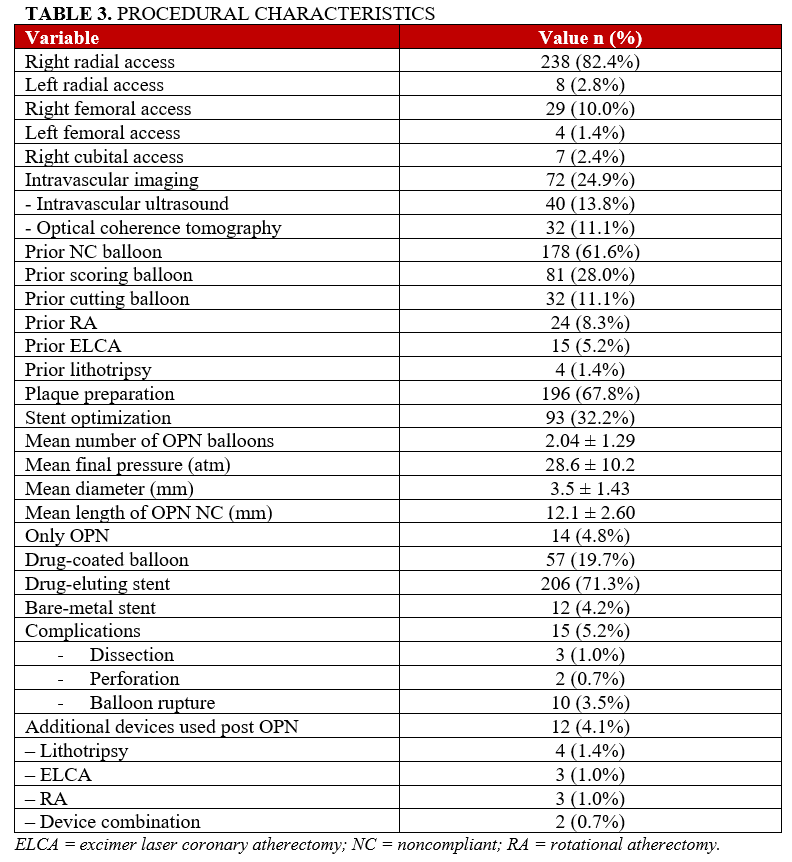
Radial access was used in the majority of procedures (246 [85%]), mostly the right radial artery (238 [82%]). Intracoronary imaging was used in 72 (25%) cases: 40 (14%) intravascular ultrasound and 32 (11%) optical coherence tomography.
The main indication for OPN NC balloon use was plaque modification prior to stent implantation (196 [68%]); the remining cases (93 [32%]) used OPN NC balloons for stent optimization. The use of combined plaque modification tools included 81 (28%) SB, 32 (11%) CB, 24 (8%) RA, 15 (5%) ELCA, and 4 (1.4%) IVL. The OPN device was able to reach the target lesion in all cases.
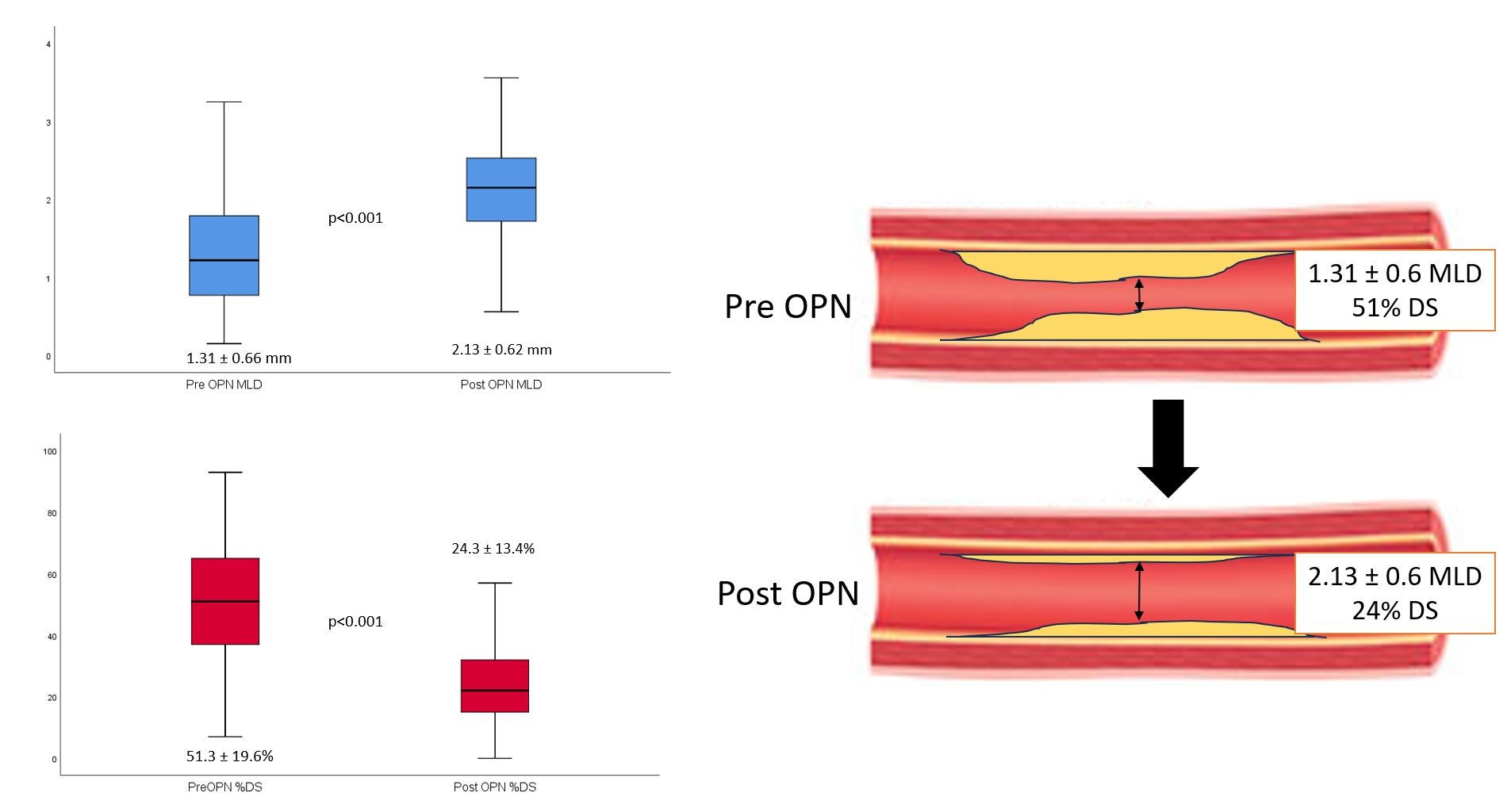
The efficacy in terms of procedural success was 95%. Notably, over one-third of lesions (n = 105) required inflation pressures of greater than or equal to 40 atm. The QCA showed significant improvement in minimal lumen diameter (MLD) (1.31 ± 0.66 mm to 2.13 ± 0.62 mm, P < .001) and decrease in the diameter stenosis (51% to 24%, P < .001) after its use (Figure 3).
The safety was excellent with a very low incidence of periprocedural complications, including 3.5% balloon rupture but without periprocedural coronary perforations. All balloons had pressures of approximately 20 to 30 atm (probably due to penetrated calcium spicules with an optimal plaque preparation in these type of complex lesions). We had only 2 cases (0.7%) of coronary perforation, which were resolved with prolonged balloon inflation and were not related to flow-limiting dissection lesions. There were 3 cases (1%) of flow-limiting dissection, all of which were resolved after stent implantation and were not associated with any periprocedural and in-hospital MAE.
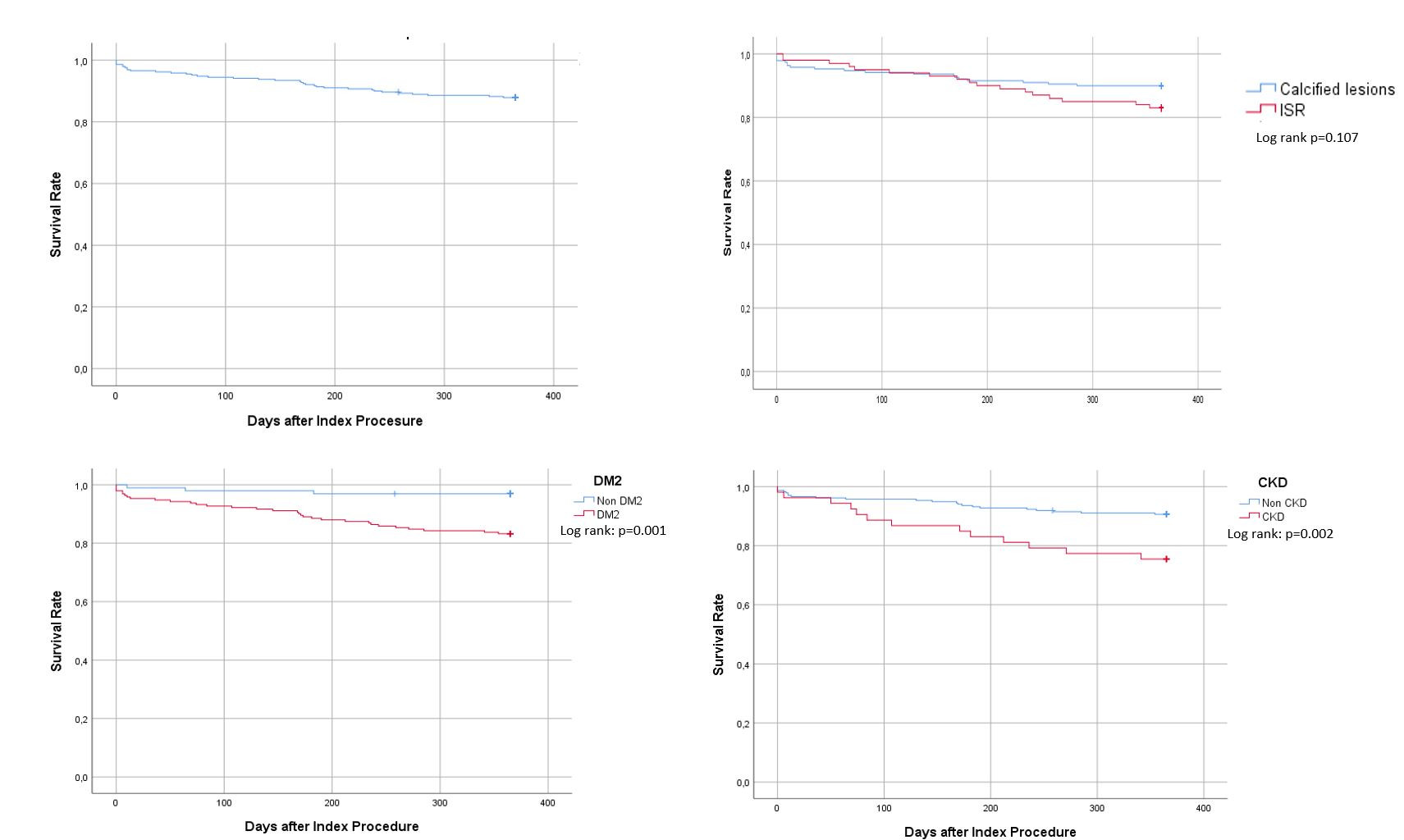
At 1-year follow-up, the rate of MACE was 3.8% for patient-oriented MACE and 3.5% for lesion-oriented MACE, with only 2 cases (0.7%) of stent thrombosis (Table 4). In the univariate analysis and again in the multivariate model including 6 variables, only the presence of CKD (OR: 3.1; 95% CI, 1.5-6.8; P < .05) and type 2 diabetes (OR: 6.3; 95% CI, 1.9-21.1; P < .05) were identified as independent predictors of MACE. The Kaplan-Meier general curves and independent predictors of MACE are presented in Figure 4.
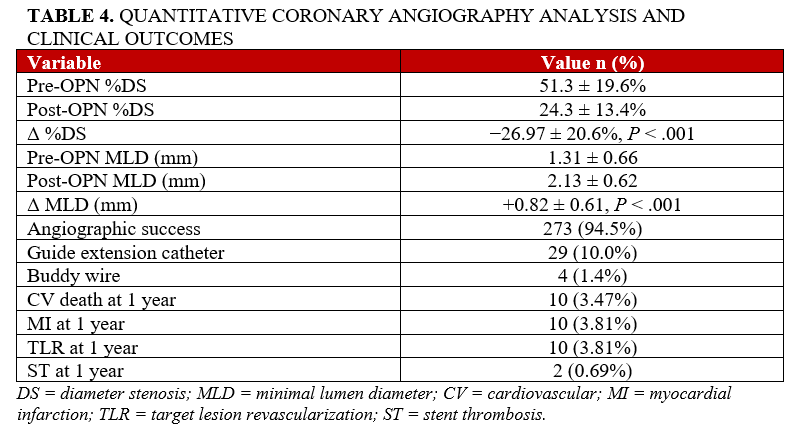
QCA analysis
High-pressure dilatation with OPN NC balloons resulted in a significant acute luminal gain (Figure 3, Table 4). MLD increased from 1.31 ± 0.66 mm to 2.13 ± 0.62 mm (P < .001), with a corresponding reduction in diameter stenosis from 51.3 ± 19.6% to 24.3 ± 13.4% (P < .001). Angiographic success, defined as residual stenosis of less than 30% without major complications, was achieved in 273 lesions (94.5%).
Discussion
The present work includes data from one of the largest registries evaluating the use of the OPN NC balloon in real-world practice. The main findings of the study are (1) in daily clinical practice, the primary use of this device is for plaque preparation (approximately two-thirds of cases), followed by stent optimization (one-third); (2) the safety profile is excellent, with a very low rate of periprocedural complications, in-hospital MAE, and stent thrombosis, even in complex clinical scenarios; and (3) the device demonstrated high efficacy, allowing successful treatment of challenging lesions in a relatively simple, rapid, and cost-effective manner. In addition, we propose a pragmatic algorithm for the management of calcified coronary lesions (Figure 1).
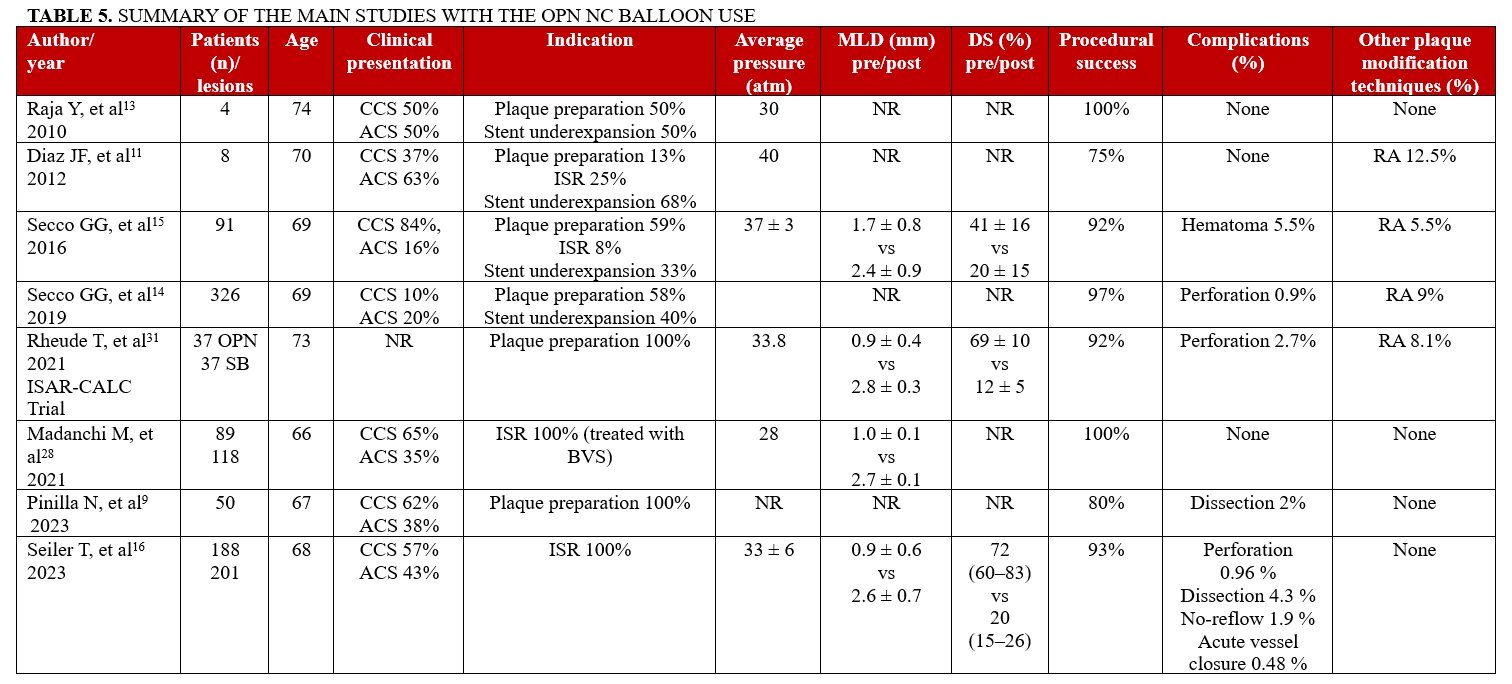
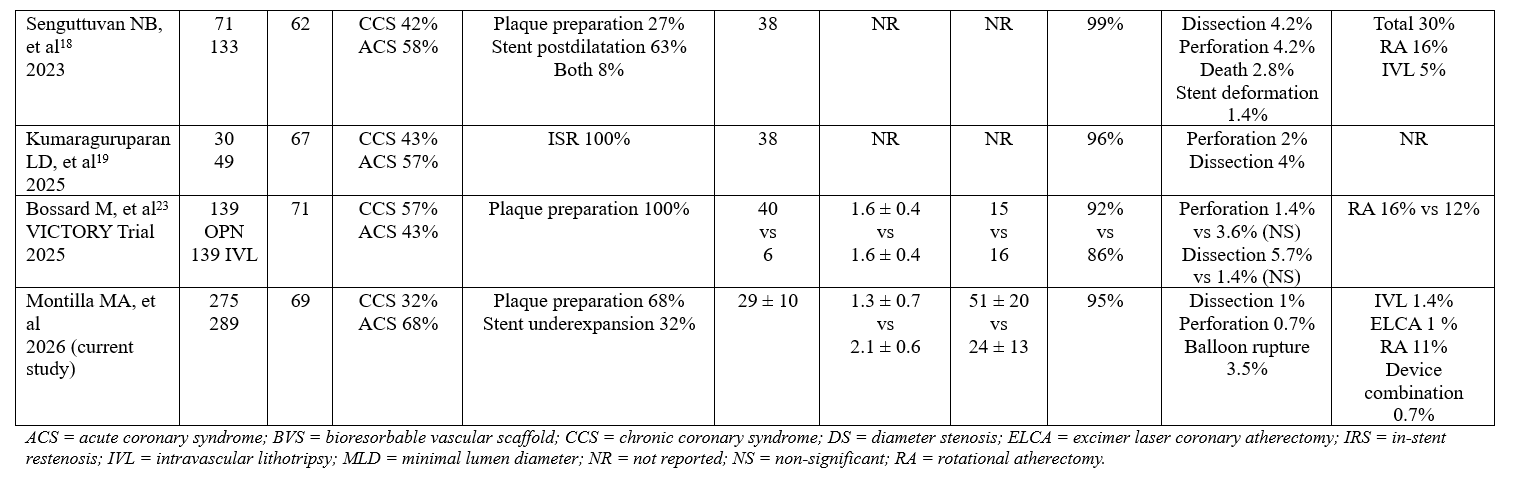
The OPN super high-pressure NC balloon has emerged as a valuable therapeutic tool in the management of complex CAD, particularly in cases of severe calcification and ISR.9,19 Its dual-layer design enables safe inflation at extremely high pressures (up to 45-55 atm), permitting modification of resistant lesions that do not respond to conventional balloon assisted techniques—often without the need for atherectomy, ELCA, or lithotripsy.10,11,15 Nevertheless, evidence regarding safety and efficacy, especially at very high pressures, is still scarce.1,3,5 Table 5 summarizes the current clinical evidence on its use.
Compared with other published series,9,12,16 the present study included older patients, with a higher burden of cardiovascular risk factors and a greater proportion of multivessel and complex lesions, including ostial lesions, bifurcations, and ISR. Compared with previous ones, a distinctive feature of our cohort was the high percentage of patients presenting with acute coronary syndromes (ACS)—a subgroup that carries higher procedural and clinical risk.12
In our real-world registry, the OPN NC balloon demonstrated excellent safety and efficacy, even in a population characterized by high anatomical and clinical complexity, achieving a success rate of 94.5%. This procedural success rate (>90%) has been consistently reported across most of the studies regarding the use of this device12 and is comparable to the largest series published to date.14,15
Complication rates were remarkably low, with only 2 cases (0.7%) of coronary perforation—both successfully managed with prolonged balloon inflation—and approximately 1% of cases with non-significant coronary dissections. This favorable safety profile persisted despite the frequent use of ultra-high pressures and the inclusion of high-risk lesions and patients, aligning with the results from previous studies (Table 5).
In more than one-third of cases, inflation pressures of greater than or equal to 40 atm were required to achieve an adequate lumen area. Even at these extreme pressures, balloon rupture occurred in only 3.5% of procedures (mostly around 20 atm, likely due to focal calcified flakes), with no increase in major complications. These data support prior findings by Secco et al and other large registries, which stratified results according to final inflation pressure up to 50 atm.11,14,15
The growing use of IVL may, in part, be attributed to its novelty and the perception of plaque modification at low nominal pressure (4-6 atm). However, the actual energy delivered corresponds to mechanical effects comparable to those achieved with OPN inflation at 50 atm in coronary arteries (and up to 100 atm in peripheral arteries). Moreover, IVL devices have a poorer crossing profile, are approximately 4 times more expensive, take longer to apply, and present a higher rupture rate (6%-10%) in heavily calcified lesions.21,22 Recently, the VICTORY randomized clinical trial directly compared OPN with IVL for de novo severely calcified coronary lesions under OCT guidance. OCT-guided PCI with lesion preparation using the OPN NC balloon proved non-inferiority to IVL in terms of stent expansion, with a similar safety profile, lower cost, and faster procedural use.23 A small recent cadaver study compared vascular damage in the preparation of calcified plaques with IVL, CB, and OPN NC, with the OPN demonstrating usefulness especially when the calcium arc was greater than 180º.24 In the ShortCUT study, there were no differences in stent expansion, calcium fractures, strategy success, intraprocedural adverse events, or MACE out to 30 days between use of IVL or CB for the treatment of calcified lesions; however, the OPN NC balloon was significantly less costly.25
The impact of the OPN NC balloon on luminal gain was confirmed by QCA, which demonstrated a significant increase in MLD (1.31 ± 0.66 mm to 2.13 ± 0.62 mm) and a corresponding reduction in diameter stenosis (51.3% to 24.3%) (P < .001). These improvements are clinically relevant, as suboptimal stent expansion is a well-established predictor of ISR, stent thrombosis, and TLF.1,26,27
The OPN NC balloon also showed strong performance in ISR—a particularly challenging setting—representing 34.6% of the treated lesions. In this context, luminal gain and optimal stent expansion are key predictors of outcomes after PCI. OPN facilitated adequate expansion even after the failure of conventional NC, SB, or CB (previously used in 62.6%, 28%, and 11.1% of cases, respectively). Neointimal atherosclerosis remains a limitation to maximal luminal gain.17 Several studies have evaluated the efficacy of the OPN NC balloon in ISR, showing significant acute luminal gain with low complication rates.16,19,28 Our study evaluated this device in 100 patients with good results: success was not achieved in 6 patients and 2 cases of non-severe coronary perforation were reported. Notably, several of the cases that were unsuccessful (despite the combined use of all complex plaque modification techniques) involved ISRs on multiple layers of underexpanded stents. This emphasizes the great importance of optimizing stent outcomes with IVI during the first implant and, if the necessary material is unavailable, referring patients to referral centers earlier, before stenting.
Stent underexpansion is another scenario where the OPN NC balloon represents a promising alternative. It is a well-known predictor of adverse events and MACE.29,30 In our registry, the OPN balloon was used for stent optimization in 32.2% of cases, with only 3 non-fatal complications reported. At 1-year follow-up, rates of TLR (3.8%), MI (3.8%), and stent thrombosis (0.7%) were low, comparable to or better than previously reported ISR outcomes.1,3 Interestingly, no differences in adverse events were observed according to lesion characteristics. Classic predictors of MACE such as diameter stenosis reduction or MLD improvement were not significantly associated with outcomes, likely because of the overall low MACE incidence during follow-up.
Although IVI was used in only 25.9% of procedures, angiographic and QCA data suggest that OPN achieved effective lesion modification—aided by the motion-corrected StentBoost X-ray technique)—allowing for the evaluation of stent expansion and apposition, in most cases. As highlighted by Ng et al, achieving an adequate minimal stent area (MSA)—particularly in ISR or underexpansion—is critical to avoid adverse events.1 In future clinical practice, systematic use of IVUS or OCT could improve procedure strategy and help achieve better plaque modification and stent optimization,9,31 as recommended in current guidelines.7,32
Uncrossable lesions represent one of the main limitations to balloon techniques, including OPN, and delivery challenges usually require the use of other techniques. Due to availability, RA is the most used technique to achieve balloon advancement in most cath labs; its use in these complex coronary scenarios could account for around 10% to 15% of cases (Table 5). Moreover, as occurred in a small subgroup of lesions (4.1%), adjunctive plaque modification techniques such as RA, ELCA, or IVL were required even after use of the OPN NC balloon.8,33
Secco et al’s registry showed a higher need for RA in the group treated with lower pressure.14 Our data showed similar need for prior modification techniques (especially RA) because of uncrossability. These results support a stepwise approach, where OPN serves as a high-performance intermediate strategy that may prevent the need for more invasive debulking in many cases.6
In a study with patients from the PREPARE-CALC and ISAR-CALC trials, the authors analyzed OCT of the 3 techniques (RA, CB or SB, and OPN balloon) exhibiting similar stent expansion, with lower stent eccentricity in the OPN group.34 To date, no randomized clinical trial has directly compared OPN with atherectomy techniques—likely because such a comparison may not be entirely appropriate, given the different mechanisms of action.
Overall, our data confirm the excellent performance, versatility, and safety profile of the OPN NC balloon in complex coronary lesion subsets, including ISR, bifurcations, ostial lesions, and cases requiring inflations beyond conventional limits. Its high-pressure performance, deliverability, and compatibility with standard 6F systems make it a practical and effective tool for contemporary PCI.1,3,26
Future prospective studies involving randomized clinical trials comparing the OPN balloon with other plaque modification strategies—such as atherectomy, lithotripsy, and modified balloons—are warranted to better define its role across different lesion subsets.
Recent comparative evidence between OPN and IVL has shown similar results in terms of safety and efficacy, with OPN demonstrating advantages in cost-effectiveness, procedural efficiency, and device deliverability. Future studies should aim to refine patient and lesion selection criteria to optimize the use of both modalities according to specific anatomical characteristics.
The routine incorporation of IVI should be encouraged to guide device selection, evaluate calcium modification, and ensure optimal stent expansion. In addition, the development of standardized, pressure-based inflation protocols and balloon sizing strategies may help improve procedural consistency and outcomes.
Finally, long-term follow-up studies are essential to confirm the durability of OPN-based lesion preparation and its impact on clinical outcomes over time.
Limitations
This study has several limitations inherent to its design. First, it is a retrospective, single-center observational registry with a limited sample size (even though it represents one of the largest series published to date regarding the use of this device). Second, the absence of a control group prevents direct comparison with other calcium modification techniques.
Third, IVI was not systematically performed, limiting the detailed assessment of calcium fracture and precise stent expansion. However, its use was higher than that reported in most real-world series, especially considering the long inclusion period, during which several imaging and modification techniques (OCT, ELCA, IVL, OA, etc.) were either unavailable or only gradually implemented in routine practice. Because of this, the use of motion-corrected X-ray techniques, which enhance the visualization of metallic stents, allowing for the evaluation of stent expansion and apposition, was essential. While the primary, FDA-cleared purpose of these techniques is to verify stent positioning and expansion after deployment, they are used during the broader "lesion preparation" phase to ensure optimal vessel preparation and to assess the success of predilation in complex cases.
Device and strategy selection were left to operator discretion, though efforts were made to follow the algorithm presented in Figure 1, which was adapted over time as new coronary tools became available. However, some potentially relevant variables were not collected, such as the type of guidewire used, wire entrapment with or without position loss, or the specific pressure at which balloon rupture occurred.
Finally, follow-up was limited to 1 year, and the long-term durability of outcomes remains to be determined. The relatively small sample size may also limit the statistical power to detect significant differences between subgroups.
Conclusions
The OPN super high-pressure NC balloon demonstrated an excellent safety and efficacy profile, with significant luminal gain confirmed by QCA in a large cohort of complex patients with calcified CAD. It was particularly effective in the treatment of ISR—including cases with calcified neoatherosclerosis—and in de novo lesions requiring inflation pressures greater than or equal to 40 atm, without a proportional increase in complications. These findings support the use of the OPN balloon as both a first-line and bailout tool for plaque modification and stent optimization in complex coronary interventions, as it offers a simple, effective, and cost-efficient approach that can often obviate the need for more invasive techniques.
Affiliations and Disclosures
Miguel Ángel Montilla-Garrido, MD1; Santiago Jesús Camacho-Freire, MD, PhD, Prof1,2; Elena Izaga-Torralba, MD, PhD1; Carmen Lluch-Requerey, MD1; Jessica Roa-Garrido, MD1; Oscar Lagos-De Grande, MD1; Antonio Enrique Gómez-Menchero, MD1
From the 1Cardiology Department, University Hospital Juan Ramon Jimenez, Huelva, Spain; 2Medicine Department, University of Huelva, Huelva, Spain.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Miguel Angel Montilla Garrido, Avenida Ronda Norte S/N, Huelva 21003, Spain. Email: montillagarrido@hotmail.com; X: @Montyks3, @CamachoFreire
References
1. Ng P, Maehara A, Kirtane AJ, et al. Management of coronary stent underexpansion. J Am Coll Cardiol. 2025;85(6):625-644. doi:10.1016/j.jacc.2024.12.009
2. Généreux P, Madhavan MV, Mintz GS, et al. Ischemic outcomes after coronary intervention of calcified vessels in acute coronary syndromes. Pooled analysis from the HORIZONS-AMI (Harmonizing Outcomes With Revascularization and Stents in Acute Myocardial Infarction) and ACUITY (Acute Catheterization and Urgent Intervention Triage Strategy) TRIALS. J Am Coll Cardiol. 2014;63(18):1845-1854. doi:10.1016/j.jacc.2014.01.034
3. Mattaroccia G, Redivo M, Cianca A, et al. The new era of coronary angioplasty: how cutting-edge technologies are redefining complex interventions. Heart Surg Forum 2025;28(1):107-119. doi:10.59958/hsf.8165
4. Madhavan MV, Tarigopula M, Mintz GS, Maehara A, Stone GW, Généreux P. Coronary artery calcification: pathogenesis and prognostic implications. J Am Coll Cardiol. 2014;63(17):1703-1714. doi:10.1016/j.jacc.2014.01.017
5. Sammour YM, Mohamed KA, El-Sabawi B, et al. Approach to coronary calcium and procedural techniques during percutaneous coronary intervention. Curr Treat Options Cardio Med. 2025;27:26. doi:10.1007/s11936-025-01083-5
6. Allali A, Richardt G, Toelg R, et al. High-speed rotational atherectomy versus modified balloons for plaque preparation of severely calcified coronary lesions: two-year outcomes of the randomised PREPARE-CALC trial. EuroIntervention. 2023;18(16):e1365-e1367. doi:10.4244/EIJ-D-22-00677
7. Vrints C, Andreotti F, Koskinas KC, et al; ESC Scientific Document Group. 2024 ESC guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024;45(36):3415-3537. doi:10.1093/eurheartj/ehae177
8. Maffey MW, Bagur R. Dedicated balloon techniques for coronary calcium modification. Interv Cardiol. 2024;19:e13. doi:10.15420/icr.2024.06
9. Pinilla-Echeverri N, Bossard M, Hillani A, et al. Treatment of calcified lesions using a dedicated super-high pressure balloon: multicenter optical coherence tomography registry. Cardiovasc Revasc Med. 2023;52:49-58. doi:10.1016/j.carrev.2023.02.020.
10. Rodriguez-Leor O, Cid-Alvarez AB, Lopez-Benito M, et al; REPLICA-EPIC18 Investigators. A prospective, multicenter, real-world registry of coronary lithotripsy in calcified coronary arteries: the REPLICA-EPIC18 study. JACC Cardiovasc Interv. 2024;17(6):756-767. doi:10.1016/j.jcin.2023.12.018
11. Díaz JF, Gómez-Menchero A, Cardenal R, Sánchez-González C, Sanghvi A. Extremely high-pressure dilation with a new noncompliant balloon. Tex Heart Inst J. 2012;39(5):635-638.
12. Kumar S, Jalli S, Sandoval Y, et al. Systematic review and meta-analysis of the super high-pressure balloon (SIS-OPN) for percutaneous coronary intervention. Catheter Cardiovasc Interv. 2025;105(4):938-950. doi:10.1002/ccd.31403
13. Raja Y, Routledge HC, Doshi SN. A noncompliant, high pressure balloon to manage undilatable coronary lesions. Catheter Cardiovasc Interv. 2010;75(7):1067-1073. doi:10.1002/ccd.22430
14. Secco GG, Buettner A, Parisi R, et al. Clinical experience with very high-pressure dilatation for resistant coronary lesions. Cardiovasc Revasc Med. 2019;20(12):1083-1087. doi:10.1016/j.carrev.2019.02.026
15. Secco GG, Ghione M, Mattesini A, et al. Very high-pressure dilatation for undilatable coronary lesions: indications and results with a new dedicated balloon. EuroIntervention. 2016;12(3):359-365. doi:10.4244/EIJY15M06_04
16. Seiler T, Attinger-Toller A, Cioffi GM, et al. Treatment of in-stent restenosis using a dedicated super high-pressure balloon. Cardiovasc Revasc Med. 2023;46:29-35. doi:10.1016/j.carrev.2022.08.018
17. Tanaka A, Jabbour RJ, Kawamoto H, Latib A, Colombo A. A super high-pressure balloon solution for a non-dilatable in-stent restenosis. Int J Cardiol. 2016;203:357-359. doi:10.1016/j.ijcard.2015.10.188
18. Senguttuvan NB, Singh H, Kumar BV, et al. Safety and efficacy of OPN balloon in patients with calcified coronary artery disease. Cardiovasc Revasc Med. 2023;54:25-30. doi:10.1016/j.carrev.2023.02.018
19. Kumaraguruparan LD, Polareddy DR, Kovvuri HR, et al. Safety and efficacy of super-high pressure OPN balloon in patients with in-stent restenosis - an intra-coronary imaging-based observational study. Sci Rep. 2025;15(1):36653. doi:10.1038/s41598-025-20488-7
20. Novelli L, Sorolla Romero JA, Diez Gil JL, Amat-Santos I, Brilakis ES, Sanz-Sanchez J. Guidewire friction following super high-pressure balloon percutaneous coronary intervention. JACC Cardiovasc Interv. 2025;18(7):956-957. doi:10.1016/j.jcin.2024.12.020
21. Buckley AJ, McCormick JP, Carey J, et al. Intravascular lithotripsy-assisted PCI for severely calcified coronary lesions: evaluating the impact on quality of life and outcomes. Ir J Med Sci. 2023;192(3):1085-1090. doi:10.1007/s11845-022-03077-9
22. Dini CS, Tomberli B, Mattesini A, et al. Intravascular lithotripsy for calcific coronary and peripheral artery stenoses. EuroIntervention. 2019;15(8):714-721. doi:10.4244/EIJ-D-18-01056
23. Bossard M. A randomized, multicenter, non-inferiority comparison of intravascular lithotripsy and super-high-pressure non-compliant balloons for treatment of calcified and refractory coronary lesions: the VICTORY trial. Abstract presented at: Transcatheter Cardiovascular Therapeutics (TCT) congress; October 26, 2025; San Francisco, CA. https://www.tctmd.com/slide/short-cut-randomized-trial-cracking-calcium-code
24. Sekimoto T, Fujiyoshi K, Kawakami R, et al. Comparison of vascular injury from intravascular lithotripsy, cutting, or ultra-high-pressure balloons during coronary calcium modification. JACC Cardiovasc Interv. 2025;18(17):2093-2104. doi:10.1016/j.jcin.2025.06.035
25. Baron S. The ShortCUT Trial: Shockwave Lithotripsy Compared to Cutting Balloon Treatment in Calcified Coronary Artery Disease. Abstract presented at: Transcatheter Cardiovascular Therapeutics (TCT) congress; October 26, 2025; San Francisco, CA. https://www.tctmd.com/slide/short-cut-randomized-trial-cracking-calcium-code
26. Fujii K, Carlier SG, Mintz GS, et al. Stent underexpansion and residual reference segment stenosis are related to stent thrombosis after sirolimus-eluting stent implantation: an intravascular ultrasound study. J Am Coll Cardiol. 2005;45(7):995-998. doi:10.1016/j.jacc.2004.12.066
27. Paolucci L, Shabbir A, Lombardi M, Jerónimo A, Escaned J, Gonzalo N. Management of stent underexpansion and aorto-ostial lesions. Interv Cardiol. 2024;19:e26. doi:10.15420/icr.2024.10
28. Madanchi M, Cioffi GM, Attinger-Toller A, et al. Long-term outcomes after treatment of in-stent restenosis using the Absorb everolimus-eluting bioresorbable scaffold. Open Heart. 2021;8(2):e001776. doi:10.1136/openhrt-2021-001776
29. Baudinet T, Seguy B, Cetran L, Luttoo MK, Coste P, Gerbaud E. Bail-out therapy in ST-segment elevation myocardial infarction due to calcified lesion causing stent underexpansion: Intravascular lithotripsy is in the lead. J Cardiol Cases. 2021;23(6):264-266. doi:10.1016/j.jccase.2020.12.014
30. Erriquez A, Pavasini R, Campo G. Strategie per la gestione della sotto-espansione dello stent [Management of stent under-expansion]. Article in Italian. G Ital Cardiol (Rome). 2020;21(6 Suppl 1):21S-26S. doi:10.1714/3373.33489
31. Rheude T, Rai H, Richardt G, et al. Super high-pressure balloon versus scoring balloon to prepare severely calcified coronary lesions: the ISAR-CALC randomised trial. EuroIntervention. 2021;17(6):481-488. doi:10.4244/EIJ-D-20-01000
32. Rao SV, O'Donoghue ML, Ruel M, et al. 2025 ACC/AHA/ACEP/NAEMSP/SCAI guideline for the management of patients with acute coronary syndromes: a report of the American College of Cardiology/American Heart Association joint committee on clinical practice guidelines. Circulation. 2025;151(13):e771-e862. doi:10.1161/CIR.0000000000001309
33. McQuillan C, Jackson MWP, Brilakis ES, Egred M. Uncrossable and undilatable lesions-a practical approach to optimizing outcomes in PCI. Catheter Cardiovasc Interv. 2021;97(1):121-126. doi:10.1002/ccd.29001
34. Rheude T, Fitzgerald S, Allali A, et al. Rotational atherectomy or balloon-based techniques to prepare severely calcified coronary lesions. JACC Cardiovasc Interv. 2022;15(18):1864-1874. doi:10.1016/j.jcin.2022.07.034













