


Understanding the Peroneal Tendons in Persistent Lateral Ankle Pain
This review outlines a practical, evidence-informed approach to diagnosis, imaging interpretation, and management to help clinicians identify and treat peroneal tendon pathology effectively. Such disorders are often overlooked due to symptom overlap with ligamentous injury and limitations of static imaging.
Key Takeaways
- Persistent “ankle sprain” pain is often not ligamentous—peroneal tendon pathology should be strongly considered when patients present with posterolateral pain, retromalleolar tenderness, or mechanical symptoms.
- Clinical exam remains critical despite advanced imaging—MRI can miss dynamic instability and subtle longitudinal tears, making adjunctive ultrasound and targeted physical examination essential.
- Management hinges on biomechanics and pathology severity—most cases respond to structured conservative care, but surgical intervention yields strong outcomes when tailored to tendon integrity, instability, and contributing anatomy.
Persistent lateral ankle pain following an ankle sprain is a common and often frustrating clinical scenario. Despite apparent ligamentous integrity and resolution of swelling, patients may continue to report pain localized along the lateral ankle. While most ankle sprains resolve uneventfully, persistent symptoms warrant further evaluation for peroneal tendon pathology.
Contemporary consensus guidance emphasizes that delayed recognition increases the likelihood of chronic tendinopathy, mechanical symptoms, and functional limitation, particularly in athletic populations and in the presence of predisposing anatomy.1
The peroneus longus and brevis function as primary evertors and as dynamic stabilizers against inversion. Clinically, their contribution to lateral ankle stability becomes most apparent when patients report activity-related posterolateral pain, retromalleolar tenderness, weakness with eversion endurance, or mechanical snapping. Because the symptom profile overlaps with residual lateral ligament pain, evaluation for possible peroneal pathology must be deliberate.1,2
Key Components of the Physical Examination
Inspection. Inspect the retromalleolar region for subtle fullness. Also document standing alignment; cavovarus alignment and other lateral column-loading phenotypes often have association with with peroneal tendon disorders and can influence outcomes if unaddressed.1,3
Palpation. Focal tenderness is typically posterior to the fibula with peroneal pathology and may extend distally toward the peroneal tubercle. Palpate in neutral and again in slight plantarflexion; the tendons become more superficial and the examination often becomes more discriminating.1
Range of Motion and Strength. Pain with resisted eversion supports the presence of tendinopathy or partial tearing. Weakness is suggestive but not always present, as chronic longitudinal splitting can exist with preserved manual strength. A combined plantarflexion-inversion maneuver frequently reproduces symptoms by tensioning the tendons within the superior peroneal tunnel.1,2
Dynamic Assessment. Resisted dorsiflexion-eversion while palpating the tendons can demonstrate crepitus or excursion. A palpable/visible snap over the fibula during circumduction is strongly suggestive of superior peroneal retinacular insufficiency and dynamic instability, which may static imaging results may underestimate.4
The single-leg heel rise test is a useful adjunct for assessing peroneal endurance and functional strength. Inability to complete repetitions or asymmetric fatigue may indicate underlying tendinopathy or tearing not captured by manual muscle testing alone.
Given the overlap between peroneal tendon pathology and lateral ankle ligament instability, routine performance of the anterior drawer and talar tilt tests can help assess concurrent ligamentous laxity, which may influence surgical procedure selection.
Clinical Pearls
- Always compare bilaterally, using the contralateral limb as a control. However, do not treat the contralateral limb as “normal by default”; bilateral tendinopathy is not rare in cavovarus phenotypes or high-demand athletes.1
- Palpation in slight plantarflexion enhances tendon accessibility.1
- Subtle cavovarus alignment may predispose to recurrent lateral ankle pathology. Adjunct procedures may be necessary if surgery is indicated.1,3
- Perform single-leg heel rise testing to assess functional peroneal endurance; asymmetry or early fatigue may suggest tendinopathy despite preserved manual strength.
- Assess for concurrent lateral ankle instability with anterior drawer and talar tilt testing, as coexisting instability is common and affects management.
Differential Diagnosis
Chronic lateral ankle pain differentials remain broad and include:
- Lateral ligament pathology
- Sinus tarsi syndrome
- Stress injury
- Lateral talar osteochondral pathology
- Calcaneus anterior process injury
- Os peroneum disorders
- Cuboid syndrome
- Superficial peroneal nerve pathology (which may cause motor dysfunction)
Components of Conservative Management
Conservative management is the appropriate first-line approach for most patients with peroneal tendon pathology in the absence of acute full-thickness rupture or refractory instability. Goals include pain reduction, restoration of strength and proprioception, and optimization of biomechanical loading.5
Activity Modification and Immobilization. Initial management typically involves activity modification and a period of relative rest. Use of a controlled ankle motion (CAM) boot or rigid ankle brace for 2–6 weeks in acute or significantly symptomatic presentations may reduce mechanical load on the tendons and allow inflammation to subside.5
Physical Therapy. Structured physical therapy is the cornerstone of conservative care and should include:5
- Progressive eccentric and concentric peroneal strengthening
- Proprioceptive and neuromuscular re-education
- Gait retraining and sport-specific movement pattern correction
- Stretching of the gastrocnemius-soleus complex to reduce tendon load in plantarflexion
- Addressing any identified biomechanical contributors (eg, foot orthoses for cavovarus alignment)
Blood Flow Restriction. Blood flow restriction training has shown early promise as a low-load strengthening strategy in musculoskeletal rehabilitation, and while peroneal tendon-specific evidence remains limited, it represents a potentially useful adjunct during the early recovery period when high-load exercise is not yet appropriate.5
Orthotic Management. Custom or prefabricated foot orthoses with lateral posting may be beneficial in patients with cavovarus alignment or other foot morphologies that increase peroneal tendon stress. In patients with concurrent lateral ligament insufficiency, using functional ankle brace may facilitate return to activity.5
Injections. Corticosteroid injections into the peroneal tendon sheath may provide short-term symptomatic relief, but should be used with caution given the theoretical risk of tendon weakening with repeated administration. Ultrasound guidance improves accuracy. Platelet-rich plasma (PRP) injection represents an emerging option, though current evidence remains limited for peroneal tendon pathology specifically.5
Duration and Transition to Surgery. A trial of structured conservative management lasting 3–6 months is generally appropriate before considering surgical intervention. Persistent pain, functional limitation, or progression of pathology on imaging despite conservative therapy may indicated need to proceed with further evaluation and surgical planning.5
MRI Evaluation
Consideration of magnetic resonance imaging (MRI) is appropriate in patients with chronic lateral ankle pain unresponsive to conservative therapy, or when examination findings suggest tendon tear, weakness, subluxation, or associated pathology.1,2
Key Findings
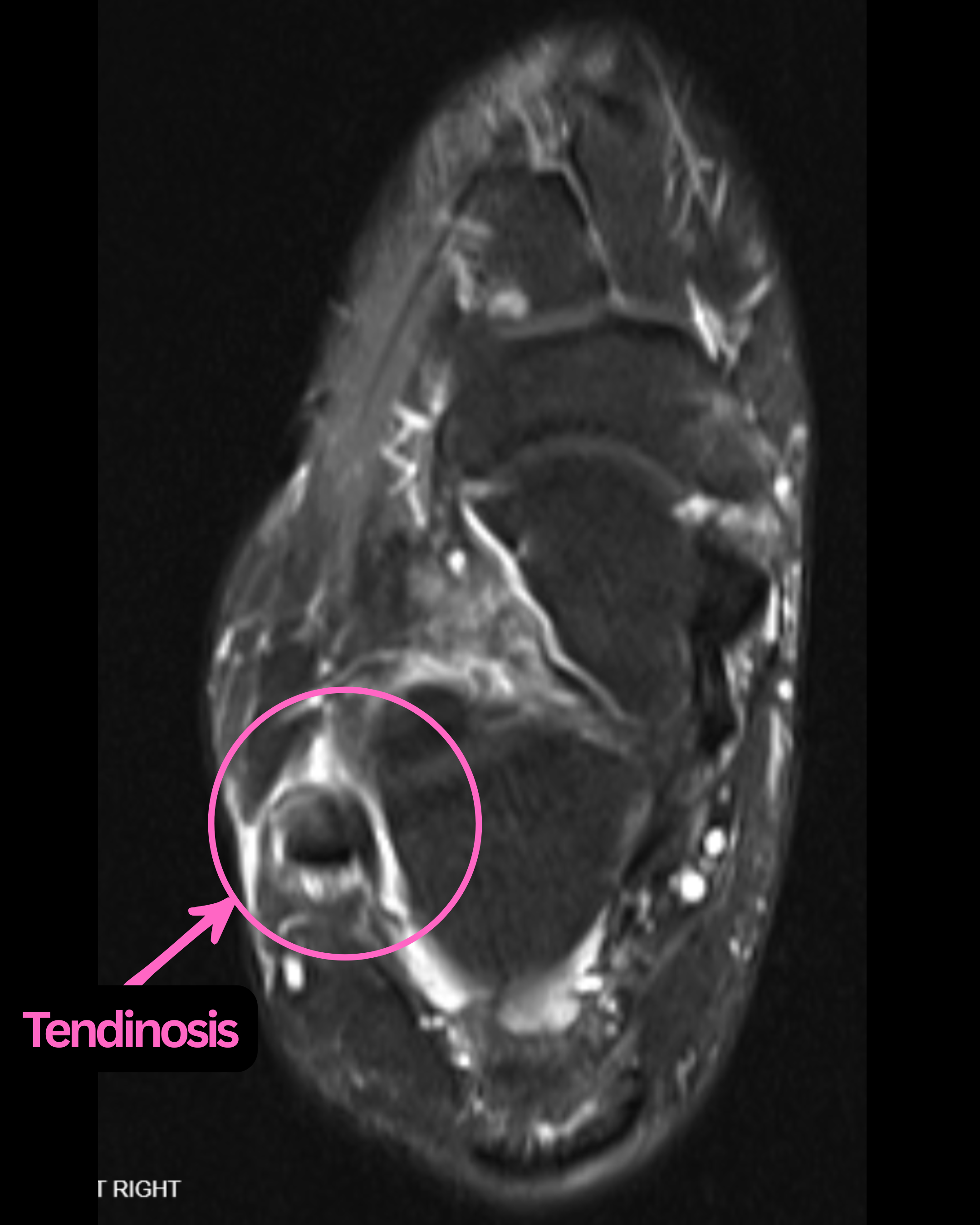
Tendinosis. Increased intratendinous signal intensity with thickening and peritendinous fluid; may represent acute or chronic change.2
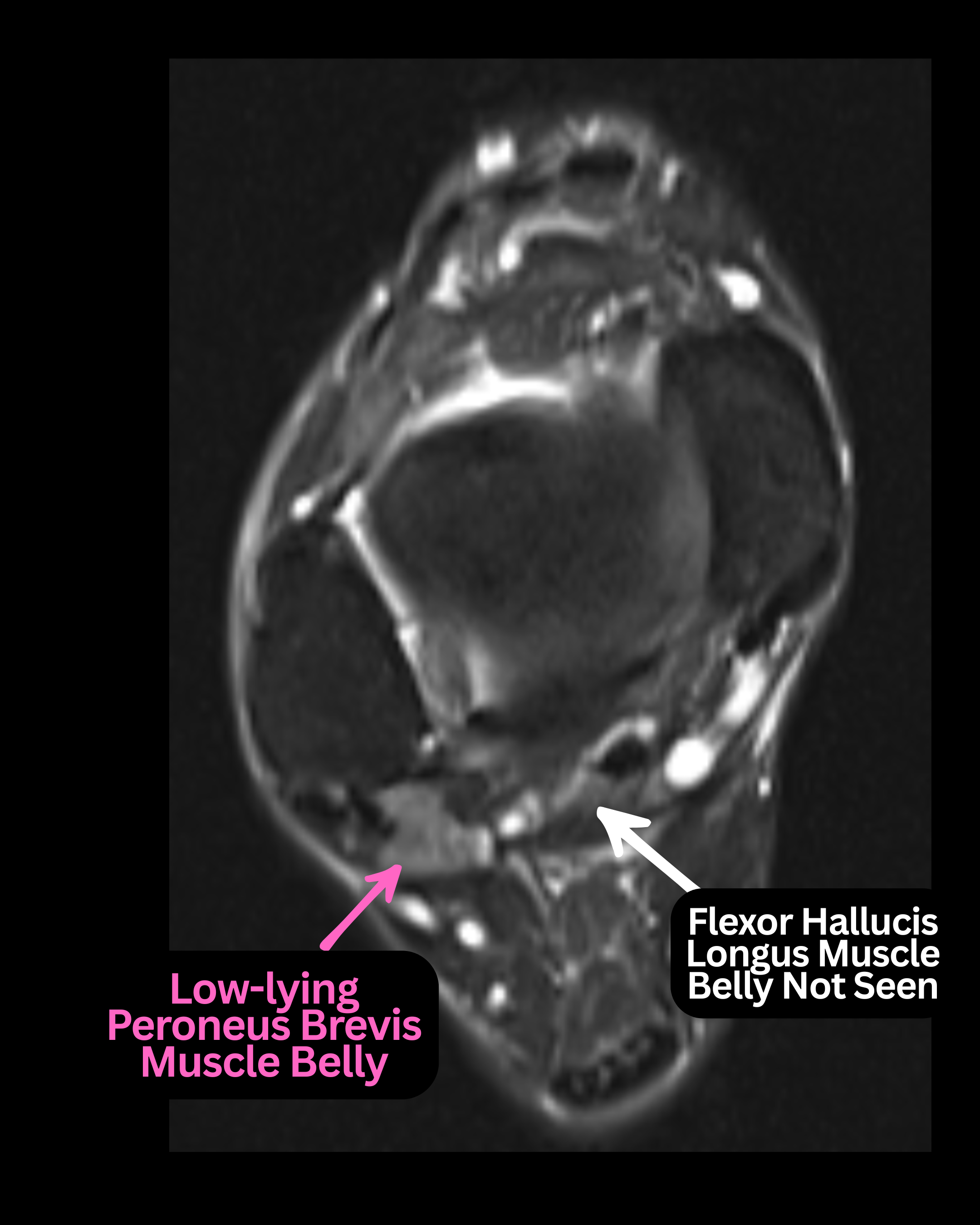
Low-lying Muscle Belly. This finding is characterized by distal extension of muscle tissue into the retromalleolar groove. When the peroneus brevis muscle belly extends more distally than expected, it represents a low-lying variant that can contribute to tendon crowding and tearing.1,6 Evaluating an axial MRI view contributes to diagnosis of low-lying muscle belly, identifying the most inferior level of flexor hallucis longus (FHL) muscle belly. If one notes any peroneus brevis muscle belly inferior to this level, it constitutes a pathologic finding.
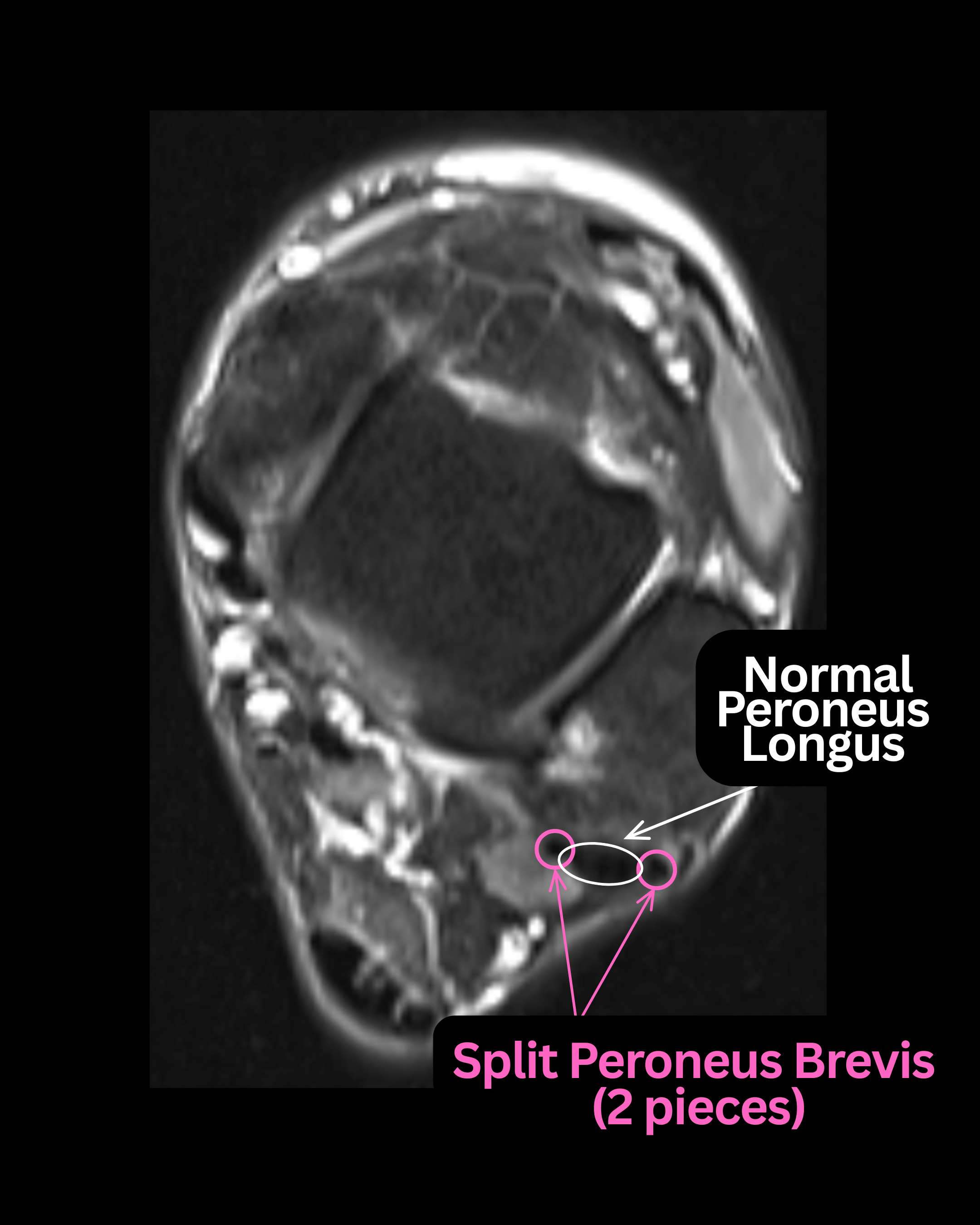
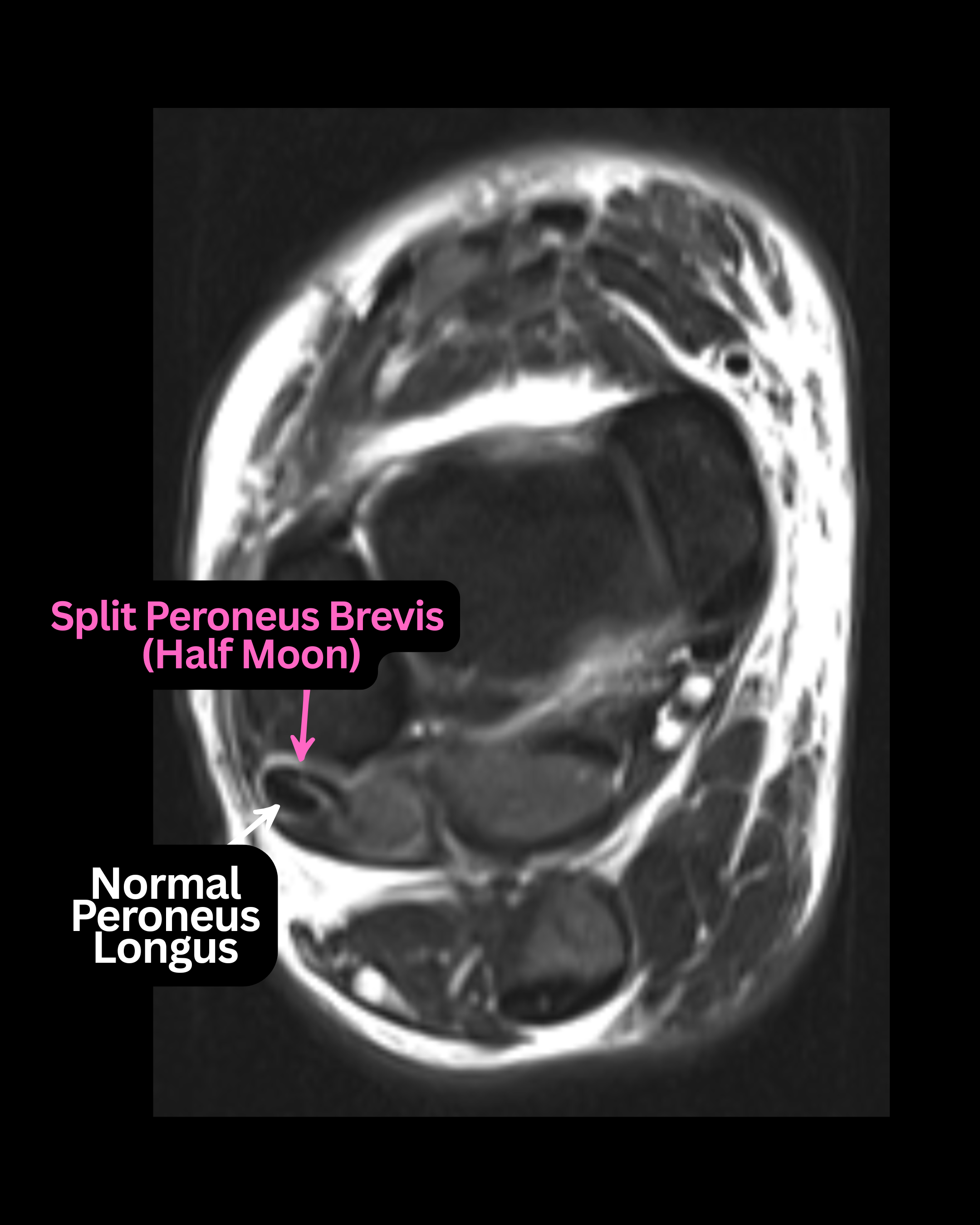
Longitudinal Split Tears. Most commonly involves the peroneus brevis, seen as 2 round structures or a crescentic configuration on axial images. Recent pictorial review literature emphasizes that these can be subtle and vulnerable to interpretive pitfalls.6
Subluxation/Dislocation. Tendons displaced lateral or anterior to the fibula, often with retinaculum injury and sheath fluid. Note: this is typically a dynamic problem diagnosed clinically or on ultrasound; static tests like MRI may not show pathology.4
Os Peroneum Pathology. Fracture, displacement, or entrapment of the os peroneum may mimic or exacerbate peroneal symptoms. Contemporary radiology review literature frames this as a spectrum (painful os peroneum syndrome) often linked with peroneal tendon pathology.7
Limitations. MRI may yield false negatives due to the small, obliquely oriented tendons and partial volume averaging. The “magic angle” artifact—which occurs when tendons oriented at approximately 55° to the magnetic field exhibit artificial T2 signal—can further obscure findings. Static imaging also fails to assess dynamic instability such as subluxation. Recent peroneus brevis split-tear imaging reviews specifically discuss the oblique course/magic-angle artifact as a recurrent pitfall in routine clinical MRI interpretation.6
Adjunct Imaging. Dynamic ultrasound provides a valuable complement, allowing real-time evaluation of tendon motion and instability during active or resisted maneuvers. In a 2024 study comparing imaging with intraoperative findings, ultrasound demonstrated higher sensitivity for peroneal subluxation than MRI, while MRI was slightly more accurate for tears in that cohort.4
Bottom Line
MRI remains a valuable tool for delineating peroneal tendon pathology, but clinical correlation is essential. Longitudinal tears and crowding variants (including low-lying muscle belly/accessory muscles) are emphasized in recent imaging reviews as commonly underappreciated without careful, tendon-specific image review.6
Notes on Surgical Management
A curvilinear incision posterior to the fibula provides optimal access while minimizing sural nerve injury. Identification and incision of the superior peroneal retinaculum takes place, preserving a cuff for later repair; consensus guidance and contemporary technique reviews emphasize that retinacular handling is central to durable stabilization and to avoiding postoperative stenosis.1,2
Intra-operative assessment should include:
- Tendinosis (thickening, fraying, discoloration)
- Partial or longitudinal tears (commonly peroneus brevis)
- Full-thickness tears (rare)
- Instability or excessive tendon excursion
- Accessory pathology (os peroneum, low-lying muscle belly, peroneus quartus)
Surgical Options
Debridement and Tubularization. Resection of devitalized tissue followed by tubularization aims to restore structure and function. Contemporary operative reviews support repair/ tubularization strategies when tendon quality is adequate and contributing instability/crowding is addressed.2
Side-to-Side Tenodesis. Salvage procedure for advanced tearing/poor tendon quality. Contemporary reviews emphasize viability and functional tendon substance as the practical determinant (rather than a single rigid percentage threshold).2
Peroneus Longus Pathology. Pathology isolated to the peroneus longus, including longitudinal tearing, tendinosis, and os peroneum-associated injury, is more rare. In cases of severe longus destruction where tenodesis is not feasible, allograft or autograft tendon reconstruction represents an advanced salvage option, though evidence specific to peroneal tendon reconstruction remains limited.
Surgeon familiarity and patient-specific factors should guide selection.7
Os Peroneum Management. Symptomatic fractures or entrapment require excision with tendon repair or fixation when appropriate; modern radiology reviews describe this as a spectrum involving both the ossicle and peroneus longus tendon.7
Retinacular Repair and Groove Deepening. Essential in cases of recurrent subluxation. Recent systematic review literature continues to report high satisfaction and low redislocation rates, with higher return-to-sport rates in pooled data when groove deepening is combined with superior peroneal retinaculum (SPR) repair in appropriate patients.8
Separate contemporary series also support anatomic SPR reattachment without groove deepening in selected patients, reflecting ongoing technique variability and the importance of tailoring to anatomy and chronicity.9
Peroneus Quartus and Accessory Muscles
The peroneus quartus is an accessory muscle present in up to 20–25% of individuals and most commonly found within the peroneal tunnel posterior to the fibula. When present, it contributes to tendon crowding and is associated with increased rates of peroneus brevis pathology. At the time of surgery, accessory muscles and tendons should be identified and addressed. Excision of the peroneus quartus is generally recommended when crowding is thought to contribute to pathology, as failure to do so may increase recurrence risk.
Technical Pearls
- Preserve healthy tendon tissue whenever feasible
- Leave an adequate retinacular cuff to facilitate secure repair
- Avoid overtightening the retinaculum to prevent postoperative stenosis
- Address accessory pathology (low-lying muscle belly/accessory muscles) to reduce recurrence risk
- When performing tenodesis, tension the tendons with the ankle in neutral dorsiflexion and slight eversion
Considerations for Postoperative Management
Typical postoperative care includes:
- Immobilization in a CAM boot with crutches/knee scooter for 3–4 weeks and up to 6 weeks (depending on preoperative mobility)
- Early non-weight-bearing range of motion exercises with the boot off
- Progressive weight-bearing at 3–4 weeks postop with initiation of physical therapy, emphasizing proprioception, strength, and gradual return to activity
- Return to full activity for most cases is generally feasible at 8–12 weeks depending on reconstruction extent and patient factors1,2
- More extensive reconstructions (groove deepening, tenodesis, retinacular repair) may require 4–6 months to achieve sport-level return. Guidance for return-to-sport readiness typically follows functional criteria including strength symmetry (≥90% limb symmetry index), single-leg heel rise endurance comparable to the contralateral side, and successful completion of sport-specific movement tasks1,2
Conclusion
A thorough understanding of peroneal tendon anatomy, biomechanics, and clinical presentation is essential for accurate diagnosis and effective management of persistent lateral ankle pain. Because symptoms often mimic a protracted ankle sprain, clinicians may overlook peroneal tendon disorders without meticulous physical examination and appropriate imaging. MRI remains a valuable diagnostic tool, though its limitations—particularly in dynamic pathology and subtle longitudinal tearing—necessitate careful clinical correlation and, when appropriate, adjunctive dynamic ultrasound.
When pathology is clearly defined and the operative plan is tailored to the specific tendon disorder, surgical intervention yields favorable outcomes. Modern reviews and systematic analyses support durable improvement across repair, tenodesis, and instability-focused procedures in appropriately selected patients.2
Dr. Dikis currently practices as a partner with McFarland Clinic in Iowa. He is certified in foot surgery and reconstructive foot and ankle surgery by the American Board of Foot and Ankle Surgery. He serves as clinical faculty with the Des Moines University College of Podiatric Medicine and Surgery. He is the host and creator of the Pod Patrol podcast, and one-half of the Instagram tandem FootDocDuo.
Disclosures
Dr. Dikis discloses no non-financial or commercial, proprietary, or financial interest relevant to the manuscript. He discloses that AI tools were used in the manuscript only for structure formatting.
References
1. van Dijk PA, Miller D, Calder J, et al. The ESSKA-AFAS international consensus statement on peroneal tendon pathologies. Knee Surg Sports Traumatol Arthrosc. 2018;26(10):3096-3107.
2. Danna NR, Brodsky JW. Diagnosis and operative treatment of peroneal tendon tears. Foot Ankle Orthop. 2020;5(2):2473011420910407.
3. Bagley C, Parker L. Diagnosis and treatment of peroneal tendon disorders. Orthop Trauma. 2023;37(1):71-78.
4. Melville DM, Taljanovic M, et al. Comparison of ultrasound and MRI with intraoperative findings in the diagnosis of peroneal tendinopathy, tears, and subluxation. J Clin Med. 2024.
5. Howard A, John A, Theiss R. Peroneus tendon disorders: Evaluation and non-operative management. Curr Phys Med Rehabil Rep. 2023;11:152-162.
6. Bokwa-Dąbrowska K, Zych R, Mocanu D, Huuskonen M, Dziedzic D, Szaro P. Peroneus brevis split tear - A challenging diagnosis: A pictorial review of magnetic resonance and ultrasound imaging. Part 1. Anatomical basis and clinical insights. Eur J Radiol Open. 2025 Jan 8;14:100633.
7. Hallinan JTPD, Wang W, Pathria MN, Smitaman E, Huang BK. The peroneus longus muscle and tendon: a review of its anatomy and pathology. Skeletal Radiol. 2019 Sep;48(9):1329-1344.
8. Di Santo P, Basciani S, Papalia GF, et al. Return to sport after surgical treatment for dislocation of the peroneal tendon: a systematic review of the current literature. Applied Sciences. 2023; 13(13):7685.
9. Pearce CJ, Calder JDF. Surgical anatomy of the peroneal tendons. Foot Ankle Clin. 2011;16(3):391–403.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






