


Shining a Light on Payer Management in Medical-Benefit Oncology: A Call for Action to Prioritize Patient Care
Abstract
Cancer treatment decisions should be made by patients and their oncology care teams, informed uniquely by tumor biology, disease stage, prior therapy, comorbidities, and patient preferences—not constrained by coverage rules. Utilization-management approaches, traditionally associated with other therapeutic areas, are increasingly applied to medical-benefit oncology, leading to treatment delays, added administrative burden, and barriers to evidence-based care. This report describes how payer management in oncology is evolving, why the current environment is worsening, the impact to patients and practices, and the policy changes needed to protect timely access and physician-led decision making in cancer care.
Evolution of Payer Management in Oncology—And What Has Changed
Historically, oncology (particularly medical-benefit, physician-administered drugs) was viewed as a therapeutic area where payers applied comparatively less active management due to the seriousness and complexity of cancer care. While payers have historically managed pharmacy benefit oncology drugs, more recently, physician-administered medical benefit oncology drugs are being managed and frequently subject to prior authorization and related controls. These processes can delay access to life-saving therapies and add administrative friction that diverts practice resources from patient care. Today, however, cancer drug spending has become the top spending category for both commercial insurers and Medicare managed care in the United States, with total cancer costs projected to reach approximately $246 billion by 2030,1,2 and cancer drugs representing 50% to 60% of total oncology care spend.3 This environment has driven payers to adopt tighter formularies and expand prior authorization and step-edit policies (including fail-first step therapy). These measures can shift decision-making away from oncology teams and toward administrative criteria that may trail behind the current evidence base. Recent payer actions illustrate this shift, including new medical policies for programmed cell death protein 1 (PD‑1) and programmed death‑ligand 1 (PD‑L1) inhibitors in lung cancer. Such policies signal that even foundational and fast-evolving oncology categories may face tighter utilization controls.
Why Payer Management Is Increasing: A Rapidly Evolving and Costly Treatment Landscape
Oncology payer management is increasing and is expected to intensify as treatment options expand and costs rise. Despite the investment in developing innovative therapies, payers are increasingly focused on cost-containment efforts through tighter formularies, prior authorizations, and step edits (including fail-first step therapy). This shift carries significant risks by threatening to place critical treatment decisions in the hands of payers rather than the patient’s dedicated oncology care team, potentially causing treatment delays without guaranteed access to personalized medicines and negatively affecting community oncology. These pressures also extend beyond drug access to key components of contemporary oncology care, such as imaging and biomarker testing, which can further complicate and delay the path from diagnosis to treatment selection. Community oncology—which delivers 60% of oncology care— faces a disproportionate strain because many clinics have fewer resources to absorb administrative workload and reimbursement pressures.
Patients with Medicare Advantage (MA) plans or commercial coverage often face the greatest coverage challenges. Whereas Medicare fee-for-service (FFS) generally provides open access to oncology drugs, MA plans function more like commercial insurance, by selecting preferred drugs and using utilization-management techniques to manage access.4,5 As more patients age into Medicare, and as more beneficiaries elect MA plans over FFS, an even larger portion of Medicare patients will face restrictive management policies.6 Additionally, as cancer diagnoses rise among younger Americans, many of whom are covered by commercial plans, payer management strategies will increasingly affect these patients as well. Looking ahead, the shift toward greater control over medical-benefit drugs is expected to intensify, further complicating access to life-saving treatments and ultimately worsening patient outcomes.
A medical oncologist from a large, network-affiliated community oncology practice noted, “Prior authorization is onerous and difficult to implement. Very commonly, the treatment decision for a patient has to change once it goes through the prior authorization process, especially for supportive care drugs.”
Medicare FFS enrollment is declining while MA enrollment is increasing, accounting for over 50% of the Medicare population.7 This trend will likely accelerate as standalone prescription drug plans exit the market and MA plans continue to offer benefit structures that attract more patients.
Implications of Payer Utilization Management and Why Patient Autonomy Matters in Oncology
Time is clinically meaningful in oncology. Delays can be critical and prompt intervention is essential for optimal outcomes, as several studies have identified that delayed care is associated with increased mortality risk.7-9 The autonomy of oncology clinicians is not a preference but a safeguard. Cancer treatment decisions often require nuanced interpretation of evolving evidence and individualized risk–benefit tradeoffs based on the patient’s disease biology, treatment history, comorbidities, and goals. When payer policies diverge from current clinical standards or are applied rigidly, they may force changes to treatment plans, delay treatment initiation, and erode trust in the doctor–patient relationship.
Study Partnership and Survey Methods
To better understand the current state of payer management from an oncology perspective, Florida Cancer Specialists & Research Institute (FCS), Florida’s largest community oncology provider, worked with Avalere Health to conduct national market research with oncology providers across the US. FCS treats more than 1.1 million patients annually across nearly 100 locations. As a physician-owned and led practice, FCS prioritizes patient well-being, ensuring that medical decisions are driven by expertise, ethics, and evidence-based care.
In collaboration with FCS, Avalere Health developed and conducted a survey in May 2025 focused on oncology drug management trends, utilization management techniques, experiences with utilization management, and patient implications. Seventy-five respondents completed the survey, including 57 medical oncologists, 8 oncology pharmacists, 9 practice administrators, and 1 oncology nurse. Respondents were geographically diverse and represented both community oncology practices and hospital-, health system–, or academic-affiliated oncology practices. The survey excluded integrated delivery networks, defined as an institution where an organization owns and operates a network of multiple health care facilities with an internal payer system.
Survey Findings
Provider Perceptions: What Physicians Are Experiencing
Respondents reported frequent misalignment between health plan criteria and the preferred treatment plan, describing that for patients covered under commercial or MA plans, the plan criteria differed from the physicians’ preferred treatment plan most of the time (Figure 1). Community oncology respondents reported that MA plan criteria differed from their preferred treatment plan more often than commercial plans (24% vs 8%, respectively), while hospital/health system practices reported similarity between payer types. Although community practices reported commercial plan misalignment to be less, they reported commercial criteria differed “sometimes” 68% of the time, on average.
How often are health plans’ criteria different from your preferred treatment plan?
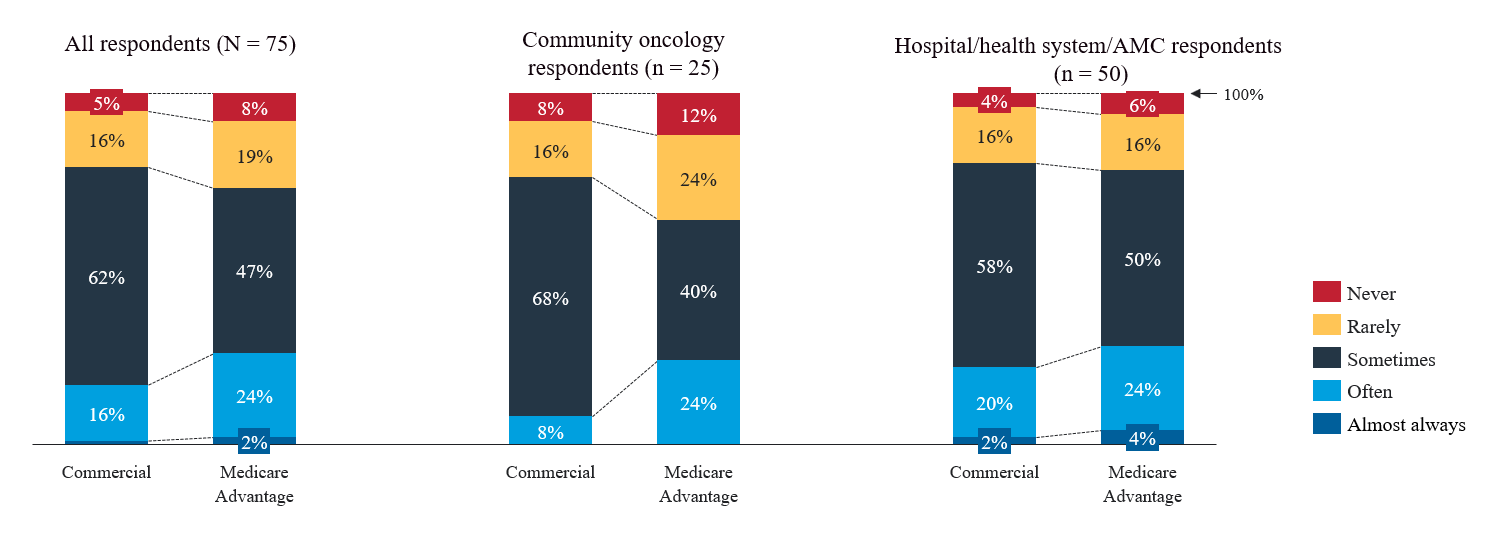
Data were derived from an Avalere Health survey of 75 geographically diverse oncology physicians, nurses, pharmacists, and practice administrators.
Abbreviation: AMC, academic-affiliated medical center.
aReproduced with permission from Avalere Health.
Oncology policies are often shaped without input from oncologists, resulting in a lack of clinical expertise needed to make informed decisions tailored to a personalized care plan.10 When physicians are required to complete a peer-to-peer review with a payer, they are constrained by the plan’s scheduling availability, sometimes even compelled to leave other patients’ appointments to complete the call. These peer-to-peer reviews are also rarely conducted with oncologists, which often means oncologists must defend their treatment decisions to individuals unfamiliar with oncology, standards of care, and the individual needs of their patient. As one medical oncologist interviewed about utilization management noted, “Less than 20% of the time I’m speaking to an oncologist in a peer-to-peer discussion. These calls are rarely useful…” Figure 2 summarizes how often 59 oncology providers described speaking with an oncologist during a peer-to-peer review: 80% of respondents said they speak with an oncologist “never” (7%), “rarely” (41%), or “sometimes” (32%).
How often is the person with whom you speak during a peer-to-peer review an oncologist?
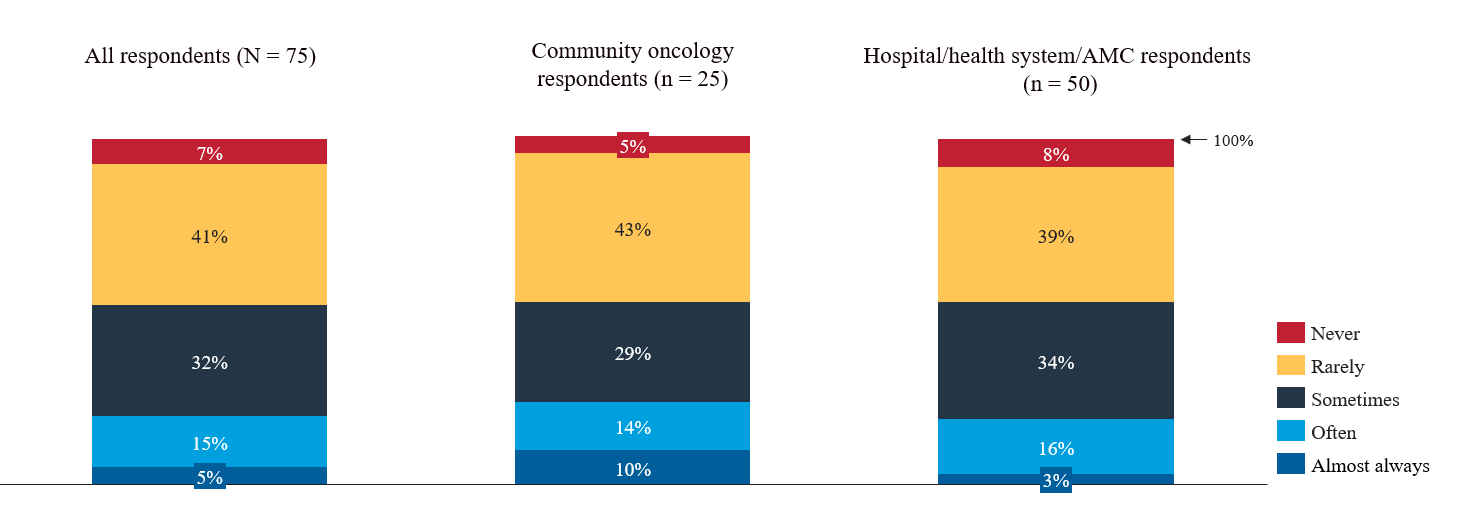
Data were derived from an Avalere Health survey of 75 geographically diverse oncology physicians, nurses, pharmacists, and practice administrators.
Abbreviation: AMC, academic-affiliated medical center.
aReproduced with permission from Avalere Health.
Prior authorization requirements for physician-administered drugs are common, and denials occur in about one-quarter of claims. Community oncology providers reported that 29% of prior authorizations for physician-administered drugs are denied on the first submission, and 28% are denied after 2 or more submissions. The most common reasons for prior authorization denials include drug non-coverage (68%), unmet step-edit criteria (60%), and the patient not meeting coverage criteria (60%). When prior authorization is denied, providers may continue to pursue the preferred drug through an appeal (including a peer-to-peer review) or medical exception process. These options delay access to care and act like bureaucratic red tape that oncology providers and patients face when trying to select the best treatment option.
As illustrated in Figure 3, most respondents reported that their practice always appeals prior authorization denials; however, when they do not appeal, the most common reason is that the patient cannot afford to wait to initiate treatment.
In the event of PA denial, which of the following is a common reason that you do not appeal the denial?
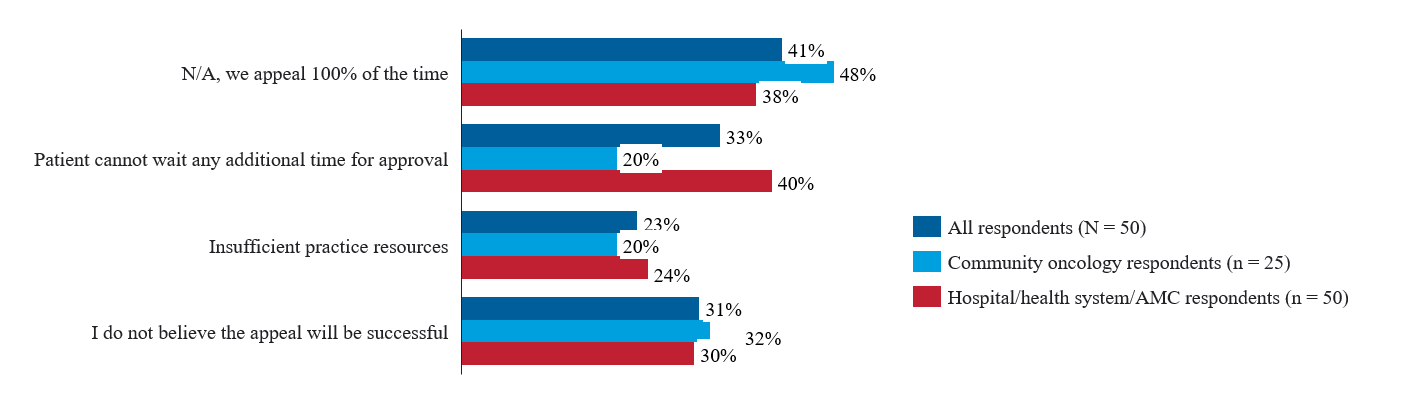
Data were derived from an Avalere Health survey of 75 geographically diverse oncology physicians, nurses, pharmacists, and practice administrators.
Abbreviations: AMC, academic-affiliated medical center; N/A, not applicable; PA, prior authorization.
aReproduced with permission from Avalere Health.
Respondents’ views on increased medical exceptions and peer-to-peer reviews were similar between community oncology and hospital/health system practice respondents (Figure 4). While slightly more hospital-based practices describe undertaking medical exceptions than community oncology practices (56% vs 48%), this may be possible given the greater administrative staff and resources available to these practices. Community practices face a higher rate of prior authorization denial on the second submission than hospitals (28% vs 17%). Although community practices appeal prior authorization denials more often, they may not be able to engage in the medical exception process as often as hospitals due to the increased time requirement. Community oncology respondents also described a slightly greater increase in peer-to-peer reviews (57%) than hospital-based practices (55%).
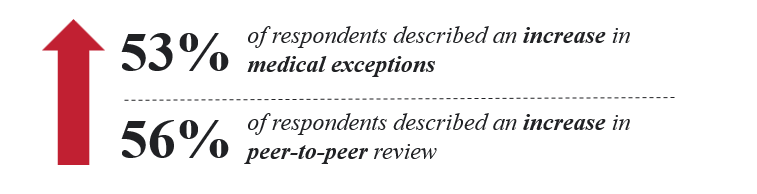
Data were derived from an Avalere Health survey of 75 geographically diverse oncology physicians, nurses, pharmacists, and practice administrators.
aIncrease in medical exceptions and peer-to-peer review is relative to the past 3 years.
bReproduced with permission from Avalere Health.
In a recent American Medical Association (AMA) survey, 77% of physicians reported that prior authorization has led to ineffective initial treatments.11 Utilization-management practices in oncology can delay and undermine patient care, especially when timely intervention is critical. Patients facing cancer cannot afford to navigate through bureaucratic red tape to receive the timely treatment they need.
The Medical Exception Process Is Time-Consuming and Not Guaranteed
Although payers may justify their use of utilization-management practices by stating that access to nonpreferred drugs or treatments can be pursued on a case-by-case basis, the reality is far more complex. It creates a dangerous situation in which a patient’s disease continues to progress while they must fight for access to potentially life-saving treatments. In the battle against cancer, time is not just precious—it’s a matter of survival. If a medical-benefit drug is not covered by a plan, physicians may initiate the medical exception process, which is time-consuming and does not guarantee a favorable outcome. Survey respondents described that most medical exceptions take up to 1 hour (57%), with some taking up to 2 hours (17%).
The AMA survey reported that, across therapeutic areas, 53% of physicians do not appeal denials because their patient cannot wait for the health plan to approve the prior authorization, which may result in treatment that is inconsistent with the current standard of care.11 In our survey of oncologists, this response was very similar, with 52% of respondents noting they do not undergo medical exceptions because the patient cannot wait for approval. Nearly 60% of our survey respondents reported the average delay in treatment is 1 to 2 weeks, and 20% reported patients face a 3- to 4-week delay, on average.
Impact of Formulary Exclusions in Oncology
Formulary exclusions are becoming increasingly common among commercial and MA plans, with an ever-growing number of cancer treatments excluded from coverage. According to a 2021 IQVIA report, there were 60 oncology formulary exclusions, 34 of which were due to the availability of a branded preferred alternative.12 Since this report, payers have faced increased liability and are seeking ways to manage costs associated with the greater number of patients with cancer and the evolution of the treatment landscape. As a result, the number of exclusions has likely grown since 2021 and will likely continue to increase.
Under the Inflation Reduction Act, plans will face increased liability for Medicare beneficiaries. This pressure will increase plans’ use of utilization management and likely increase beneficiary cost sharing, both of which can have negative consequences for patients.13
When patients cannot access the treatments their physicians and care team consider most appropriate, they may be forced to switch to alternative medications, which may be less effective or pose more severe side effects. Payer management strategies that favor their preferred drugs over the physician’s recommended drug often put patients in an agonizing position: choosing between the best therapy clinically recommended and the one they can afford, due to differences in cost-sharing between preferred and nonpreferred drug tiers. It is likely that pharmacy-benefit management techniques will expand into medical benefits, driven by such factors as growing innovation in high-cost specialty drugs, increasing regulatory scrutiny of affordability and access, and growing patient advocacy efforts aimed at reducing barriers to access.14
The way payers manage oncology treatment coverage has profound implications for patient outcomes. For example, payers have imposed coverage limits in the past on oral antiemetics, which many patients with cancer rely on as part of their anti-chemotherapy treatment regimen, even when the patient’s physician has prescribed a higher quantity.15 Because coverage policies have the potential to influence life-extending decisions, it is crucial that they are carefully considered and that care decisions remain in the hands of patients and their physicians—not dictated by payer policies.
“We worry about payers continuing to manage formularies tighter and tighter. That becomes a difficult administrative burden.”
– CEO, community oncology practice
Recommendations
Policy action is needed to protect timely access and physician-led decision-making. Restoring balance between cost containment and patient-centered care requires policy and regulatory action that reduces inappropriate utilization management while ensuring timely, clinically informed review. Priority reforms are as follows:
- Prohibit fail-first step therapy in oncology
- Require that prior authorization and appeals be reviewed by oncologists, including peer-to-peer requirements with appropriate specialty alignment
- Establish strict timelines for prior authorization decisions that reflect the time-sensitive nature of oncology care
- Mandate electronic, standardized platforms for utilization-management processes to reduce administrative burden and reliance on antiquated manual workflows
Conclusion: A Call for Patient-First Oncology Coverage Reform
Cancer care has entered an era of rapid scientific progress, and patients benefit when treatment decisions can be made and implemented quickly by their care teams using the best treatment options. Yet payer utilization management is increasingly shaping access to medical-benefit oncology therapies and services through rules and processes that can delay care, fragment patient journeys, and shift decisions away from physician-led individualized treatment planning.
The goal of reform is not to eliminate oversight, but to ensure that oversight is clinically appropriate, timely, and aligned with the realities of modern oncology. A recent poll by Pew Research Center found that both Congress and the general public believe insurance companies exert too much influence over health policy.16 As a topic of partisan agreement and growing impact on Americans’ lives, Congress must act.
Policymakers and regulators should prioritize a targeted set of changes: ending oncology fail-first requirements, ensuring oncologist-led review of prior authorization and appeals, enforcing clear timelines, and modernizing utilization-management infrastructure through electronic and standardized processes. These steps would reduce avoidable delays, protect patient access, and reaffirm a basic principle: cancer treatment decisions should be driven by patients and their oncology care teams, not by administrative barriers that are misaligned with individualized care. Looking forward, it is our collective responsibility to advocate for people with cancer. Ensuring that physicians retain the ability to make independent, patient-centered treatment decisions is critical to patient care.
Key Takeaways
- Payer utilization management (eg, prior authorization, step therapy) is increasingly applied to medical-benefit oncology, contributing to treatment delays, administrative burden, and misalignment with evidence-based, physician-directed care.
- Survey data show frequent prior authorization denials, limited oncologist involvement in reviews, and treatment delays of 1-4 weeks, potentially compromising outcomes in time-sensitive cancer care.
- Policy reforms are needed to reduce barriers, including eliminating fail-first policies, ensuring oncologist-led reviews, and streamlining authorization processes to protect timely patient access.
Clinical Pathway Category: Business
Author Information
Authors: Lucio Gordan, MD1; Kiana Mehring, MBA, PPMC1; David T. Wenk, MD1; Josh Eaves2; Ryan Ciarrocchi2
Affiliations: 1Florida Cancer Specialists & Research Institute; 2McKesson
Address correspondence to:
Kiana Mehring, MBA, PPMC
Vice President of Payer Strategy & RCM
Florida Cancer Specialists & Research Institute LLC
Managed Care
2890 Center Pointe Drive
Fort Myers, FL 33916
239-218-0119
Kiana.Mehring@flcancer.com
Disclosures: This report was developed through a collaboration between Avalere Health, a health care consulting firm, and Florida Cancer Specialists & Research Institute, a physician-owned and led community oncology practice. Avalere Health conducted the survey and interviews referenced in this report. All authors are either employees or affiliates of these organizations and contributed to the development of this paper in their professional capacities. No author has received personal financial compensation from pharmaceutical manufacturers or payers related to the content of this report. The views expressed herein reflect the authors’ professional perspectives and are intended to inform policy and practice in oncology care. The authors affirm that the findings and recommendations are based on data collected through independent research and are not influenced by external commercial interests.
References
- Runyan A, Yi J, Honcz J. The evolution of payer management of oncology drugs in the United States between 2017 and 2022. J Manag Care Spec Pharm. 2023;29(10):1138-1149. doi:10.18553/jmcp.2023.23045
- Insights on cancer: rates, costs, and strategies. NIHCM Foundation. December 19, 2024. Accessed February 26, 2026. https://nihcm.org/publications/insights-on-cancer-rates-costs-and-strategies
- Loria K. Up, up and not going away: cancer drug prices. Managed Healthcare Executive. October 14, 2022. Accessed February 26, 2026. https://www.managedhealthcareexecutive.com/view/up-up-and-not-going-away-cancer-drug-prices
- Anderson KE, Alexander GC, Ma C, Dy SM, Sen AP. Medicare Advantage coverage restrictions for the costliest physician-administered drugs. Am J Manag Care. 2022;28(70):e255-e262. doi:10.37765/ajmc.2022.89184
- Bradley CJ, Liang R, Lindrooth RC, Sabik LM, Perraillon MC. High-cost cancer drug use in Medicare Advantage and traditional Medicare. JAMA Health Forum. 2025;6(1):e244868. doi:10.1001/jamahealthforum.2024.4868
- Freed M, Bikiek JF, Damico A, Neuman T. Medicare Advantage in 2024: enrollment update and key trends. Kaiser Family Foundation. August 8, 2024. Accessed February 26, 2026. https://www.kff.org/medicare/medicare-advantage-in-2024-enrollment-update-and-key-trends/
- Ungvari Z, Fekete M, Buda A, et al. Quantifying the impact of treatment delays on breast cancer survival outcomes: a comprehensive meta-analysis. Geroscience. Published online June 10, 2025. doi:10.1007/s11357-025-01719-1
- Hanna TP, King WD, Thibodeau S, et al. Mortality due to cancer treatment delay: systematic review and meta-analysis. BMJ. 2020:371:m4087. doi:10.1136/bmj.m4087
- Zouzoulas D, Karalis T, Sofianou I, et al. The impact of treatment delay on endometrial and ovarian cancer patients: a systematic review. Cancers (Basel). 2025;17(13):2076. doi:10.3390/cancers17132076
- Tallen A, Clancy E. Prior authorization in oncology: burdens and barriers to care. Cancer Therapy Advisor. August 20, 2024. Accessed February 26, 2026. https://www.cancertherapyadvisor.com/features/oncology-prior-authorization-burdens-barriers-to-care/
- American Medical Association. 2024 AMA prior authorization physician survey. American Medical Association; 2025. Accessed February 26, 2026. https://www.ama-assn.org/system/files/prior-authorization-survey.pdf
- Yang J, Zhang Q, Raynor L. Controlling cancer care: the emergence of formulary exclusions in oncology. IQVIA. September 21, 2021. Accessed February 26, 2026. https://www.iqvia.com/locations/united-states/library/white-papers/controlling-cancer-care-the-emergence-of-formulary-exclusions-in-oncology
- Getachew B, Stengel K, Donthi S. The new stakeholder economics of Part D after the IRA. Avalere Health. August 29, 2025. Accessed March 3, 2026. https://advisory.avalerehealth.com/insights/the-new-stakeholder-economics-of-part-d-after-the-ira
- Levine AA, Panzer AD, Kauf TL, O’Sullivan AK, Strand L, Chambers JD. Specialty drug coverage varies between health plans’ medical and pharmacy benefit policies. J Manag Care Spec Pharm. 2023;29(6):607-613. doi:10.18553/jmcp.2023.29.6.607
- Murphy T. Limits to anti-nausea pill coverage wear on cancer patients and doctors. Associated Press. September 10, 2024. Accessed February 26, 2026. https://apnews.com/article/cancer-nausea-zofran-ondansetron-coverage-limits-c73a6d1d8ad20108319473d083ee81d2
- Pasquini G, Yam E. Americans’ views on who influences health policy and which health issues to prioritize. Pew Research Center. July 10, 2025. Accessed February 26, 2026. https://www.pewresearch.org/science/2025/07/10/americans-views-on-who-influences-health-policy-and-which-health-issues-to-prioritize/



