Advances in Charcot Neuroarthropathy Surgical Techniques
Charcot neuroarthropathy remains a limb-threatening condition, but evolving surgical strategies are shifting the focus from rigid fixation to functional limb preservation. Emerging techniques—such as the “flipper foot” construct and selective joint fusion—aim to balance stability with controlled motion, improving durability, reducing recurrent breakdown, and enhancing patient mobility.
Key Takeaways
- Early recognition and coordinated care are still foundational—but surgery has evolved. Prompt diagnosis, immobilization, and optimization of comorbidities (especially diabetes) remain critical. However, once stabilized, patients now benefit from more nuanced surgical approaches that go beyond traditional rigid reconstruction.
- Rigid fixation alone may contribute to recurrent failure in neuropathic feet. Historically, aggressive fusion and fixation aimed to create a braceable, stable foot—but often at the cost of increased mechanical stress and risk of subsequent Charcot events. Neuropathic patients may not tolerate overly rigid constructs due to altered load distribution.
- “Flipper foot” and motion-preserving constructs can improve function and limb salvage. Newer techniques that fuse the hindfoot while preserving midfoot motion help reduce stress, prevent reulceration, and maintain functional gait. These approaches, combined with staged healing and bracing, represent a meaningful advancement in long-term outcomes and quality of life for patients with Charcot neuroarthropathy.

Charcot neuroarthropathy (CN) is a challenging complication that occurs in patients with neuropathy, often from diabetes mellitus. CN is a noninfectious condition resulting in structural collapse of bones and joints, with subsequent deformities (Figure 1). These deformities result in abnormal pressure points at risk for ulceration. Due to the loss of protective feeling, these ulcerations can become infected, leading to osteomyelitis. Historically, patients who developed CN often underwent primary leg amputation due to complications with conservative and surgical treatments. Previously, delayed diagnosis, limited treatment options (especially surgical), and potentially less effective medical management of underlying conditions like diabetes mellitus contributed to poor outcomes. The risks of progression to severe deformity, ulceration, infection, and amputation were significant. Even after surgical reconstruction, deformities can persist, which makes bracing challenging. With significant partial foot and leg amputations, life expectancies are lower for patients with this condition. Based on 2005 data, above- and below-knee amputation mortality rates range from 13-40% in the first year, 35-65% in 3 years, and 39-80% in 5 years.1
Advances in the podiatric profession have made strides in managing complications stemming from CN. Early recognition is paramount. A red, hot, and swollen foot in a patient with numbness is usually a late-stage clinical finding suggesting the process has already begun. Early intervention involves immobilization and non-weight-bearing. Coordinating medical care with their primary physician or endocrinologist to improve diabetes control is also essential. Once medically stabilized, surgical intervention may become a consideration to help stabilize the fractures and deformities that arise from CN. Previously, stabilization with screws and plates would aggressively hold the foot and ankle in a straight position for effective bracing. However, due to the nature of neuropathy, the increased stress from a rigid foot which is normally meant to move cannot accommodate these forces and may result in another Charcot event. In this article, we will discuss a newer approach to limb salvage for patients with CN to create a more functional foot that we feel may have improved longevity compared to previous paradigms.
The flipper foot construct is a Charcot reconstruction strategy that combines rigid hindfoot fusion with preserved or renewed midfoot motion, creating a controlled, functional lever arm that aims to reduce stress and improve long-term limb durability.2 In practice, this involves stabilizing the hindfoot, often through procedures such as tibiocalcaneal or tibiotalocalcaneal arthrodesis using intramedullary fixation, to correct deformity and provide a stable base, while deliberately avoiding or reversing fusion in the midfoot to maintain a motion segment. This preserved mobility, sometimes enhanced through osteotomy or joint “unlocking,” allows controlled sagittal plane movement at joints like the talonavicular, producing a rocker-like or “flipper” effect during gait. By balancing stability with flexibility, this construct reduces abnormal pressure distribution seen in fully rigid reconstructions, helping to minimize recurrent ulceration, prevent additional Charcot events, and improve overall function and brace tolerance in high-risk patients with neuropathy.
Details of Representative Cases
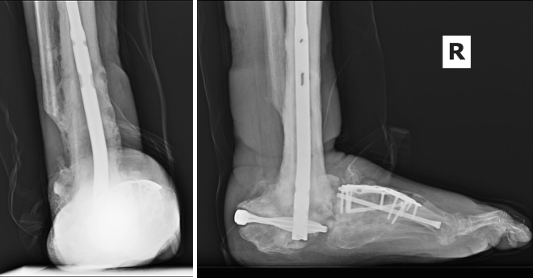
To illustrate the pitfalls of CN treatment, we present a 61-year-old male who already underwent midfoot fusion for a prior diabetic Charcot event (Figure 2). He came in for a second opinion 6-months after index procedure, as he had declined an ankle fusion, wanting to preserve his motion so that he could drive. A second set of radiographs demonstrate attempted hindfoot fusion that resulted in collapse to the talus bone in the ankle joint (Figure 3).
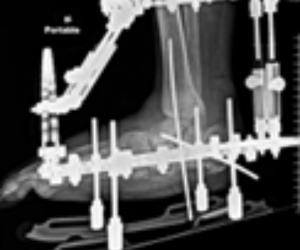
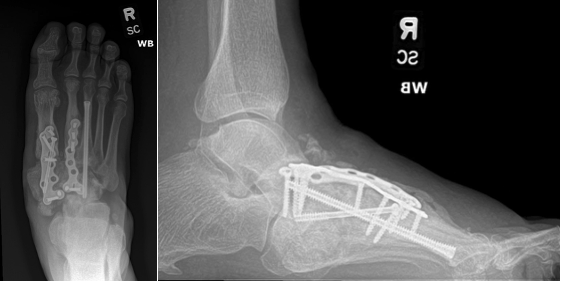
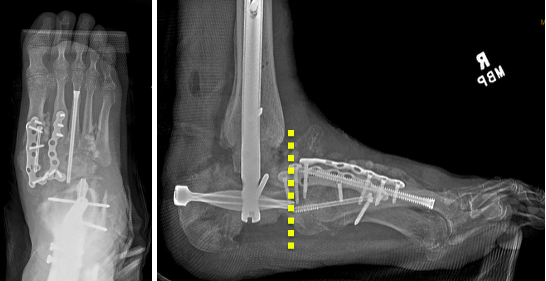
Recent podiatric research has revealed an alternative treatment option to the traditional rigid fixation. As mentioned, the Charcot flipper foot construct involves fusing the hindfoot while leaving the midfoot mobile, to allow for some motion, lowering risk of further breakdown.2 The final surgery replaced the dislocated talus with a cadaver bone and fused the hindfoot with an intramedullary nail, all through small incisions for preparation and hardware fixation. The midfoot screws added in his second surgery were removed and a midfoot osteotomy with a plantar-based wedge allowed the forefoot to plantarflex relative to the hindfoot for sagittal plane correction and recreate a plantigrade foot (Figure 4). Dynamization of the intramedullary nail began around 3 months postop to assist with bone healing. Postoperatively, patients used a Charcot restraint orthotic walker (CROW) boot until the hindfoot allograft showed sufficient consolidation at 5 months (Figure 5). He is now ambulating in a TayCo brace to allow for forefoot motion. He will be braced for 18-months postoperatively to ensure full osseous consolidation before a re-evaluation as to whether hindfoot bracing is still needed.
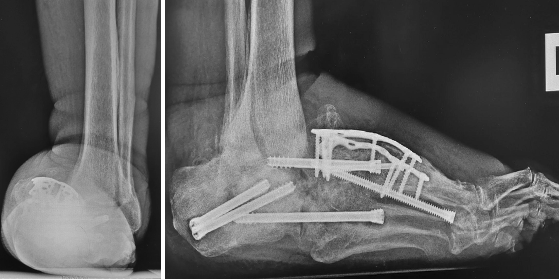
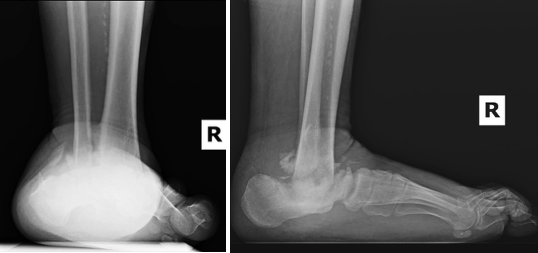
There can be severe chronic deformities that occur after acute trauma with concomitant CN. We evaluated a 47-year-old male with a left below-knee amputation, diabetes mellitus, peripheral neuropathy, and end-stage renal disease requiring dialysis. The patient sustained a right ankle fracture a year ago, initially treated conservatively due to his multiple comorbidities. Immobilization took place with a high-tide cast boot, but he ulcerated at the medial ankle due to the lateral subluxation of the foot. The patient transitioned to regular shoes and used a knee scooter to maintain non-weight-bearing. The resulting deformity was an unstable ankle with a laterally shifted foot relative to the long axis of the leg (Figure 6). The patient underwent a talectomy and tibiocalcaneal arthrodesis with an intramedullary nail (Figure 7). The flipper foot technique can be implemented for patients that undergo talectomy and tibiocalcaneal arthrodesis. With resection of the talus, a motion segment anterior to the ankle forms at the pre-existing talonavicular joint. This creates a more functional gait pattern and helps to lessen stress to the midfoot that may result in another Charcot event.2 The patient ambulated in a removable boot 3 months postoperatively, by which time, the medial ulceration had healed. The patient demonstrated a plantigrade hindfoot with motion through the tibionavicular joint (click here for video). We accommodated his limb length discrepancy height adjustment to his contralateral prosthesis.

Conclusion
Charcot neuroarthropathy is a devastating condition with significant risk factors for limb loss. Podiatric surgical advances have been able to improve limb salvage rates and restore function. With the continued evolution of podiatric surgical treatment, patients with this condition have better prognosis and functional status than in the past so that they can be productive members of society.
Dr. Husain is the program director of the McLaren Oakland Hospital Podiatric Medicine and Surgery Residency Program and in private practice in Rochester, MI with Great Lakes Foot and Ankle Institute.
Drs. Garbis and Lawton are PGY3 residents at the McLaren Oakland Hospital Podiatric Medicine and Surgery Residency Program.
Disclosures
The authors have no non-financial or commercial, proprietary, or financial interest in the products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
References
1. Singh N, Armstrong, DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005; 293(2): 217-28.
2. Loveland JD. New surgical techniques in the treatment of charcot neuroarthropathy deformities. Clin Podiatr Med Surg. 2025; 42(3): 505-19.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.