


Can a Complete Achilles Rupture Heal Without Surgery? A 4-Year Follow-Up in a High-Risk Patient
This case challenges conventional thinking, demonstrating successful nonoperative management despite a large tendon gap, neuropathy, and poor adherence to treatment recommendations. Four-year follow-up findings highlight the potential for functional recovery and tendon remodeling without surgical intervention.
Key Takeaways
- Nonoperative care can succeed—even in high-risk, complex ruptures.
Despite a full-thickness Achilles rupture with a 3.4 cm gap and significant comorbidities, the patient achieved tendon healing and functional ambulation without surgery, supporting growing evidence that conservative care can be effective. - Surgical advantages may not outweigh risks in diabetic populations.
While surgery may slightly reduce rerupture risk, it carries substantially higher complication rates—particularly in patients with diabetes, neuropathy, and poor glycemic control—making nonoperative management a compelling option. - Functional recovery does not require perfect compliance or anatomy.
Even with suboptimal adherence to offloading and immobilization, the patient demonstrated tendon reattachment via scar remodeling and maintained a satisfactory quality of life, underscoring the importance of individualized, patient-centered treatment decisions.
The Achilles tendon is considered the largest and strongest tendon in the human body and is responsible for ankle plantarflexion and knee stabilization during gait.1,2 The Achilles tendon is composed of fibers contributed by the gastrocnemius and soleus muscles that consolidate and insert into the calcaneal tuberosity. Despite its strength, it is the most frequently ruptured tendon in the lower extremity and such injuries can result in significant functional limitation and prolonged recovery time. Some believe a general increase in the incidence of acute Achilles ruptures may correlate with increased activity in the older population.3 The most common factors contributing to Achilles tendon ruptures are blunt trauma, male sex, pre-existing pathology of the tendon, and abrupt plantarflexion of the foot.4
The main objective of treatment for these ruptures is to restore normal function and achieve patient satisfaction, with least complications possible. Management strategies may be operative or nonoperative, and there is a continuous debate with no clear consensus on a superior option.5,6 The argument for surgery points to data that shows reduced risk of rerupture compared with nonoperative treatment, with risk difference in rupture rates varying from 5-7%.7-9 On the other hand, complication rates of deep vein thrombosis, infection, and sural nerve injury associated with these surgeries vary from 16-21%,7,8 fueling the debate for advocates of nonoperative management.10
A recent analysis of 17,996 patients with Achilles ruptures between 2007 and 2015 found that operative management did not reduce the risk of subsequent ruptures compared to nonoperative management, but did lead to increased risk of wound complications.11 Another recent study by Kosiol and colleagues used magnetic resonance imaging (MRI) and ultrasound to assess tendon quality in operatively and nonoperatively treated acute Achilles tendon ruptures, finding equivalent treatment outcomes, including elongation and thickening of the injured tendon.12 Even though evidence from Canada and Europe has demonstrated the efficacy of nonoperative route since 2010,13,14 and studies do address the role of early weight-bearing in nonoperative cases,15 we have observed a continued bias toward surgical management in the United States.
This report presents a unique case of a patient with diabetes and neuropathy, with multiple comorbidities who presented with a complete rupture of the Achilles tendon managed nonoperatively with a 4-year post-injury follow up. This case is unique in that despite a complete rupture with a large gap of 3.4 cm and continued nonadherence with weight-bearing recommendations, the patient healed with a satisfactory functional outcome observed at 4 years. We believe this case can serve as a reference point for future studies in conservative management of high-risk patients with complex, fully ruptured Achilles tendon injuries.
Case Details
A 67-year-old male presented with a chief concern of right heel pain for 6 months. However, approximately 4 weeks prior to his visit he felt like he was hit in the back of the leg. He continued walking since then due to minimal pain (which he rated as 1 out of 10), however he felt that his gait and balance had subsequently changed. The patient denied any acute injury to the foot and ankle. He had not initiated any treatment on his own prior to his visit. His past medical history was significant for poorly controlled type 2 diabetes with neuropathy (HbA1c of 9.5%), diabetic nephropathy, and morbid obesity. His surgical history was unremarkable. The patient’s medications included metformin 500 mg SR, glimepiride 4 mg, losartan 100 mg, amlodipine 10 mg, and atorvastatin 40 mg, all daily. He had no known allergies.
The patient ambulated into clinic in extra-depth shoes with multidensity plastizote custom molded inserts and a mildly antalgic gait. He had +1/4 dorsalis pedis and posterior tibial pulses with 1-second capillary refill time and moderate nonpitting edema to the right ankle. Neurologic examination showed diminished sharp/dull/vibratory sensation. Semmes-Weinstein 5.07 monofilament sensation was significantly diminished at 1/10 sites tested bilaterally. The patient demonstrated +5/5 muscle strength of the anterior and lateral compartments with a plantarflexion decrease to 3/5 to the right with 5/5 strength in all compartments in the left lower extremity. There was a notable defect of the Achilles along the watershed area with thickening of the tendon more proximally and a positive Thompsons test. The patient exhibited mild pain rated at 3/10 along the site, both with palpation and passive ankle dorsiflexion/plantarflexion. The dermatologic exam showed an increase in texture and turgor to the right ankle with no other significant findings.
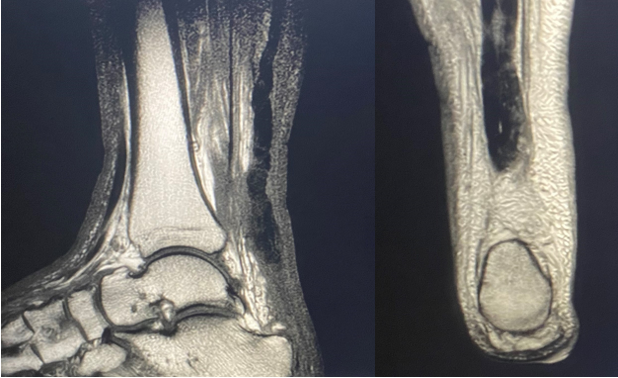
Radiographically, there was no evidence fracture or dislocation in the foot or ankle. Posterior and plantar enthesophytes were noted with soft tissue edema along posterior heel (Figure 1). Subsequent MRI revealed complete rupture of the Achilles tendon, with irregularity and thickening of the distal portion. The normal insertion on the posterior calcaneus was disrupted and approximately 3.4 cm of proximal retraction (Figure 2).

Despite complete rupture of the tendon the decision was made to nonoperatively manage the injury. The team based this decision on the patient’s body habitus and history of difficulty adhering to treatment recommendations, obesity, uncontrolled hemoglobin A1c, neuropathy, nephropathy, and patient’s refusal to consider surgical intervention given potential complications. We thoroughly discussed the possibility of extensive future reconstructive surgery if healing was inadequate. This discussion also included assessment of the patient’s expectations for activity level in the future. Given his refusal to adopt non-weight-bearing status with a plantarflexed cast, we implemented management with a cast boot with attempted minimal weight-bearing for 4 months. Despite strict non-weight-bearing instructions, the patient ambulated without the boot for majority of that 4 months. Subsequently, the patient advanced to an ankle-foot orthosis to allow for proper gait. He also did not adhere to this recommendation, thus we transitioned him to extra-depth shoes with custom accommodative inserts.
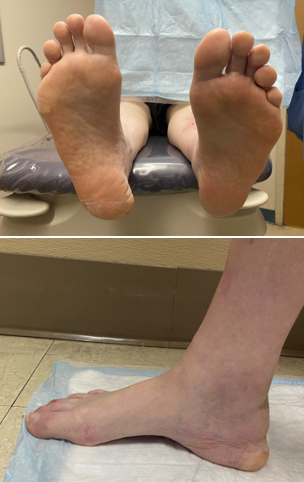
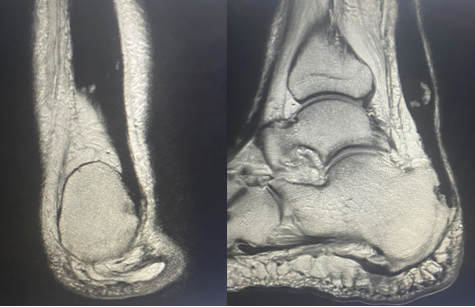
Four years post-injury, the patient continues to ambulate in extra-depth shoes with a notable medial heel fat pad displacement, but with no evidence of wound development, and no pain (Figure 3). He has a decrease in calf girth of 2.9 cm on the right compared to the left and increased ankle dorsiflexion on the right side. Upon stance, his calcaneal resting position is in a mild varus position (Figure 4). His gait reveals lowered push-off force with decreased plantarflexion and increased ankle dorsiflexion on the right side. In addition, his gait exhibits lower gait velocity, shorter stride length, increased dorsiflexion, and longer stance time on the right compared to the left. He also exhibits foot slap upon heel contact. Interestingly, a 4 year follow up MRI showed scarring in the area of the previous defect with evidence of chronic scar remodeling along the Achilles tendon (Figure 5).

Points of Discussion
The Achilles tendon is the largest and strongest tendon in the human body. Despite this, it is the most frequently ruptured tendon in the lower extremity and as a result leads to significant functional limitation and prolonged recovery. Treatment aims to restore function, achieve patient satisfaction, and avoid complications. The debate of surgical versus nonsurgical treatment has not been resolved with evidenced pros and cons existing for both treatment methods. The primary goal for operative intervention rests on the decreased rate of rerupture and early rehabilitation. However, recent literature with large studies have shown similar rerupture rates in operative versus nonoperative management, and notable complications in the operative group.7,8,12 Rupture of the Achilles tendon in the diabetic population can lead to significant complications given common comorbidities. The authors have presented a unique case of a high-risk patient with a total Achilles tendon rupture and a significant 3.4 cm gap, treated nonoperatively with a long-term follow up. Despite this patient’s suboptimal adherence to conservative treatment with improper offloading and immobilization, the patient has healed with minimal functional limitations and with overall high self-satisfaction rating. A 4-year follow up has revealed no complications with wound development and no restriction in his level of activities. Furthermore, a 4-year MRI follow up reveals reapproximation of the ruptured Achilles tendon site with scar tissue.
Conclusion
The operative versus nonoperative management of acute Achilles tendon ruptures remains controversial. Arguments for both can be made, however, more recent data seems to validate the efficacy of nonoperative treatment versus that of operative treatment to be the same with less complications. Certainly, patient selection is key. The authors have presented a unique case of nonoperative management of a complete Achilles tendon rupture in a high-risk patient with a functional and satisfactory outcome at 4 years follow-up. The results shown here bear testament to recent studies advocating for nonoperative management. This case is distinctive because, despite a complete rupture with a substantial 3.4 cm gap and persistent nonadherence, the patient achieved healing through nonoperative management. The tailored modification of the therapeutic treatment on an individual basis with consideration to expected activity level is the best approach in this subpopulation. There is much more work to be done to resolve the debate as to the need for surgical intervention in acute Achilles tendon rupture in high-risk patients. This unique case represents a reference point from which future studies can build upon.
The authors are all Staff Podiatric Surgeons at Veterans Health Affairs in Puget Sound, Seattle, WA.
The authors share that they have no non-financial or commercial, proprietary, or financial interest in the products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
References
- Drake RL, Vogl AW, Mitchell AWM. Gray’s Anatomy for Students. 3rd ed. Philadelphia, PA: Churchill Livingstone; 2015.
- Doral MN, Alam M, Bozkurt M, et al. Functional anatomy of the Achilles tendon. Knee Surg Sports Traumatol Arthrosc. 2010;18(5):638-643.
- Lantto I, Heikkinen J, Flinkkilä T, Ohtonen P, Leppilahti J. Epidemiology of Achilles tendon ruptures: increasing incidence over a 33-year period. Scand J Med Sci Sports. 2015;25(1):e133-e138.
- Hartman H, Cacace A, Leatherman H, et al. Gender differences in Achilles tendon ruptures—a retrospective study and a review of the literature. J Foot Ankle Surg. 2024;63(5):614-620.
- Egger AC, Berkowitz MJ. Achilles tendon injuries. Curr Rev Musculoskelet Med. 2017;10:72-80.
- Ganestam A, Kallemose T, Troelsen A, Barfod KW. Increasing incidence of acute Achilles tendon rupture and a noticeable decline in surgical treatment from 1994 to 2013: a nationwide registry study of 33,160 patients. Knee Surg Sports Traumatol Arthrosc. 2016;24:3730-3737.
- Khan RJK, Carey Smith RL. Surgical interventions for treating acute Achilles tendon ruptures. Cochrane Database Syst Rev. 2010;(9):CD003674.
- Jiang N, Wang B, Chen A, Dong F, Yu B. Operative versus nonoperative treatment for acute Achilles tendon rupture: a meta-analysis based on current evidence. Int Orthop. 2012;36:765-773.
- Wilkins R, Bisson LJ. Operative versus nonoperative management of acute Achilles tendon ruptures: a quantitative systematic review of randomized controlled trials. Am J Sports Med. 2012;40:2154-2160.
- Bergkvist D, Åström I, Josefsson PO, Dahlberg LE. Acute Achilles tendon rupture: a questionnaire follow-up of 487 patients. J Bone Joint Surg Am. 2012;94:1229-1233.
- Crook BS, et al. Operative versus nonoperative treatment of acute Achilles tendon rupture: a propensity score-matched analysis of a large national database. Orthop J Sports Med. 2023;11(2).
- Kosiol J, et al. Operative versus conservative treatment of acute Achilles tendon ruptures: preliminary results of clinical outcome, kinematic MRI and contrast-enhanced ultrasound. Arch Orthop Trauma Surg. 2023;143:2455-2465.
- Wallace RG, Heyes GJ, Michael AL. The nonoperative functional management of patients with a rupture of the tendo Achilles leads to low rates of re-rupture. J Bone Joint Surg Br. 2011;93(10):1362-1366.
- Willits K, Amendola A, Bryant D, et al. Operative versus nonoperative treatment of acute Achilles tendon ruptures: a multicenter randomized trial using accelerated functional rehabilitation. J Bone Joint Surg Am. 2010;92(17):2767-2775.
- Barfod KW. Achilles tendon rupture: assessment of nonoperative treatment. Dan Med J. 2014;61(4):B4837.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






