


Ankle Arthritis and TAR: Diagnosis, Instability, and Surgical Decision-Making
Ankle arthritis is a debilitating condition commonly driven by prior trauma and chronic instability, often progressing despite conservative care. As imaging limitations challenge early detection of intra-articular damage, surgical decision-making becomes increasingly nuanced. Advances in total ankle replacement are reshaping treatment paradigms, offering motion-preserving alternatives to traditional fusion in select patients.
Key Takeaways
- Post-traumatic injury drives most ankle arthritis: Up to 70% of cases stem from prior trauma, with chronic lateral ankle instability significantly accelerating joint degeneration.
- MRI may underestimate pathology: Advanced imaging often fails to detect intra-articular damage, while arthroscopy frequently reveals more extensive cartilage injury and delamination.
- TAR is emerging as a primary option: With modern implant advancements, total ankle replacement offers improved functional outcomes and motion preservation compared to arthrodesis in appropriately selected patients.
Arthritis involves inflammation of a joint and gradual breakdown of its associated structures including cartilage, bone, and the surrounding soft tissues. This condition leads to decreased mobility, pain, swelling, and significant functional impairment. The pathogenesis of arthritis varies by joint, with some cases occurring primarily over time, while ankle arthritis more often develops secondarily following traumatic injury. Post-traumatic etiologies account for approximately 70% of ankle arthritis cases, followed by rheumatological disease, acquired deformity, chronic instability, and least commonly, primary arthritis.1-2
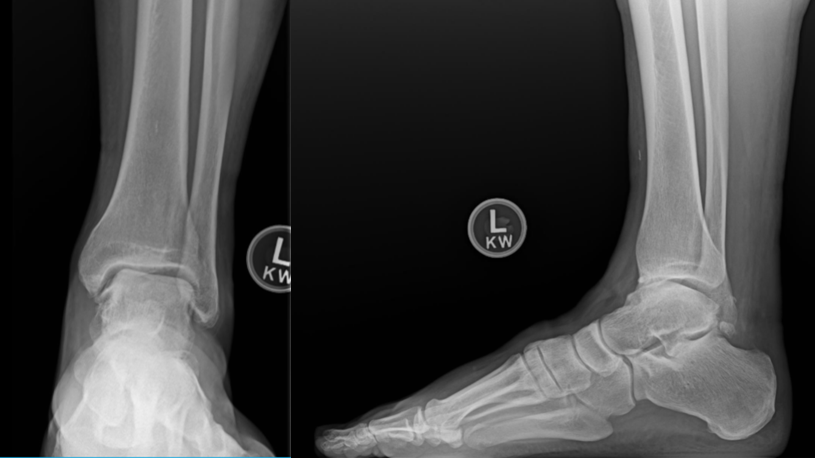
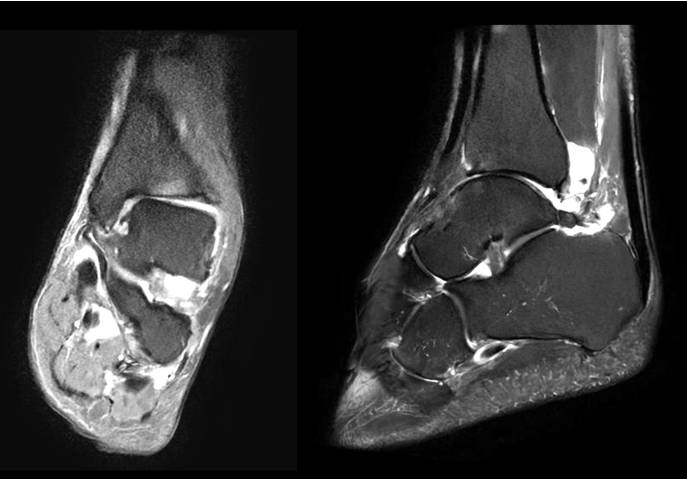
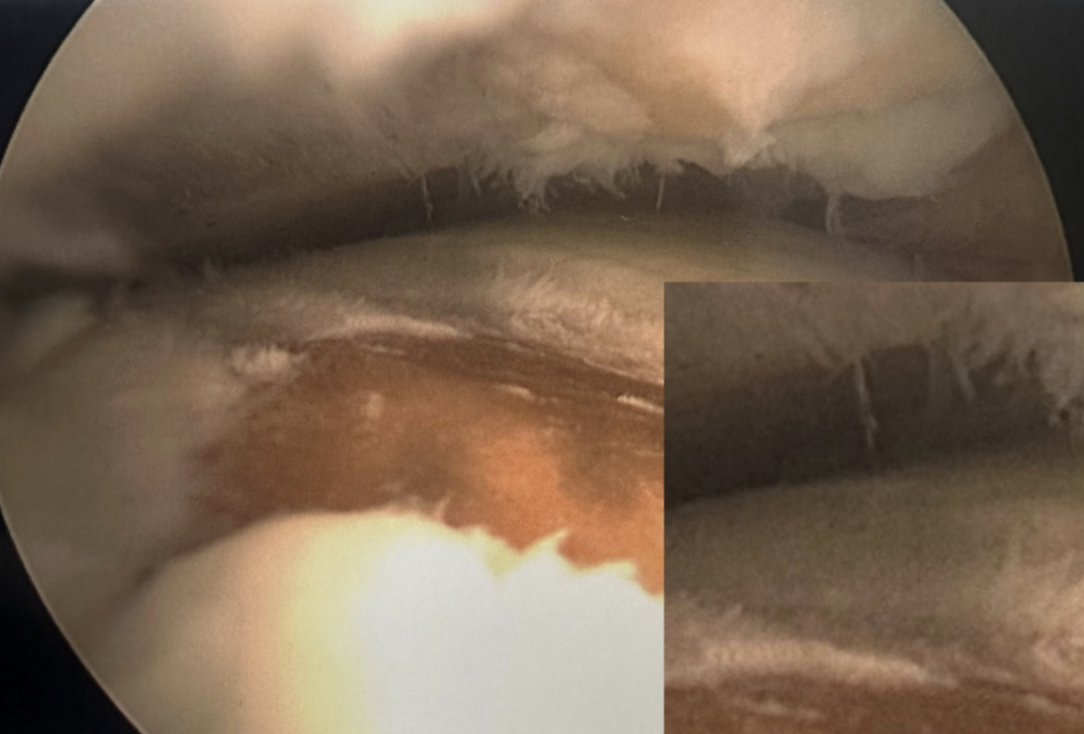
Chronic ankle instability is a frequently encountered problem in our practice. The photos shown below (Figures 1-3) illustrate a patient with chronic lateral ankle instability (CLAI) who underwent lateral ankle ligament reconstruction in conjunction with arthroscopic debridement. Despite the use of advanced imaging modalities, chronic articular and subchondral pathology is often poorly appreciated on magnetic resonance imaging (MRI). Prior studies comparing preoperative MRI with arthroscopic findings in patients with chronic lateral ankle instability have demonstrated that MRI has limited sensitivity for detecting associated intraarticular pathology.3
In contrast, intraoperative findings can clearly demonstrate extensive articular cartilage delamination associated with chronic instability and asymmetric loading of the ankle joint. Recurrent ankle sprains leading to chronic lateral instability are a well-recognized cause of post-traumatic ankle arthritis, with prior studies reporting that up to 80% of patients with chronic lateral ankle instability ultimately develop ankle arthritis.4-5
Treatment Options
Multiple conservative therapies exist to address early onset of ankle arthritis including bracing, anti-inflammatory medications, shoe gear modifications, and intraarticular injections. In patients who fail to respond to conservative management, multiple surgical options exist based on the severity of ankle arthritis as well as patient-specific factors, including comorbidities, age, activity level, and postoperative expectations.
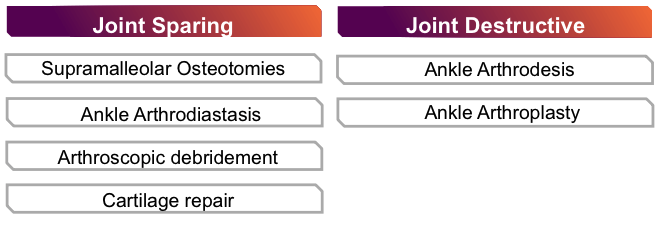
Surgical options fall into 2 broad categories including joint-sparing and joint-destructive procedures, as noted below (Figure 4). Ankle arthrodesis has been considered the standard of treatment for end-stage ankle arthritis, with several studies demonstrating the significant improvement in pain and patient-reported quality of life following fusion.6-7 However, with continued advancements in implant designs, surgical technique, and revision options, total ankle replacement has gained increased acceptance as an alternative. Replacement offers preservation of ankle range of motion and may spare the adjacent joints from compensatory straining compared with arthrodesis. Recent literature suggests that total ankle arthroplasty may provide superior functional outcomes measures and comparative revision rates to ankle arthrodesis.8-10
Surgeons generally consider total ankle replacement for patients with relatively low functional demands, sufficient bone stock, and neutral-to-minimally deformed ankle arthritis. Beyond patient-specific considerations, both deformity and osseous constraints play a key role in determining the most appropriate surgical option. Substantial subchondral osteolysis or thin cortical bone in the distal tibia can compromise implant fixation and long-term stability. This warrants careful preoperative evaluation, and in some cases, ankle arthrodesis may be the more appropriate treatment option.

Brief History of Total Ankle Replacements
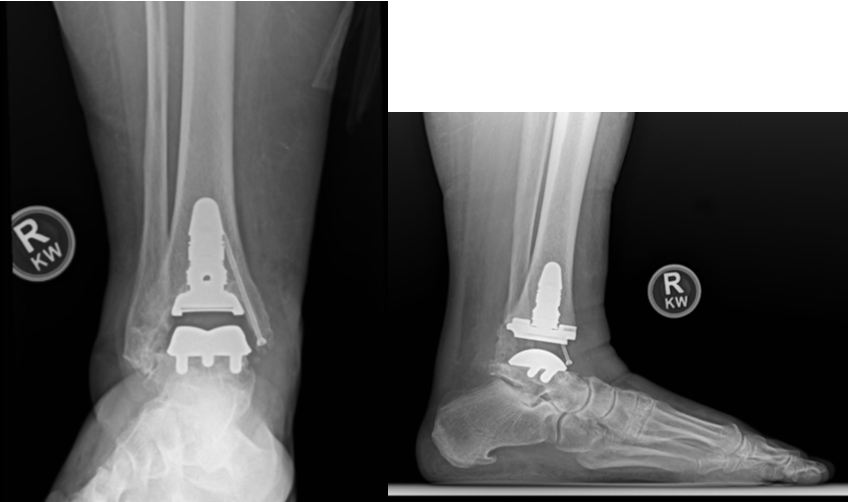
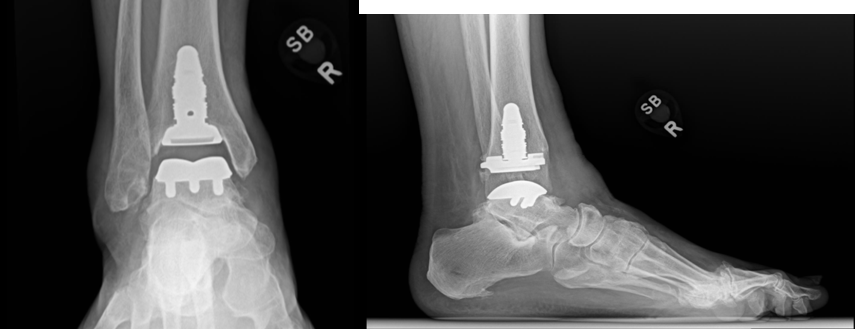
The first total ankle arthroplasty took place in 1970 by Lord and Marotte, utilizing an inverted hip stem implanted into the tibia, combined with a talectomy and a cemented acetabular cup placed within the calcaneus.11 These first-generation ankle replacements carried an association with high failure rates, persistent pain, and progressive deformity. Second-generation designs (1980s-1990s) prioritized bone-sparing cuts, cementless fixation, and in some cases included mobile-bearing constructs and/or fusion of the syndesmosis. Third- and fourth-generation TARs (2000s-present) evolved into 3-component semi-constrained systems with emphasis on minimal bone resection, patient-specific cutting guides, improved instrumentation, and component technology that mirrors native articular geometry (Figure 6). Building on these advancements, recent studies have shown that fourth-generation ankle implants achieve moderate-to-long-term survivorship exceeding 90%.12-13
Our Experience
Our institution has been at the forefront of the advancing, developing, and increasing understanding of total ankle replacement over the last 2 decades. A common procedure within our institution, our surgeons have used a variety of implant designs and maintain comprehensive data record sets to facilitate work towards continually improved patient outcomes. For the purposes of this article, while careful work-up and patient selection are critical, we provide a generalized overview of our institutional approach.
Several total ankle replacement (TAR) implant designs are currently available on the market. While each implant differs, they each generally categorize as low-profile or stemmed designs. Based on recent data and research, most TARs performed at our institution include a stemmed component. Many systems also offer patient-specific instrumentation (PSI); however, we primarily use standard instrumentation to allow precise intraoperative adjustment of bone cuts and correction, without relying on a patient-specific cutting guide. Although some studies suggest that PSI may reduce operative time while achieving similar clinical outcomes, other reports indicate that it does not improve alignment compared with standard instrumentation.9-10
Notes on the Surgical Technique
We initially assemble the leg holder on the back table for subsequent use as the external standard instrumentation (Figure 7). If the operating surgeon elects to place a prophylactic medial malleolar construct, this becomes the first step of the procedure. Fluoroscopic guidance aids the surgeon in placing a metallic or biointegrative implant (surgeon preference) into the medial malleolus, with careful attention to trajectory and length to avoid interference with the planned stemmed tibial component.

We then secure the operative extremity within the external leg holder and pin according to manufacturer specifications. Intraoperative fluoroscopy obtained in orthogonal planes confirms appropriate alignment and positioning of the reaming rod, as well as to verifies planned tibial and talar resections and component sizing. We pay meticulous attention to achieving a rectus or slightly valgus tibial resection (Figure 8). In our experience, excessively rectus cuts may result in a residual varus appearance postoperatively. We also take care to ensure that the talar flat cut is not overly aggressive and does not violate the subtalar joint. In our practice, we no longer perform chamfer cuts due to observed incidences of significant component subsidence.
Tibial and talar bone cuts subsequently take place. At this stage of the procedure, we direct meticulous attention to ensure thorough gutter debridement and removal of any residual osseous or soft tissue impingement from the resected surfaces. Tibial reaming then occurs through the external jig into the metaphysis to accommodate the selected tibial stem length. The surgeon assembles and implants the modular tibial stem and base components accordingly.
Following tibial preparation and component implantation, the surgeon removes the foot from the leg holder. Insertion of talar and polyethylene trial components allows assessment of sizing, alignment, stability, and range of motion. Final component implantation takes place according to manufacturer guidelines. The system utilized offers modularity with interchangeable components, allowing customization of stemmed constructs based on patient anatomy and surgeon preference.

Concluding Thoughts
Ankle arthritis is a debilitating condition that most commonly develops as a sequela of prior trauma. While thoroughly exhausting nonoperative treatment modalities should take place before considering surgical intervention, advancements in implant design and instrumentation over the past decade have significantly improved the durability, reproducibility, and predictability of outcomes following total ankle arthroplasty. Despite these advances, total ankle replacement remains a technically demanding procedure with complications often challenging to manage. Given the potential complexity of complications, careful oversight by experienced providers is essential. In our view, total ankle arthroplasty has evolved beyond an alternative to ankle fusion and is increasingly regarded as a primary treatment option.
Dr. Badillo is a Fellow at the Orthopedic Foot and Ankle Center in Worthington, OH.
Dr. Brandao is the Fellowship Co-Director at the Orthopedic Foot and Ankle Center in Worthington, OH.
Disclosures
The authors have no non-financial or commercial, proprietary, or financial interest in products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
References
1. Valderrabano V, Horisberger M, Russell I, Dougall H, Hintermann B. Etiology of ankle osteoarthritis. Clin Orthop Relat Res. 2009 Jul;467(7):1800-6. doi: 10.1007/s11999-008-0543-6. Epub 2008 Oct 2. PMID: 18830791; PMCID: PMC2690733.
2. Saltzman CL, Salamon ML, Blanchard GM, et al. Epidemiology of ankle arthritis: report of a consecutive series of 639 patients from a tertiary orthopaedic center. Iowa Orthop J. 2005;25:44-6. PMID: 16089071; PMCID: PMC1888779.
3. O'Neill PJ, Van Aman SE, Guyton GP. Is MRI adequate to detect lesions in patients with ankle instability? Clin Orthop Relat Res. 2010 Apr;468(4):1115-9. doi: 10.1007/s11999-009-1131-0. Epub 2009 Oct 23. PMID: 19851818; PMCID: PMC2835579.
4. Gribble PA, Bleakley CM, Caulfield BM, et al. 2016 consensus statement of the International Ankle Consortium: prevalence, impact and long-term consequences of lateral ankle sprains. Br J Sports Med. 2016 Dec;50(24):1493-1495. doi: 10.1136/bjsports-2016-096188. Epub 2016 Jun 3. PMID: 27259750
5. Hong CC, Tan KJ, Calder J. Chronic lateral ankle ligament instability - Current evidence and recent management advances. J Clin Orthop Trauma. 2023 Dec 28;48:102328. doi: 10.1016/j.jcot.2023.102328. PMID: 38274643; PMCID: PMC10806209.
6. Rajapakshe S, Sutherland JM, Wing K, et al. Health and quality of life outcomes among patients undergoing surgery for end-stage ankle arthritis. Foot Ankle Int. 2019 Oct;40(10):1129-1139. doi: 10.1177/1071100719856888. Epub 2019 Jun 19. PMID: 31215232.
7. Kohring JM, Houck JR, Oh I, Flemister AS, Ketz JP, Baumhauer JF. Pattern of recovery and outcomes of patient reported physical function and pain interference after ankle fusion: a retrospective cohort study. J Patient Rep Outcomes. 2020 May 27;4(1):40. doi: 10.1186/s41687-020-00203-y. PMID: 32462241; PMCID: PMC7253567.
8. Goldberg AJ, Chowdhury K, Bordea E, et al. Total ankle replacement versus ankle arthrodesis for patients aged 50-85 years with end-stage ankle osteoarthritis: the TARVA RCT. Health Technol Assess. 2023 Mar;27(5):1-80. doi: 10.3310/PTYJ1146. PMID: 37022932; PMCID: PMC10150410.
9. Liu J, Cho T, Arefi IA, Lawrence A, Jayasuriya AC. Total ankle arthroplasty versus ankle arthrodesis in end-stage osteoarthritis: A meta-analysis of comparative outcomes. J Orthop. 2025 Mar 27;63:157-164. doi: 10.1016/j.jor.2025.03.056. PMID: 40248053; PMCID: PMC12000697.
10. Glazebrook JM, Glazebrook HM, Glazebrook MA, Morash JG. Ankle arthrodesis or total ankle arthroplasty surgery for end stage ankle arthritis, which is best? A review of the best available evidence. Foot Ankle Surg. 2024 Jan;30(1):1-6. doi: 10.1016/j.fas.2023.08.001. Epub 2023 Aug 9. PMID: 37580181.6.
11. Colò G, Fusini F, Mazzotti A, Faldini C, Leigheb M, Surace MF. Five decades of total ankle replacement: from early failures to fourth-generation innovations and future priorities. Eur J Orthop Surg Traumatol. 2025;36(1):64. Published 2025 Dec 29. doi:10.1007/s00590-025-04634-5
12. Kostusiak M, Dahill M, Dean M, et al. 8-year survivorship of a 4th generation fixed bearing total ankle replacements. Foot Ankle Orthop. 2024 Dec 19;9(4):2473011424S00106. doi: 10.1177/2473011424S00106. PMCID: PMC11660248.
13. Basile P, Manning E, Miner S, et al. Total ankle arthroplasty survivorship: a meta-analysis. J Foot Ankle Surg. 2020; 59(5):1040–1048. https://doi.org/10.1053/j.jfas.2019.10.011
14. Arceri A, Abdi P, Mazzotti A, et al. Standard total ankle arthroplasty vs. patient-specific instrumentation: a comparative study. J Personalized Med. 2024; 14(7):770. https://doi.org/10.3390/jpm14070770
15. Jones CH, Boden A, Friedmann P, et al. Patient-specific instrumentation does not improve alignment compared to the extramedullary foot holder for the INBONE II total ankle arthroplasty. Foot Ankle Int. 2025 Nov;46(11):1207-1217. doi: 10.1177/10711007251353787. Epub 2025 Jul 24. PMID: 40703039.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.





