Caught in the Web: Alteplase-Assisted Rescue of an Entrapped Pericardial Pigtail
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00110. Epub April 30, 2026.
A 12-year-old boy with a case of disseminated tuberculosis (clinically and microbiologically diagnosed) who was on guideline-directed oral antitubercular therapy (ATT) presented to the outpatient clinic with worsening exertional dyspnea (New York Heart Association III severity) for the past 2 months. He initially presented 2 years ago with a low-grade fever, weight loss, and cervical and mediastinal lymphadenopathy, which led to a diagnosis of disseminated tuberculosis (rifampicin sensitive); subsequently, ATT was initiated. After 12 months, clinical improvement with resolution of cervical lymphadenopathy was noted, leading to initiation of the continuation phase of treatment.
At the current presentation—18 months after initiation of ATT—he was afebrile; however, cervical lymphadenopathy had recurred. On examination, his jugular venous pressure was elevated, heart rate was 120 beats per minute with a regular pulse, and respiratory rate was 20 breaths per minute with bilateral normal vesicular breath sounds. Cardiac auscultation revealed muffled heart sounds without any murmur.
Transthoracic echocardiography revealed a massive pericardial effusion with features of impending cardiac tamponade. A 6F pericardial pigtail catheter was inserted, serosanguinous fluid was drained, and oral corticosteroids were added to the ongoing ATT. Pericardial fluid analysis showed a lymphocytic exudate, which was negative for acid fast bacilli and negative on Gene Xpert, a nucleic acid amplification test (Cepheid). Mycobacteria growth indicator tube (BD) culture was negative. Serum inflammatory markers were elevated and serum procalcitonin was negative. Contrast-enhanced computed tomography (CT) of the thorax showed persistent mediastinal lymphadenopathy with pericardial effusion.
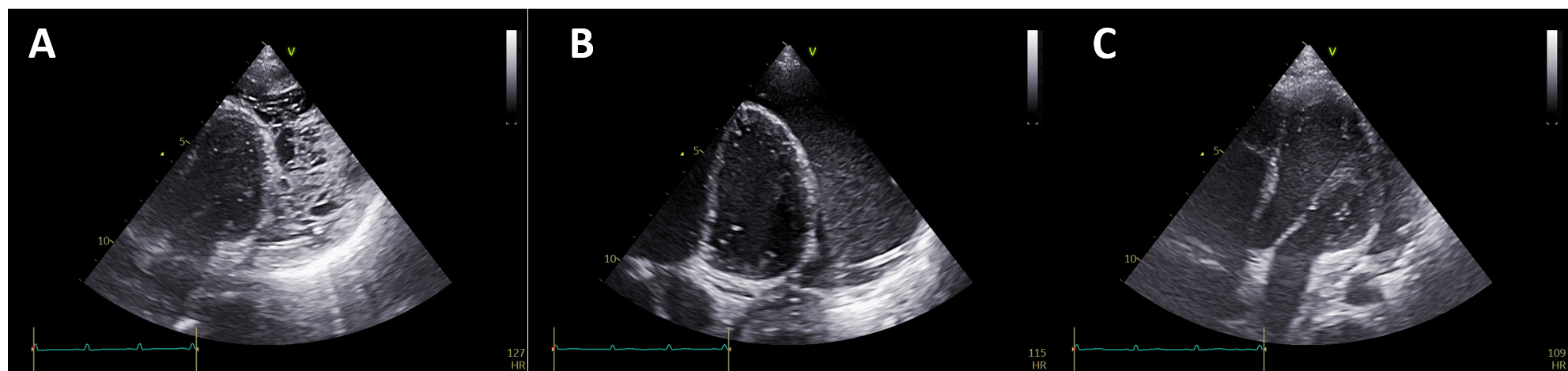
In view of clinical worsening during the continuation phase, the intensive phase of ATT was reinitiated. Over the next 2 weeks, the pericardial fluid drainage through the pigtail was reduced with mild improvement in dyspnea. Echocardiography was performed to assess the need for repositioning or removal of the pigtail catheter. However, it showed a heterogeneous pericardial collection having both fluid and organized components, with the pigtail catheter embedded within the organized component, thereby leading to nil drainage (Figure 1A). A fluoroscopy-guided attempt to manipulate the pigtail using a 0.035-inch J-tip wire (Terumo) wire was unsuccessful. The Terumo wire negotiated beyond the terminal end hole of the pigtail; however, the catheter could not be mobilized despite sustained push and traction. Attempted gentle traction to the pigtail catheter caused severe pain, further limiting forceful manipulation.
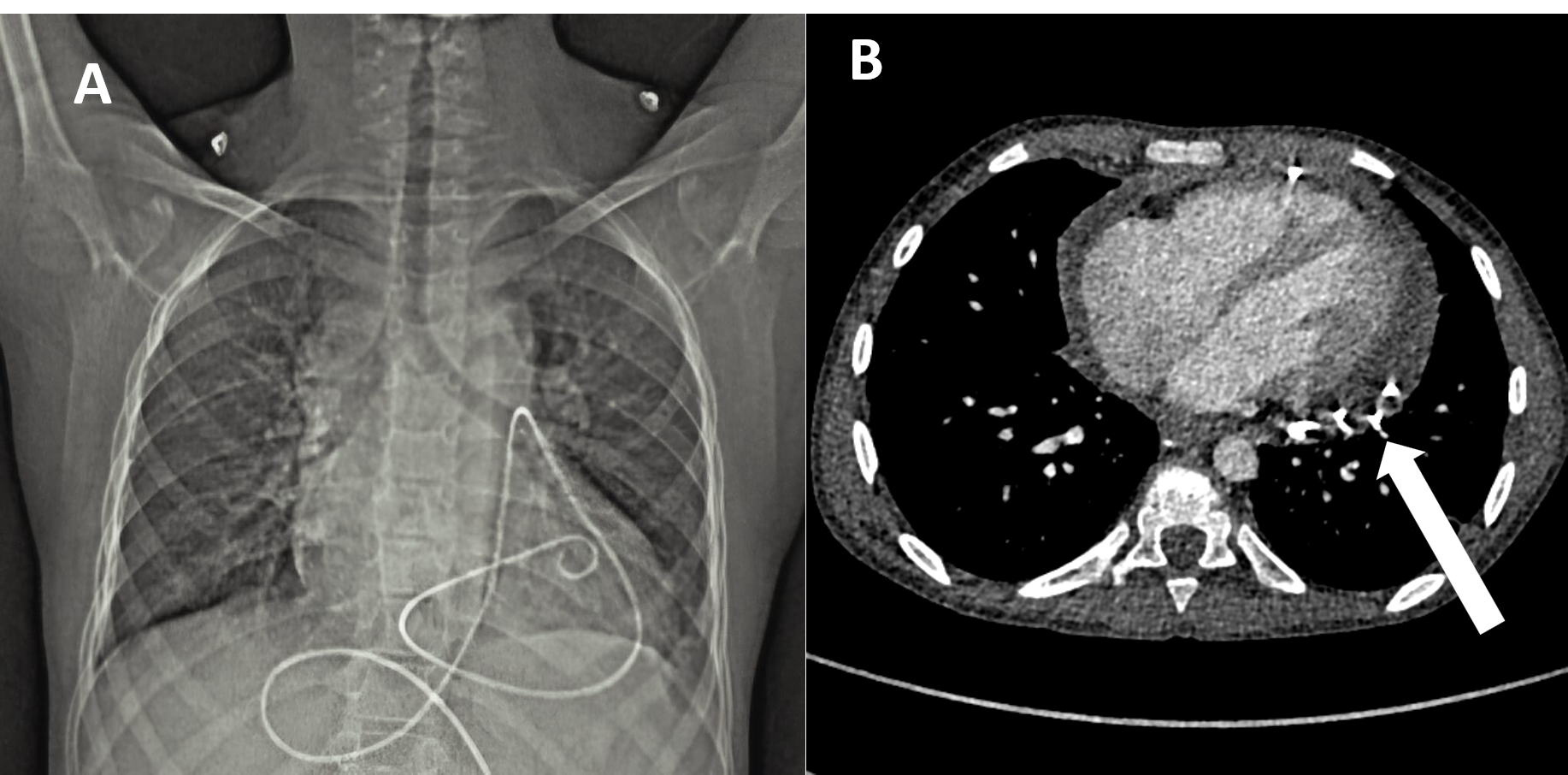
The chest CT obtained earlier showed the catheter to be intact throughout its length and showed no evidence of knotting along its course (Figure 2A, Video 1). These findings were confirmed fluoroscopically. This suggested that the pigtail catheter was entrapped between the dense septations within the organized pericardial collection (Figure 2B).
Alteplase (0.1 mg/kg) was instilled intrapericardially through the catheter to lyse the dense pericatheter-organized collection. Twelve hours later, an additional dose (0.1mg/kg) was instilled to increase lysis of the adhesions. Twenty-four hours after instillation of the first dose, echocardiography showed homogenization of the collection with dissolution of the organized component (Figure 1B). The collection was aspirated in full and the pigtail catheter was successfully removed. On follow-up echocardiography, there was significant resolution of the pericardial effusion and the patient was discharged (Figure 1C, Video 2). He remained well on follow-up for 1 month with no sign of pericardial constriction on echocardiography, and is currently receiving the intensive phase followed by continuation phase of ATT.
Tuberculous pericarditis accounts for most cases of effusive pericarditis in low-middle-income countries. Pericardiocentesis is indicated for symptomatic large pericardial effusion unresponsive to medical therapy, or when bacterial or neoplastic pericarditis is suspected. Entrapment of a pericardial pigtail catheter could be due to knot formation, extensive looping around the heart or great vessels, catheter fracture, or entrapment between dense septations within exudative pericardial effusions. Routinely available imaging and the use of fibrinolytic drugs can help avoid the need for surgical extraction of the entrapped catheter. Through this case, we share our experience and contribute to the scarce literature on management of pericardial tuberculosis and its complications.
Affiliations and Disclosures
Swaminathan Krishnaswamy, MBBS, MD; Shivam Goel, MBBS, MD, DM; Shashwat Joshi, MBBS; Ankur Handa, MBBS, MD, DM; Sivasubramanian Ramakrishnan, MBBS, MD, DM; Sourabh Agstam, MBBS, MD, DM
From the Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient(s) for the study and/or intervention(s) described in the manuscript and for the @publication of their data/thereof, including any and all images.
Address for correspondence: Sourabh Agstam, MD, DM, MRCP(UK), FACC, Department of Cardiology, 7th Floor, Cardiothoracic Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi, 110029, India. Email: sourabhagstam@gmail.com; X: @AgstamSourabh