Minimally Invasive Bunion Correction Using 100% Capital Fragment Translation: A Case Series
Minimally invasive surgery (MIS) continues to reshape bunion correction, but questions remain around the limits of deformity correction. This case series explores the clinical outcomes of an aggressive approach—100% lateral translation of the capital fragment—demonstrating reliable union and acceptable complication rates. The findings offer practical insights into when and how this technique can be safely applied in modern foot and ankle practice.
Key Takeaways
- Feasibility of Aggressive Correction: Complete (100%) lateral translation of the capital fragment in MIS bunion surgery achieved successful union in all cases in this series, demonstrating it as a potentially viable option for severe deformities.
- Cases Revealed Acceptable Outcomes with Manageable Complications: While union rates were high, the most common complications were related to hardware prominence and occasional delayed healing—not loss of correction or fixation failure.
- Patient Selection and Technique Are Critical: Optimal outcomes depend on careful patient selection, surgeon experience, and appropriate use of adjunct procedures like Akin osteotomy.
Hallux abducto valgus (HAV), or bunion deformity, affects roughly 23% of adults aged 18–65 and up to 36% of individuals over 65.1,2 It is characterized by pain to the first metatarsal phalangeal joint (MPJ), lateral deviation of the hallux, often abutting or overlapping the second digit, and medial prominence of the first metatarsal head. Radiographically, HAV presents with increased hallux valgus angle (HVA) and intermetatarsal angle (IMA), with normal values being <15° and <9°, respectively.1
The cause of HAV is multifactorial. Genetics play a role, along with structural factors such as a short or dorsiflexed first metatarsal, forefoot varus, pes plano valgus, gastrocnemius equinus, and first ray hypermobility.2 The deformity occurs predominantly in females, with a reported female-to-male ratio of 15:1.1 Footwear may worsen symptoms, but is not considered a primary cause.
Conservative treatments including stretching of the first metatarsophalangeal joint, wide or accommodative shoes, custom orthotics, and nonsteroidal anti-inflammatory drugs (NSAIDs) (primarily for symptom relief), but definitive management often requires surgical correction. Minimally invasive surgery (MIS) has gained popularity for bunion correction due to smaller incisions and improved cosmesis. First described in the 1960s, MIS techniques saw mixed early results, but technological advances over the past 10–15 years have improved outcomes.3
While numerous studies describe MIS bunion correction techniques, few report outcomes when the surgeon translates the capital fragment 100% along the metatarsal shaft. Existing reports on high translation focus largely on biomechanical stability in cadaveric models, leaving limited clinical data on actual surgical patients.4,5
This case series presents 5 patients who underwent MIS bunion correction surgery with complete (100%) translation of the capital fragment. The aim is to showcase these examples, so surgeons can evaluate the effectiveness of this aggressive correction, including union rates, radiographic improvement, and potential complications.
Surgical Approach and Postoperative Strategy
The senior author (MG) performed all procedures in this series and routinely performs minimally invasive bunion correction. In the cases presented, he achieved a 100% lateral translation of the capital fragment, with the degree of translation confirmed intraoperatively under fluoroscopy. The overall surgical approach remained consistent across patients.
The procedures began with a small dorsal-medial stab incision at the neck of the first metatarsal, clearing of the soft tissue was cleared, and a transverse osteotomy proximal to the sesamoids performed with a burr. Continuous irrigation prevented thermal necrosis for the duration of the osteotomy. The surgeon translated the capital fragment laterally to the desired alignment and secured the site with 1 headless bevelled screws. He then used a burr to contour the residual medial prominence proximal to the osteotomy as needed. An Akin osteotomy, when needed, addresses cases of persistent residual hallux abutment on the second digit after correction, using a headless screw across the osteotomy site directed from the lateral head of the proximal phalanx to the medial base. All patients provided informed consent for this additional procedure preoperatively, the surgeon decided on applicability intraoperatively.
Postoperatively, patients participated in a protected weight bearing protocol, with non-weight-bearing restrictions applied in cases involving additional procedures. Follow-up occurred at routine postoperative intervals, with radiographs obtained when available. Ideally, patients obtained X-rays at 2 weeks, 6 weeks, and 3 months postoperatively. The team defined union as the presence of osseous bridging across the osteotomy site between the metatarsal shaft and capital fragment on radiographic evaluation.
Details From the Case Series
Case 1
This first patient is a healthy 41-year-old female with a greater than 5-year history of a painful left bunion deformity. She previously attempted conservative care for 1 year and subsequently elected to pursue surgical management. On examination, she demonstrated pain to palpation of the first metatarsal head and medial eminence. On preoperative weight-bearing radiographs, the hallux valgus angle (HVA) and intermetatarsal angle (IMA) measured 25.39° and 18.23°, respectively.
She underwent minimally invasive (MIS) bunionectomy and MIS Akin osteotomy of the left foot. The osteotomy included 100% lateral translation of the capital fragment and fixation with 2 bevelled, headless screws (4.0 × 36 mm and 4.0 × 48 mm). The Akin osteotomy fixation was with a headless compression screw (2.5 × 36 mm).
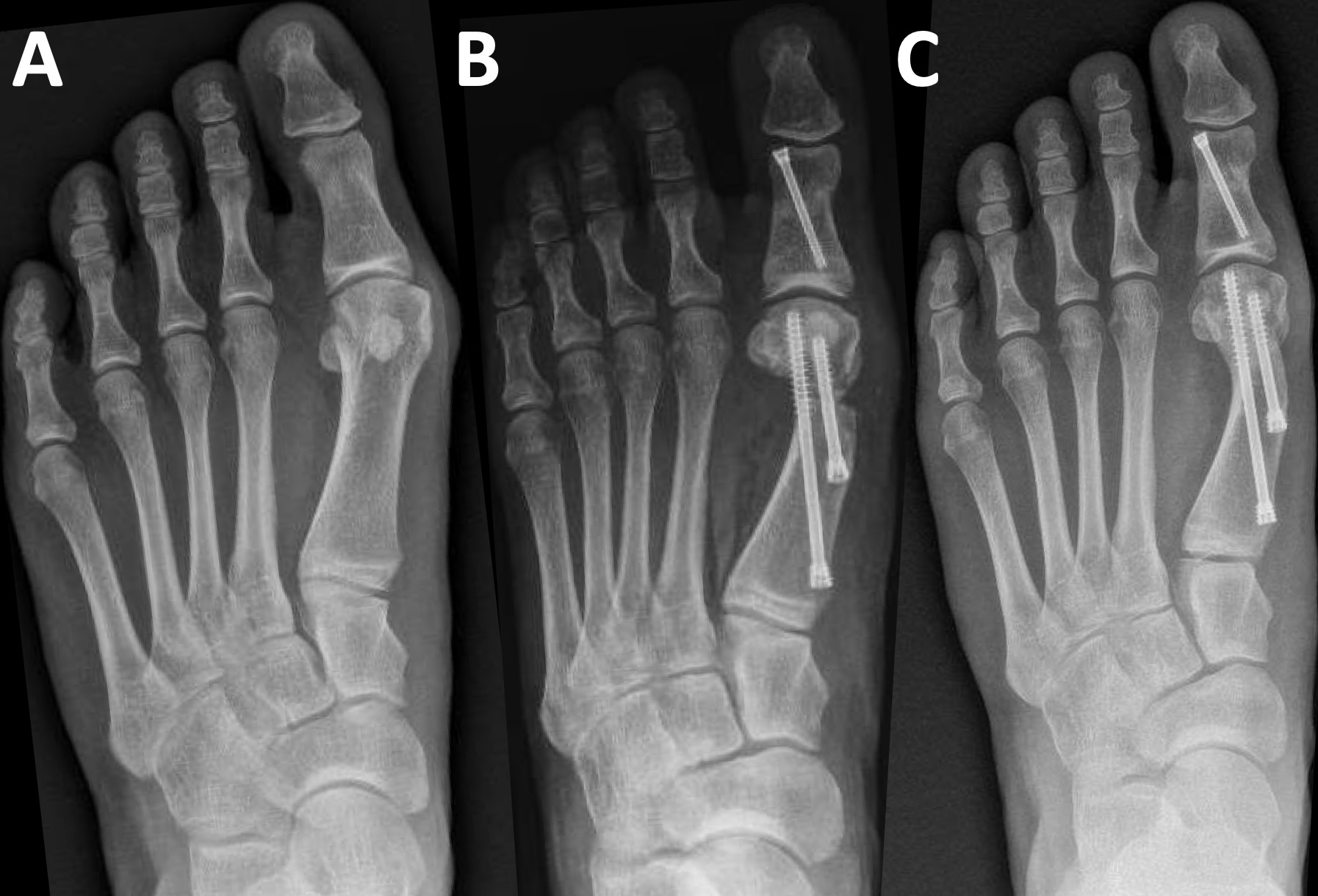
Postoperatively, the patient was permitted protected weight-bearing in a surgical shoe. She remained adherent to recommendations, and her postoperative course was uncomplicated. We observed osseous bridging at 3.5 months, with first metatarsal regeneration (FMR) type I noted.6 At that time we released her and advised her to return to the clinic as needed. Preoperative, immediate postoperative, and full-union radiographs are shown in Figures 1a, 1b, and 1c, respectively.

Case 2
This patient is a healthy 25-year-old female who also presented with painful left bunion deformity. Her pain was exacerbated by shoe gear and activity and improved with rest. Shoe modifications provided only partial relief. On examination, she demonstrated a medially deviated first metatarsophalangeal joint with abutment of the hallux against the second digit. Range of motion at the first MPJ was trackbound and painful, without crepitation, and first ray range of motion was normal. On preoperative weight-bearing radiographs, the HVA and IMA measured 19.61° and 10.62°, respectively.
She elected surgical treatment and underwent MIS bunionectomy of the left foot. A 100% lateral translation of the capital fragment took place with two bevelled, headless screws (3.5 × 32 mm and 3.5 × 50 mm) as fixation.
Postoperatively, we also permitted protected weightbearing for this patient. She remained adherent to that recommendation, also having an uncomplicated postop course. Evidence of osseous bridging appeared under 3 months postoperatively, with FMR type II noted. She was also released to return to the clinic as needed. Preoperative, immediate postoperative, and full-union radiographs are shown in Figure 2a, 2b, and 2c, respectively.

Case 3
This 44-year-old male presented with a painful left bunion deformity, with symptoms worsened by activity. Examination revealed tenderness to the medial eminence with dorsal-medial erythema. The laterally deviated hallux abutted the second digit. Range of motion at the first MPJ was trackbound, with normal firstray range of motion. On preoperative weight bearing radiographs, the HVA and IMA measured 22.97° and 13.54°, respectively.
His procedures included MIS bunionectomy and MIS Akin osteotomy of the left foot. He also underwent 100% lateral translation of the capital fragment and fixation with 2 beveled, headless screws (4.0 × 46 mm and 4.0 × 54 mm). The Akin osteotomy fixation was with a headless compression screw (2.5 × 26 mm).
Postoperatively, we allowed protected weight-bearing. Radiographic evaluation demonstrated complete osseous union by approximately 3 months. A computed tomography scan obtained at 1-year postoperatively confirmed solid union, with only minimal proximal perihardware lucency and slight extension beyond the metatarsal head at the MTJ noted. We also identified FMR type II configuration. Despite successful radiographic healing, the patient experienced persistent pain localized to the first metatarsophalangeal joint a year postop. A corticosteroid injection provided temporary symptomatic relief; however, due to continued symptoms, he ultimate underwent hardware removal of both metatarsal screws approximately 14 months after the index procedure. The patient has since reported good clinical improvement. Preoperative, immediate postoperative, and full-union post hardware removal radiographs are shown in Figures 3a, 3b, and 3c, respectively.

Case 4
In this case the patient is a 34-year-old female who presented with a painful left bunion deformity. Examination demonstrated a painful medial eminence and trackbound range of motion of the first MPJ. On preoperative weight-bearing radiographs, the HVA and IMA measured 24.30° and 10.20°, respectively.
She underwent MIS bunionectomy and MIS Akin osteotomy of the left foot. A 100% lateral translation of the capital fragment took place, fixated with 2 bevelled, headless screws (4.0 × 32 mm and 4.0 × 50 mm). The Akin osteotomy was fixated with a headless compression screw (2.5 × 26 mm).
Postoperatively, the patient executed protected weightbearing. The postoperative course was notable for persistent pain at the first MPJ associated with slight hardware prominence, particularly in shoe gear. She is considering hardware removal; however, no additional procedures have been performed to date. Osseous bridging became evident at just under three months postoperatively, with FMR type III noted. Preoperative, immediate postoperative, and full-union radiographs are shown in Figure 4a, 4b, and 4c, respectively.
Case 5
This patient is a 48-year-old female with a history of prior cigarette smoking who presented with painful right bunion deformity, along with a neuroma and chronic second MPJ dislocation present for approximately 2 years. Examination demonstrated tenderness to compression of the medial eminence, a positive Lachman test of the second toe, and positive Mulder’s click. On preoperative weight-bearing radiographs, the HVA and IMA measured 33.56° and 12.44°, respectively.
She underwent MIS bunionectomy and MIS Akin osteotomy of the right foot, including 100% lateral translation of the capital fragment fixated with 2 bevelled, headless screws (3.5 × 36 mm and 4.0 × 52 mm). The Akin osteotomy was fixated with a headless compression screw (2.5 × 26 mm). Additionally, she underwent plantar plate repair of the second MPJ with Weil osteotomy of the second metatarsal and neuroma excision.
Postoperatively, we kept the patient non-weight-bearing for 4 weeks, followed by transition to protected weight-bearing for an additional 4 weeks. During her postoperative course she experienced pain at the medial bunion screw and loosening of the plantar plate suture anchor. Full osseous union did not appear until eight months postoperatively, FMR type I noted. Removal of the prominent screw and suture anchor took place 10 months after the index procedure, with no further complications to date. Preoperative, immediate postoperative, and full-union post hardware removal radiographs are shown in Figure 5a, 5b, and 5c, respectively.

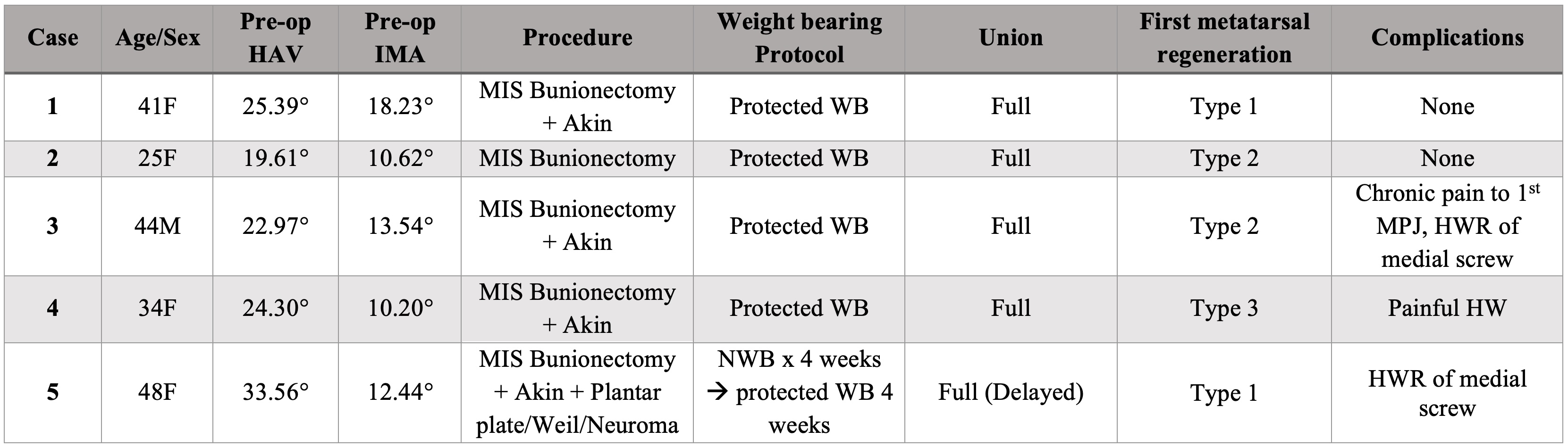
Table 1 summarizes the demographic and clinical characteristics, surgical procedures, post-operative weight-bearing protocols, union status, first metatarsal regeneration (FMR), and complications for all 5 cases. All patients underwent minimally invasive (MIS) bunion correction, with additional procedures performed as indicated. Postoperative management was primarily protected weight-bearing, with one patient initially non-weight-bearing. All cases went on to full radiographic union, with complications ranging from painful hardware to chronic first metatarsophalangeal joint pain requiring delayed management in select patients.
What These Cases Reveal About 100% Translation
The cases presented in this series demonstrate that 100% translation of the capital fragment along the first metatarsal shaft is technically feasible using a minimally invasive bunion technique. All patients achieved union across the osteotomy site, although 2 experienced delayed union. Three complications occurred, most commonly related to hardware prominence rather than hardware failure or loss of correction.
These findings align with the expanding body of literature supporting MIS bunion correction. Siddiqui and colleagues reported 217 feet treated with MIS techniques without major complications and with universal union, including bilateral procedures.7 Comparative studies have shown MIS approaches may provide faster recovery, fewer wound complications, higher patient satisfaction, and improved quality-of-life outcomes compared to open techniques.8-10
Hardware removal remains one of the more frequently reported MIS complications. A systematic review of 1,088 MIS bunions across 17 studies reported a hardware removal rate of approximately 6%, and higher removal rates have been observed when compared with open procedures.9,11 Although our sample size limits statistical interpretation, hardware removal was likewise the most common complication in our series.
Some authors have suggested that MIS techniques may be less effective for larger bunion deformities.8,12 However, our experience with complete (100%) capital fragment translation demonstrates that aggressive correction can be achieved with acceptable healing and complication profiles in appropriately selected patients.
Other considerations associated with MIS surgery include increased fluoroscopy exposure, however this typically reduces with surgeon experience.9 Another complication is the potential development of a “pseudobunion” due to inadequate resection of the medial shelf, reported more commonly with larger shifts and two-screw constructs.13 None of our patients developed this issue, likely due to aggressive medial shelf resection at the index procedure.
Radiographically, 100% capital fragment translation may initially appear atypical when compared with conventional osteotomy constructs; however, patients in our series demonstrated favorable and reliable healing patterns. When evaluated using the first metatarsal regeneration classification recently described by Blitz and team, all 3 regeneration types were observed.6 Type I regeneration consisted of callus formation located only medial to the medial bone screw, Type II demonstrated callus formation both medial and lateral to the screw, and Type III showed robust callus formation with first metatarsal regeneration. Despite limited first metatarsal regeneration in 2 patients based on the criteria outlined in the Blitz and colleagues classification, these patients maintained stable fixation without evidence of hardware failure.
Overall, these findings suggest that 100% capital fragment translation in minimally invasive bunion surgery may represent a safe and effective option in appropriately selected patients, potentially offering reliable osseous healing and an acceptable complication profile.
Clinical Pearls and Surgical Considerations
- Reserve 100% translation for severe deformity. Best suited for patients with a large IM angle that cannot be corrected with a smaller capital fragment shift; when acceptable alignment is achievable with less translation, a more conservative shift is appropriate.
- Select patients carefully and discuss healing expectations. Use added caution in patients with tobacco use, diabetes, chronic steroid therapy, or prior delayed/non-union. While fixation is typically robust, counsel patients regarding the potential for prolonged healing.
- Acknowledge the learning curve and plan adjunct options. MIS bunionectomy requires fluoroscopic control, incremental correction, and formal training. Pre-consenting for a potential Akin osteotomy provides reliable supplemental correction when maximal translation alone is insufficient.
- Set expectations for postoperative radiographs and hardware. The metatarsal head position may look atypical following maximal translation; preoperative counseling can reduce concern. Use a beveled, headless screw seated flush to minimize irritation—hardware removal is generally straightforward if needed.
- Manage delayed union conservatively when present. Continue protected weight-bearing as symptoms allow and consider a bone stimulator when serial radiographs do not demonstrate progressive improvement.
Limitations of These Cases
This case series is limited by the small number of patients in whom 100% lateral translation of the capital fragment was performed. There was also variability in deformity severity across cases, as reflected by differences in preoperative hallux valgus angle (HVA) and intermetatarsal angle (IMA). Given the limited sample size, formal statistical analysis was not feasible, and outcomes are best interpreted descriptively.
We based our evaluation of union primarily on radiographs, which can see an impact by hardware obscuring the site, and may prove less sensitive than CT in some cases. We obtained advanced imaging in only 1 patient, prompted by persistent postoperative symptoms. Additionally, not all patients attended follow-up visits or obtained imaging at consistent intervals, resulting in variability in the timing of radiographic assessments.
Closing Thoughts
Overall, we feel that this case series demonstrates that MIS bunion correction with 100% translation of the capital fragment is a potentially feasible and effective option when the case requires aggressive deformity correction. With careful patient selection and attention to technique, we feel one can achieve acceptable union rates and manageable complications. Future studies with larger cohorts should further evaluate outcomes stratified by translation magnitude to better define indications, complication profiles, and functional results.
Dr. Frey is a resident at Denver Health and Hospital Authority in Denver, CO.
Drs. Gorski, Hoffman and Jerabek are attending physicians at Denver Health in Denver, CO, where Dr. Hoffman is the director of the residency training program.
The authors have no non-financial or commercial, proprietary, or financial interest in any products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
The authors disclosed that AI was used to assist with grammar, editing, and improving clarity of the manuscript; all ideas, analyses, and original writing were developed by the authors, without any AI contribution to data analysis or interpretation.
References
1. Kuhn J, Alvi F. Hallux Valgus. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2025 Jan–. Updated August 28, 2023. Accessed January 7, 2026. https://www.ncbi.nlm.nih.gov/books/NBK553092/
2. Barnes D, Matijasich P, Maxwell A, Yatsonsky D, Ballard A, Ebraheim N, Elattar O. From etiology to intervention: a holistic review of bunion pathophysiology and care. Adv Orthop. 2024;2024:9910410. doi:10.1155/2024/9910410.
3. Blitz NM. New minimally invasive bunion surgery: easier said than done. Foot Ankle Surg Tech Rep Cases. 2023;3:100288.
4. Reddy SC, Schipper ON, Li J. Biomechanical evaluation of fourth-generation minimally invasive distal first metatarsal osteotomy–Akin osteotomy technique on first ray articular contact properties. Foot Ankle Spec. 2024;17(4):406-416. doi:10.1177/19386400231184343. Epub July 6, 2023.
5. Spacek AE, Yang C, Abicht BP. Periarticular soft tissue effect following fourth generation MIS hallux valgus correction: Formation of a pyramid-shaped first metatarsal osseous healing zone. Foot Ankle Surg Tech Rep Cases. 2024;4(3):100408.
6. Blitz NM, Wong DT, Grecea B, Baskin ES. Characterization of first metatarsal regeneration after new modern minimally invasive bunion surgery: a retrospective radiographic review of 172 cases. J Min Invasive Bunion Surg. 2024;1. doi:10.62485/001c.92756.
7. Siddiqui NA, LaPorta G, Walsh AL, Abraham JS, Beauregard S, Gdalevitch M. Radiographic outcomes of a percutaneous, reproducible distal metatarsal osteotomy for mild and moderate bunions: a multicenter study. J Foot Ankle Surg. 2019;58(6):1215-1222. doi:10.1053/j.jfas.2019.04.012.
8. Lonati D, Kannegieter E, McHugh D. A multi-dimensional systematic review of minimally invasive bunion surgery (MIBS). J Clin Med. 2025;14(8):2757. doi:10.3390/jcm14082757.
9. Kafagi AH, Kafagi AR, Tahoun M, Al Zareeni OT, El Aloul K, Ahmad MU, Pillai A. Comparative outcomes of minimally invasive versus open hallux valgus surgery: a systematic review and meta-analysis. Osteology. 2025;5(1):3. doi:10.3390/osteology5010003.
10. Crespo Romero E, Peñuela Candel R, Gómez Gómez S, et al. Percutaneous forefoot surgery for treatment of hallux valgus deformity: an intermediate prospective study. Musculoskelet Surg. 2017;101(2):167-172. doi:10.1007/s12306-017-0464-1
11. Gonzalez T, Encinas R, Johns W, Jackson JB III. Minimally invasive surgery using a Shannon burr for the treatment of hallux valgus deformity: a systematic review. Foot Ankle Orthop. 2023;8(1):24730114221151069. doi:10.1177/24730114221151069
12. Singh MS, Khurana A, Kapoor D, Katekar S, Kumar A, Vishwakarma G. Minimally invasive vs open distal metatarsal osteotomy for hallux valgus - A systematic review and meta-analysis. J Clin Orthop Trauma. 2020;11(3):348-356. doi:10.1016/j.jcot.2020.04.016
13. Grecea B, Blitz NM. Pseudobunion: a new unfortunate result after new minimally invasive bunion surgery. A retrospective radiographic review and case series of 17 feet. Foot Ankle Surg Tech Rep Cases. 2025;5:100521.