Endovascular Management for Symptomatic Superior Vena Cava Syndrome in a Patient on Hemodialysis
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
J INVASIVE CARDIOL 2026. doi:10.25270/jic/26.00136. Epub May 21, 2026.
A 59-year-old woman with end-stage renal disease undergoing maintenance hemodialysis through sequential right and left internal jugular venous catheters presented with progressive facial and neck swelling, dyspnea, and a non-functioning, left-arm arteriovenous fistula. Clinical evaluation was consistent with superior vena cava (SVC) syndrome. Computed tomography venography demonstrated complete occlusion of the SVC with bilateral brachiocephalic vein (BCV) thrombosis and large left pleural effusion.
The pleural fluid was sterile and chylous. Anticoagulation and a fat-restricted diet produced no improvement, and urgent endovascular revascularization was performed to relieve severe venous congestion and maintain future access options.
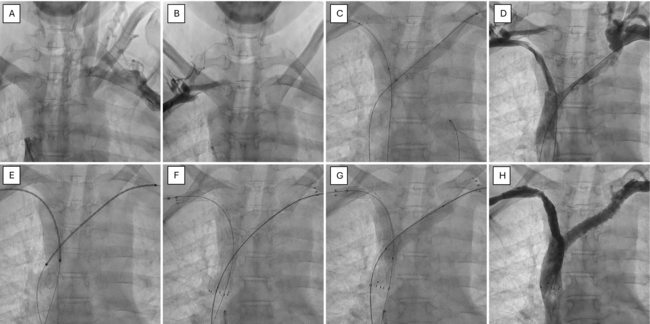
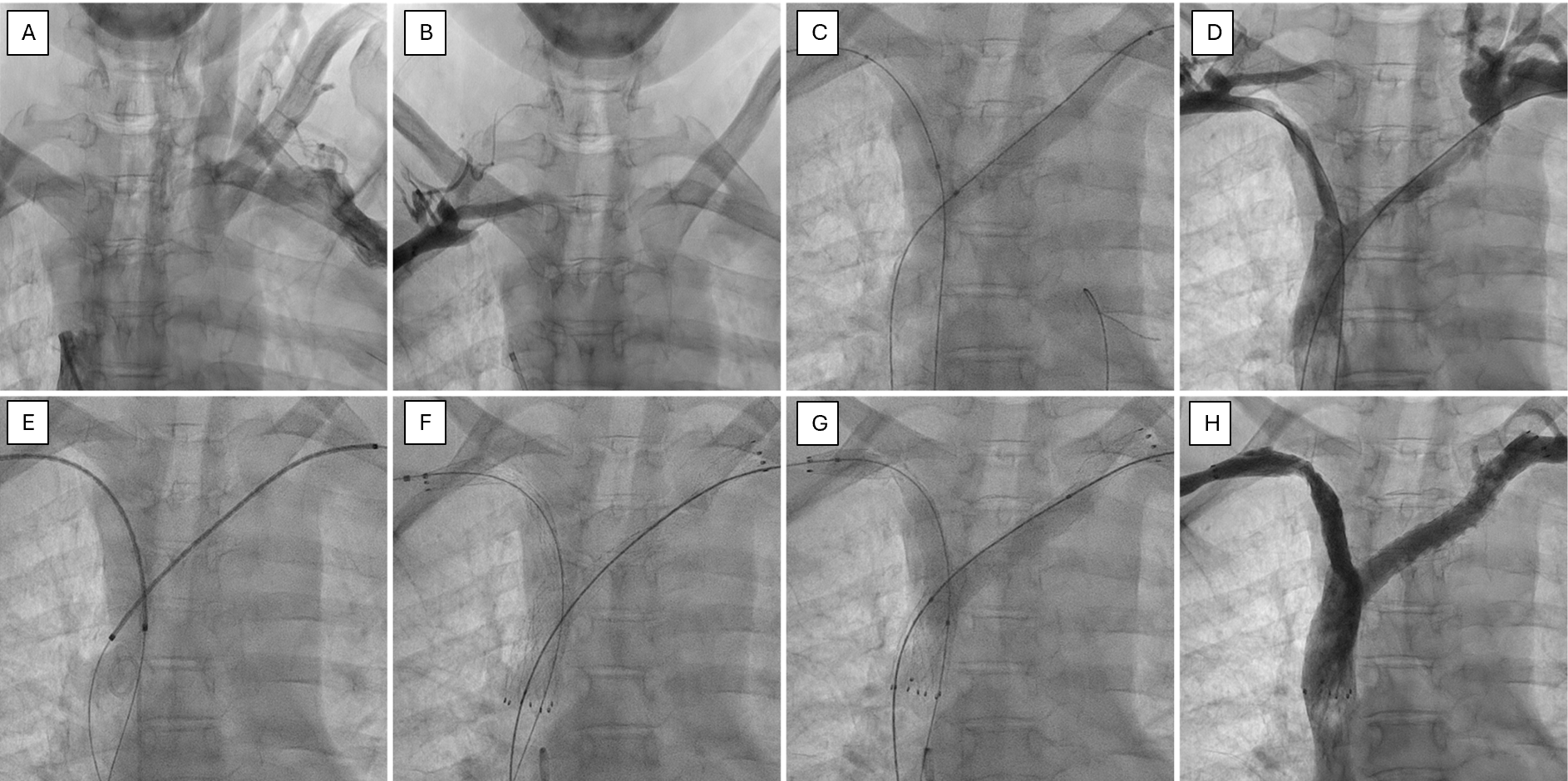
Via bilateral axillary and right femoral venous access, mechanical recanalization of both BCVs and the SVC was achieved using a 0.035-inch-hydrophilic guidewire supported by a 6F Judkins Right catheter. Balloon angioplasty was performed, followed by implantation of bilateral self-expandable LifeStar stents (BD) (14 × 100 mm on the left and 12 × 100 mm on the right) using the simultaneous kissing stent technique. Final kissing balloon dilatation (12 × 40-mm Atlas [BD] on the left and 10 × 40-mm Fortrex [Medtronic] on the right) restored unobstructed flow into the right atrium (Figure 1, Video).
Symptoms resolved immediately and the patient was discharged after 48 hours on anticoagulation and dual antiplatelet therapy (Figure 2). At the 6-month follow-up, Doppler ultrasound confirmed stent patency, and she remained asymptomatic without recurrence of chylothorax.

This case highlights the fact that, while unilateral SVC stenting is usually preferred for its similar efficacy, lower cost, simpler technique, and fewer complications, bilateral stents may be necessary in select cases to allow future catheter access. The approach is safe and can improve quality of life.
Affiliations and Disclosures
Keshav Sachdeva, MD, DM1; Hardik Jain, MD, DM1; Suraj Kumar, MD, DM1; Tejinder Singh Malhi, MD, DM1; Saurabh Nayak, MD, DM2; Bhupinder Singh, MD, DM1
From the Departments of 1Cardiology and 2Nephrology, All India Institute of Medical Sciences, Bathinda, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Consent statement: The authors confirm that informed consent was obtained from the patient and family for the intervention described in the manuscript and for the publication of thereof, including photographs.
Address for correspondence: Bhupinder Singh, MD, DM, Department of Cardiology, All India Institute of Medical Sciences, Bathinda 151001, India. Email: dr_bhupinders@yahoo.in