Late Endovascular Aneurysm Repair Limb Occlusion Presenting as Claudication: Lifelong Surveillance Essential
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00111. Epub May 4, 2026.
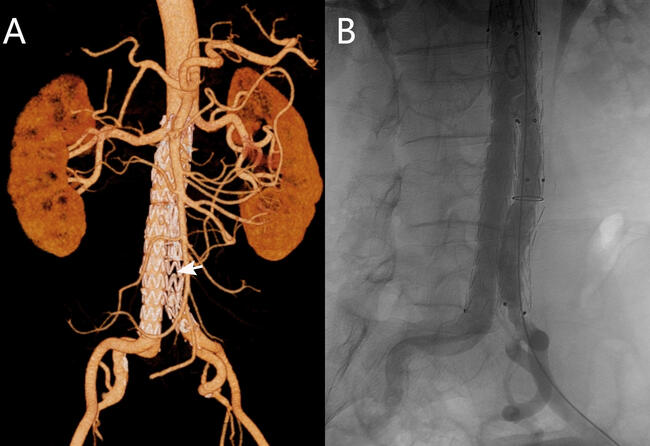
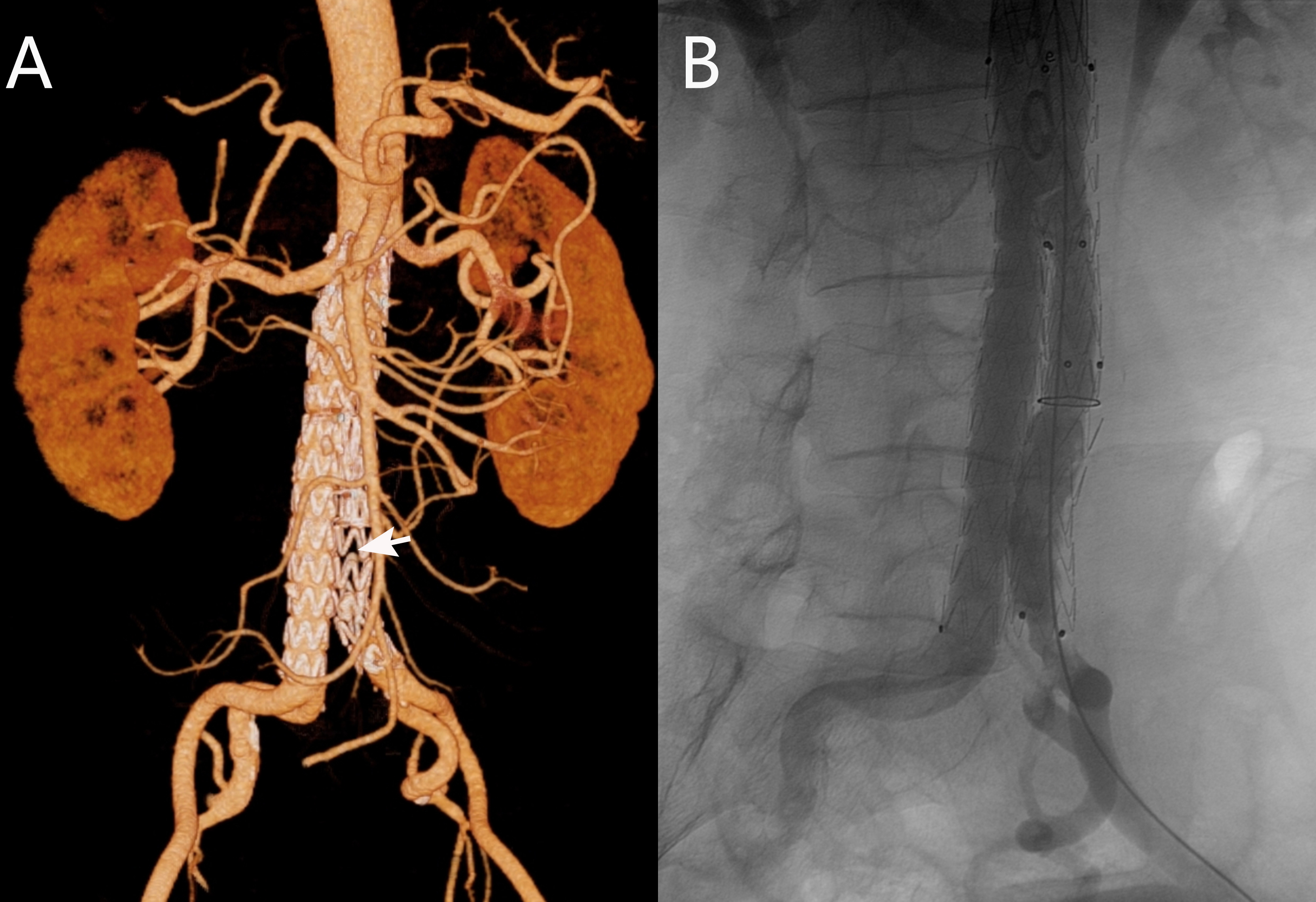
Iliac limb occlusion is a recognized late complication following endovascular aneurysm repair (EVAR) for abdominal aortic aneurysm (AAA), potentially leading to critical limb ischemia. We report the case of a 55-year-old man with medically controlled essential hypertension and a history of AAA stenting 2 years prior who presented with a 3-month history of left lower extremity fatigue on exertion. Physical examination revealed diminished left dorsalis pedis and posterior tibial pulses. Diagnostic workup confirmed moderate ischemia with a left ankle-brachial index (ABI) of 0.57 (right ABI 1.12) and an elevated D-dimer level (1.75 μg/mL). Computed tomography angiography (CTA) demonstrated complete occlusion of the left iliac limb of the stent-graft (Figure A).
The patient underwent successful endovascular intervention via left femoral access under local anesthesia, which included mechanical thrombectomy using an AngioJet Solent Omni catheter (Boston Scientific) followed by balloon angioplasty with an Atlas Gold PTA catheter (BD). Postprocedural angiography confirmed restored patency (Figure B, Video). He was discharged on dual antiplatelet therapy (rivaroxaban 20 mg/day and clopidogrel 75 mg/day) with marked symptom improvement. At 1-month follow-up, his symptoms had resolved, the left ABI had improved to 0.89, and CTA confirmed sustained limb patency.
Limb graft occlusion (LGO) is a rare but serious complication after endovascular aneurysm repair (EVAR), most commonly occurring within the first year. Our patient’s new-onset claudication led to prompt diagnosis by ankle-brachial index (ABI) and CTA, enabling successful endovascular recanalization. This case highlights a critical lesson: symptom-triggered evaluation must be backed by structured follow-up, as delayed detection risks limb-threatening ischemia. Regular ABI and imaging surveillance remain the cornerstone of early intervention and long-term EVAR success.
Affiliations and Disclosures
Ping Hu, MD1; Xin-yu Wang, MD2; Ming Qi, MD3; Jie Wang, MD1; Xiao-Jing Ma, PhD1
From the 1Department of Image Center, Wuhan Asia Heart Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, China; 2Department of Cardiology, Wuhan Asia Heart Hospital Affiliated to Wuhan University of Science and Technology, Wuhan, China; 3Department of Cardiovascular Surgery, Wuhan Asia Heart Hospital, Wuhan, China.
Drs Hu, X-y Wang, Qi, and J Wang served as co-first authors.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Funding: This work was funded by the Wuhan Clinical Medical Research Center for Cardiovascular Imaging (CMRC202302).
Consent statement: This report has obtained the patient's informed consent for the publication of their anonymized clinical data.
Data availability statement: The data that support the findings of this study are available from the corresponding author.
Address for correspondence: Xiao-Jing Ma, PhD, Department of Image Center, Wuhan Asia Heart Hospital Affiliated to Wuhan University of Science and Technology, No 753 Jinghan Road, Hankou District, Wuhan 430022, China. Email: ma312312ma@163.com