Symptomatic Os Cuboideum Secundarium in a High-Risk Foot: A Rare Anatomical Variant with Clinical Consequences
A rare accessory ossicle, the os cuboideum secundarium, is typically an incidental finding—but in high-risk feet, it can become clinically significant. This case highlights how an unrecognized plantar-lateral bony prominence contributed to ulceration in a patient with diabetes, neuropathy, and cavovarus deformity. The report underscores the importance of identifying uncommon anatomical variants when evaluating atypical pressure-related wounds.
Key Takeaways
- Rare anatomy can have real clinical consequences
Although os cuboideum secundarium is exceedingly uncommon and often asymptomatic, it can act as a focal pressure point leading to pain or ulceration. - High-risk foot types amplify minor structural abnormalities
In patients with diabetes and cavovarus alignment, even small plantar-lateral prominences can create sufficient localized pressure to cause skin breakdown, especially when protective sensation is lost. - Recognition prevents misdiagnosis and guides management
Identifying this ossicle on imaging helps differentiate it from fractures or soft-tissue masses and supports appropriate treatment—typically conservative offloading first, with surgical excision reserved for persistent or recurrent symptoms.
Introduction
Accessory ossicles of the foot are common anatomic variants and are typically incidental findings, yet a small subset are exceedingly rare and poorly understood. Among them, the os cuboideum secundarium is one of the rarest, with only a handful of documented cases described in the medical literature. The ossicle is typically located plantar or plantar-lateral to the cuboid and may articulate with the cuboid, calcaneus, or the base of the fifth metatarsal, depending on its developmental origin.1 Due to its rarity, the true prevalence is unknown, and most clinicians will never encounter a symptomatic case in practice.
To date, the literature includes only a small number of imaging-confirmed symptomatic cases. In 1996, Logan and colleagues described one of the earliest clinical and radiographic accounts, reporting a patient with lateral column pain associated with this accessory ossicle.2 Gaulke and Schmitz (2003) published a case involving a surgically excised “free os cuboideum secundarium,” noting its potential to mimic a fracture and cause persistent pain.3 Kauffmann and Stacy (2014) presented a case in which magnetic resonance imaging (MRI) helped identify the ossicle and emphasized its ability to simulate a soft-tissue mass or neoplasm on advanced imaging.4 More recently, Vermeulen and team (2023) reported an additional case from a radiology perspective, reinforcing its rarity and variable presentation on cross-sectional imaging.1 Collectively, these cases demonstrate that although the ossicle is benign, it has meaningful potential to become symptomatic under the right biomechanical circumstances.
In high-risk feet, particularly those with cavovarus deformity, plantar fat pad atrophy, neuropathy, or diabetes, even small structural prominences may generate pathologic pressure. Patients with neuropathy lose the ability to detect early callus formation or focal overload, increasing the risk of skin breakdown. Therefore, a plantar-lateral ossicle such as the os cuboideum secundarium can function as a pressure point capable of precipitating ulceration.
Despite these biomechanical implications, no published reports to date have described os cuboideum secundarium as a contributor to diabetic plantar ulceration, making this case uniquely important. This report expands on the extremely limited body of literature by illustrating how a rare accessory ossicle, combined with cavovarus foot structure and neuropathy, produced a focal pressure-related ulceration in an elderly diabetic patient. Improved recognition of this ossicle may prevent misdiagnosis, avoid unnecessary workup for fracture or mass, and guide both conservative and surgical management strategies in high-risk populations.
Case Presentation
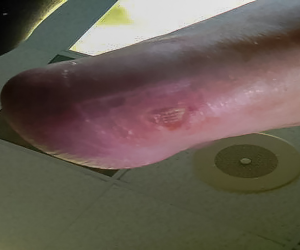
An 80-year-old male presented with a bony prominence on the right lateral plantar foot associated with an ulcer that developed after self-treatment of a callus. About a month before he established care in our clinic, the patient had used a pumice stone for callus reduction and inadvertently created a wound. The patient was evaluated by his primary care provider approximately one week after the new wound developed. Recognizing the need for specialized management, his PCP initiated a referral to podiatry. The patient had recently been issued new diabetic shoes and custom inserts through the Veterans Affairs system. He denied fevers, chills, or other systemic symptoms.
His history included type 2 diabetes mellitus (non–insulin-using), peripheral neuropathy, hypertension, hyperlipidemia, prior ST-segment elevation myocardial infarction (STEMI), transient ischemic attach (TIA), osteoarthritis, and onychomycosis. Surgical history included coronary artery bypass with graft (CABG), bilateral cataract extraction, cholecystectomy, hernia repair, bilateral carpal-tunnel release, colonoscopy, and percutaneous coronary intervention (PCI). He was married, retired, a lifelong nonsmoker, and non-alcohol user.
The clinical examination revealed palpable dorsalis pedis and posterior tibial pulses with brisk capillary refill and no edema. Neurologically, the patient demonstrated diminished light touch, vibratory sensation, and loss of protective sensation bilaterally. Dermatologic assessment showed a nearly healed ulcer at the right plantar-lateral fifth metatarsal base measuring 0.6 × 0.5 × 0.1 cm, with newly epithelialized tissue and no signs of drainage, malodor, or infection. Musculoskeletal evaluation revealed a bilateral cavovarus foot structure, decreased plantar fat pad, tailors bunionette prominence, hammertoe deformities, and a palpable bony prominence at the fifth metatarsal base, more pronounced on the right.
Right foot radiographs demonstrated a well-corticated, irregular accessory ossicle located plantar-lateral to the cuboid and proximal to the fifth metatarsal base, characteristic of os cuboideum secundarium. The ossicle corresponded directly to the area of ulceration. The ossicle measured 14mm x 18.7mm x 16.4mm (Figures 1-3).



We recommended conservative treatment due to the progressive healing of the ulcer, instructing the patient to continue offloading, use accommodative orthotics, and wear his VA-issued diabetic footwear. An accommodative orthotic was fabricated with a recessed offloading pocket beneath the bony prominence from the os cuboid secundarium, supplemented by lateral column cushioning, a soft lateral flange, and intrinsic posting to redistribute plantar pressures. Stance and gait evaluation demonstrated lateral column overload during midstance and propulsion, guiding the orthotic design to reduce shear and focal pressure over the symptomatic os cuboideum prominence. We discussed surgical excision of the ossicle and underlying bony prominence, but deferred until future need.
Important Notes and Lessons Learned
The os cuboideum secundarium is among the rarest accessory ossicles, with extremely limited documented clinical presentations.4 Although commonly incidental, symptomatic cases may result from repetitive trauma, lateral column overload, tendon irritation, or pressure from footwear.3 In patients with neuropathy and/or diabetes, even a small plantar-lateral prominence may precipitate ulceration. In this case, the patient’s cavovarus foot type, fat pad atrophy, and neuropathy set the stage for elevated lateral column plantar pressures; the os cuboideum secundarium created a focal prominence aligned with the ulcer location.
Radiographically, one expects a well-corticated ossicle to have smooth margins, aiding differentiation from fracture fragments or heterotopic ossification.2 Computed tomography (CT) or MRI can further characterize anatomy and soft tissue inflammation when indicated.5 Here, plain radiographs sufficed, especially in light of the plan for nonsurgical management.
In our experience, treatment should be guided by symptoms. Most cases respond to offloading, accommodative footwear, and modification of pressure. When persistent ulceration, pain, or tendon irritation occurs, surgical excision has been described with good outcomes.3 In this patient, conservative treatment was successful, given the healing status of his ulceration. This case therefore expands the limited literature by documenting os cuboideum secundarium as a contributor to diabetic ulceration; an association not extensively described. The patient ultimately achieved complete wound closure, and recurrence has thus far been avoided through consistent use of accommodative orthotics designed to offload areas of high plantar pressure.
Conclusion
Os cuboideum secundarium, although exceedingly rare, can serve as a clinically significant biomechanical stress point, particularly in patients with neuropathy, cavovarus foot structure, fat pad atrophy, or other conditions that increase lateral column loading. As demonstrated in this case, even a small accessory ossicle can become a focal source of pressure sufficient to precipitate plantar ulceration in high-risk individuals. Early recognition of this anatomic variant is essential when evaluating unexplained plantar-lateral wounds, recurrent callus formation, or localized pain, especially when these findings do not correlate with the more common etiologies of diabetic foot ulceration.
Conservative measures such as targeted offloading, accommodative diabetic footwear, and close wound monitoring may effectively prevent recurrence once identified; however, surgical excision becomes a consideration when conservative strategies fail or when the prominence repeatedly contributes to skin breakdown. Beyond the individual patient, this case broadens the limited body of literature on os cuboideum secundarium and underscores the need for heightened clinical awareness of rare ossicles that may influence plantar pressure patterns. By integrating anatomical variants into the differential diagnosis of lateral plantar ulcerations, clinicians can better tailor treatment, reduce complication risk, and optimize limb preservation in vulnerable populations.
Disclosures
The authors disclose that artificial intelligence (AI)–based tools were used in the preparation of this manuscript solely to assist with literature organization, language refinement, and reference formatting. All clinical interpretation, conceptual synthesis, and editorial oversight were performed by the authors. Human review and responsibility for accuracy, integrity, and originality were maintained throughout.
The authors also share that they have no non-financial or commercial, proprietary, or financial interest in the products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
Dr. Evensen is a podiatric surgeon and wound-care specialist at Golden Valley Memorial Healthcare in Clinton, MO. Dr. Evensen is actively engaged in clinical research, multidisciplinary team development, and advocacy for psychosocially informed foot and ankle care.
Jaime Moore is an adult gerontology nurse practitioner at Golden Valley Memorial Healthcare.
References
- Vermeulen A, Gupta N, Döring S. Os cuboideum secundarium: a rare accessory ossicle in the foot. J Belg Soc Radiol. 2023;107(1):19. doi:10.5334/jbsr.3043.
- Kauffmann G, Stacy GS. Os cuboideum secundarium: A rare accessory ossicle with the potential to mimic a mass on magnetic resonance imaging. Skeletal Radiol. 2014;43(1):95-98. doi:10.1007/s00256-013-1709-1.
- Gaulke R, Schmitz HG. Free os cuboideum secundarium: a case report. J Foot Ankle Surg. 2003;42(4):230-234. doi:10.1016/S1067-2516(03)70034-9.
- Logan PM, Connell DG, Janzen DL. Painful os cuboideum secundarium. Cross-sectional imaging findings. J Am Podiatr Med Assoc. 1996;86(3):123-125. doi:10.7547/87507315-86-3-123.
- Aparisi Gómez MP, et al. Anatomical variation in the ankle and foot: from incidental finding to inductor of pathology. Part II: mid-foot and fore-foot. Insights Imaging. 2019;10:69. doi:10.1186/s13244-019-0747-1.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.