Endovascular Repair of Recurrent Coarctation With Pseudoaneurysm After Prior Bare-Metal Stent Using Thoracic Branched Endoprosthesis
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00119. Epub May 22, 2026.
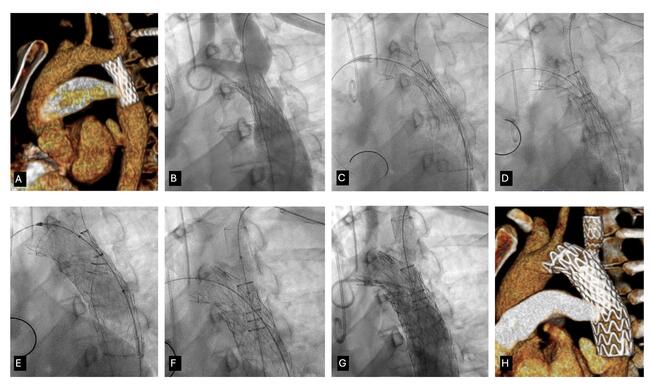
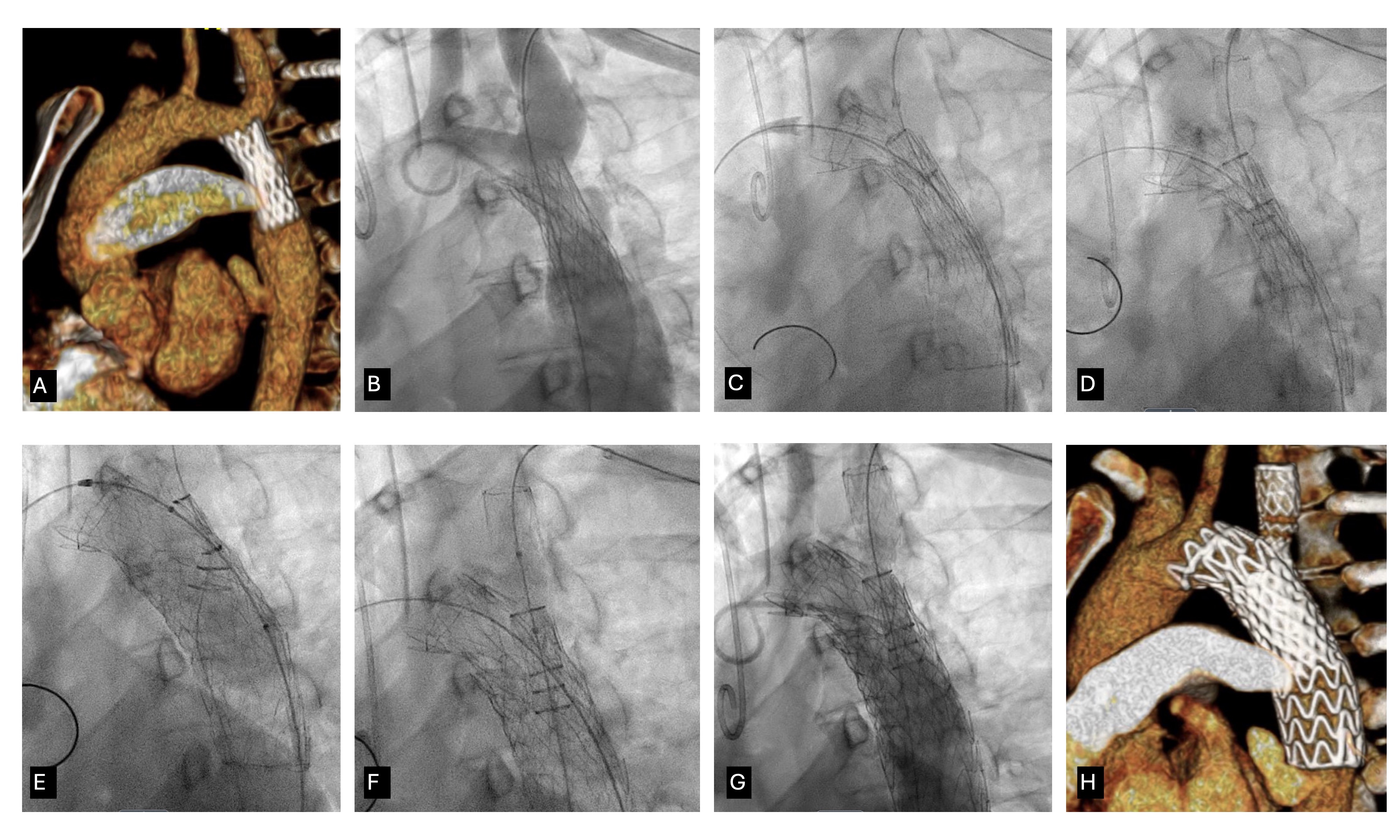
Off-the-shelf thoracic branch endoprostheses (TBE) were developed for treatment of thoracic aortic dissections and aneurysms. Endovascular repair of recurrent coarctation of the aorta (CoA) after prior stenting can be challenging, particularly in the setting of an associated pseudoaneurysm and proximity to the left subclavian artery. We report use of a TBE to treat recurrent CoA in a patient with a prior 4010 Palmaz XL stent (Cordis) presenting with an aortic pseudoaneurysm and a peak-to-peak gradient of 29 mm Hg between the ascending and descending aorta (Figure A and B).
Under general anesthesia, percutaneous right radial, left radial, and femoral arterial access were obtained with 5F, 6F, and 22F sheaths, respectively. A 6F sheath was placed in the right common femoral vein, and a temporary pacing wire was advanced into the right ventricle to allow optional rapid pacing during balloon angioplasty for improved graft stability and reduced device movement. A Lunderquist wire (Cook Medical) was positioned in the ascending aorta, and a 450-cm Dreamwire (Boston Scientific) was advanced from the left radial artery and externalized via the left femoral artery. A pigtail catheter was positioned in the ascending aorta.
A 28-mm × 10-cm GORE TBE graft (W.L. Gore & Associates) was deployed across the coarctation, extending beyond the left subclavian artery (Figure C). A 15-mm × 6-cm branch graft was deployed into the left subclavian artery (Figure D). Balloon angioplasty was performed with a 22-mm Atlas Gold balloon (BD) during rapid pacing, followed by branch-graft post-dilation (Video). Final angiography demonstrated no residual gradient, and follow-up computed tomography confirmed a patent graft without residual stenosis or bronchial compression (Figure E-H).
This case highlights the ability of TBE technology to address complex recurrent CoA with associated pseudoaneurysm and prior stent implants in a single-stage endovascular approach while preserving branch vessel perfusion.
Affiliations and Disclosures
Pradyumna Agasthi, MD1; Kaitlyn Krebushevski, MD2,3; Allison K. Cabalka, MD2,3; Jason H. Anderson, MD2,3
From the 1Department of Cardiology, Saint Francis Heart and Vascular Institute, Tulsa, Oklahoma; 2Department of Pediatric and Adolescent Medicine, Division of Pediatric Cardiology, Mayo Clinic, Rochester, Minnesota; 3Department of Cardiovascular Medicine, Division of Structural Heart Diseases, Mayo Clinic, Rochester, Minnesota.
Disclosures: Dr Cabalka is a consultant for Edwards Lifesciences and B. Braun Medical, Inc. Dr Anderson is on the cardiac advisory board for W.L. Gore & Associates and is a consultant for Edwards Lifesciences and Medtronic.
Consent statement: The authors confirm that informed consent was obtained from the patient for the intervention and publication of this report, including all associated images.
Address for correspondence: Jason H. Anderson, MD, Mayo Clinic, Rochester, MN 55905, USA. Email: Anderson.Jason@mayo.edu; X: @Dr_JHAnderson, @PradyAgasthiMD