


Contiguous Stump Neuromas After Morton's Neuroma Surgery: Surgical Management, Outcomes, and Clinical Considerations
This review examines the anatomical basis, clinical presentation, and surgical management strategies for challenging revision cases, with insights into outcomes and postoperative considerations.
Key Takeaways
- Contiguous stump neuromas can develop between adjacent interspaces following Morton's neuroma surgery, creating complex forefoot pain that may be difficult to diagnose and treat.
- Anatomical communication between the second and third interspaces may contribute to neuroma formation and symptom recurrence after primary neurectomy.
- Careful surgical planning and revision neuroma resection can help address persistent symptoms, highlighting the importance of understanding interdigital nerve anatomy and postoperative complications.
Primary interdigital neuroma represents an entrapment neuropathy caused as the nerve passes beneath the deep transverse metatarsal ligament (DTML). Resultant compression leads to perineurial fibrosis, demyelination, and endoneurial edema on histopathology. Notably, inflammatory changes are absent. Approximately 85–90% of primary interdigital neuromas occur in the third intermetatarsal space, involving the medial plantar nerve. 10–15% occur in the second interspace, also involving the medial plantar nerve. In 27% of cases, a communicating branch from the lateral plantar nerve blends with the medial plantar common digital branch, creating a larger nerve trunk in the third interspace and making it more vulnerable to compression.1 In addition, increased mobility between the central metatarsal column (2–3) and the lateral column (4–5) at the Lisfranc joint contributes to greater tethering of the nerve against the DTML within the third interspace. This may explain the higher incidence of neuroma formation at this location.
Patients with interdigital neuroma typically report plantar forefoot pain that worsens with walking and is relieved by rest, shoe removal, walking barefoot, or wearing sandals. Pain frequently radiates into the digits and can persist intermittently for weeks to months. Massaging the affected interspace may reduce symptoms. Physical examination commonly reveals plantar tenderness and fullness in the symptomatic webspace. Splaying or subluxation of adjacent digits may be noted. A positive Mulder’s sign—described as a palpable or audible “click” when the enlarged nerve is displaced dorsally—is often present in the third interspace. One must also rule out monosynovitis and plantar plate tears during evaluation.

The presence of concomitant second and third intermetatarsal space neuromas remains controversial. Thompson and Deland noted a low frequency of only 2–3 percent.2 Friscia reported a 42% dissatisfaction rate following surgical intervention.3 The senior author recommends excising a neuroma from only one interspace at a time, addressing the most symptomatic first; in his experience, the vast majority of patients do not require further surgery, and in the small number remaining, staged intervention after 6 months yields an overall very high satisfaction rate.
One must also consider more proximal nerve pathology. Tarsal tunnel syndrome may mimic contiguous neuromas. Lumbar radiculopathy—L5 (associated with second interspace symptoms) or S1 (third interspace)—must also be excluded. A stump neuroma can develop after primary neuroma excision, typically due to inadequate proximal resection. Persistent or recurrent symptoms may appear as late as years after surgery. When using a dorsal McElvey approach,4 one must release the DTML and distract the metatarsal heads with a smooth laminar spreader. Cutting distal branches is inconsequential, as Wallerian degeneration will occur.
As our experience supports, common causes of failure in neuroma surgery include:
- Inadequate proximal resection of the nerve
- Poor proximal retraction of the cut nerve
- Tethering of the nerve stump to the capsule, DTML, or plantar skin
In this case, we report an instance of an interesting complication post-neuroma excision.

Case Report
A 42-year-old female presented for a third opinion after persistent pain following a prior left third interspace neuroma excision performed a year earlier. Of note, she had no significant past medical or surgery history other than this presenting concern. Persistent symptoms, including pain radiating to the second intermetatarsal space, led to a second surgery addressing the second interspace later that same year. Despite these interventions, she continued to experience severe recalcitrant forefoot pain and was unable to bear weight. Our team considered, but ruled out via physical examination findings, complex regional pain syndrome. Examination revealed intact vascular status, numbness in the third digit, and significant dysesthetic pain along the metatarsal heads and in both the second and third intermetatarsal spaces.
Electromyography/nerve conduction studies (EMG/NCS) demonstrated tarsal tunnel syndrome, supported by positive Tinel’s sign on examination. Magnetic resonance imaging (MRI) with contrast confirmed residual stump neuromas in both the second and third interspaces. The patient consented to surgical intervention consisting of revisional stump neuroma excision of both interspaces and a tarsal tunnel release.
Notes on the Operative Technique
Anesthesia included epidural and general anesthesia, supplemented with a posterior tibial nerve block using 12 mL of 0.5% bupivacaine plain. Positioning was typical supine on the operating table, with a bump under the ankle.
Tarsal Tunnel Release. We made a longitudinal incision one fingerbreadth anterior to the Achilles tendon medially along the course of the laciniate ligament. Dissection proceeded through the subcutaneous tissues to the ligament, which we released along the course of the posterior tibial nerve, along with the superficial fascia of the abductor hallucis, retracting the muscle inferiorly. We then released the fascial tunnels of the medial and lateral plantar nerves within the deep fascia. Skin closure was with 4-0 poliglecaprone reinforced with 4-0 nylon.
Second and Third Intermetatarsal Stump Neuroma Excision. Eighteen-gauge hypodermic needles inserted from dorsal to plantar just proximal to the metatarsal heads identified the precise location of the interspaces and the proximal convergence of the metatarsals (Figure 1). We created a modified Betts incision beginning proximal to the second metatarsal plantarly and curving laterally over the third metatarsal in a longitudinal fashion. We deepened the incision through subcutaneous tissue to the plantar fascia, which we then incised longitudinally over the second interspace needle. The common digital nerve was evident beneath the flexor digitorum brevis.
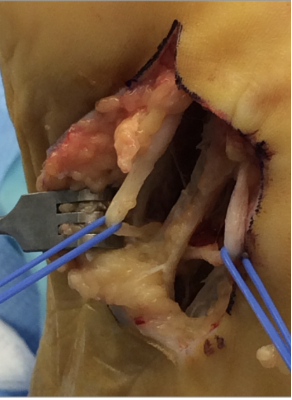
A similar incision and exposure took place for the third interspace (Figure 2). We identified both nerves as adherent to the plantar capsule of the third metatarsal head. We then transected the proximal nerve stumps within the inferior margin of the plantar incision (Figure 3). Closure of the epineurium was with 6-0 nylon, allowing the cut nerves to retract proximally into the midfoot (Figure 4). More superficial closure took place with 4-0 poliglecaprone subcutaneous sutures reinforced with multiple 4-0 nylon simple sutures.

Highlighting the Postoperative Course
We placed the patient in a posterior splint after applying the postsurgical dressing and instructed her to remain non-weight-bearing with a knee walker. She underwent sympathetic blockade by pain management as an outpatient for 2 consecutive days postoperatively.
Sutures remained in for 3 weeks, and the patient then began partial-to-full weight-bearing in a cast boot. At 6 weeks she started physical therapy and transitioned to regular footwear over the following 2 weeks. She experienced a recovery period of approximately 6 months, which we find to be typical with this type of incision and with a revisional surgery. However, at 1-year postoperatively, she reported 80% improvement compared to her preoperative state.

Conclusion
Stump neuroma following primary excision of a common digital nerve occurs in 10–30% of patients and accounts for up to 30% of postoperative pain after neuroma surgery.5 This remains a significant reason why surgical excision is best reserved for cases of full exhaustion of conservative measures.
Incomplete resection, incorrect diagnosis, or regenerating nerve fibers within scar tissue can contribute to recurrent symptoms. Careful surgical technique and appropriate patient selection are essential to achieving optimal outcomes. As this was a revision case, our team felt a plantar incision was necessary, and that a combination of factors led to that point. This example serves as a representative case that underscores the complexity that a stump neuroma presents to foot and ankle surgeons.
Dr. Visser is a past president of the St. Louis Podiatric Medical Society and the Missouri Podiatric Medical Association. He served as an examiner of the American Board of Podiatric Surgery and on the Missouri State Board of Podiatric Medicine over several governorships. He’s been a residency director for 40 years, most currently, at SSM-Depaul Foot and Ankle Reconstructive and Trauma Surgical Program in St. Louis, MO.
Dr. Pedagandham is Chief Resident at SSM Health DePaul Hospital Foot and Ankle Surgery Residency in St. Louis, MO.
The authors declare no known competing financial interests or relationships that could have influenced the work reported in this paper.
References
1. Wheeless, C. R., III. (n.d.). Morton's neuroma: Interdigital perineural fibrosis. Wheeless' Textbook of Orthopaedics. Retrieved June 4, 2026, from https://www.wheelessonline.com/orthopaedics/mortons-neuroma-interdigital-perineural-fibrosis/
2. Thompson FM, Deland JT. Occurrence of two interdigital neuromas in one foot. Foot Ankle. 1993;14(1):15-7. doi: 10.1177/107110079301400103. PMID: 8425725.
3. Friscia DA, Strom DE, Parr JW, Saltzman CL, Johnson KA. Surgical treatment for primary interdigital neuroma. Orthopedics. 1991;14(6):669-72. doi: 10.3928/0147-7447- 19910601-07. PMID: 1866348.
4. Akermark C, Saartok T, Zuber Z. A prospective 2-year follow-up study of plantar incisions in the treatment of primary intermetatarsal neuromas (Morton's neuroma). Foot Ankle Surg. 2008;14(2):67-73. doi: 10.1016/j.fas.2007.10.004. Epub 2008 Feb 21. PMID: 19083618.
5. Thomajan CH. A method for entubulating exposed nerve ends following neurectomy using a porcine extracellular matrix nerve cap. Foot Ankle Spec. 2022 Dec;15(6):579-585. doi: 10.1177/19386400221106642. Epub 2022 Jul 1. PMID: 35778874; PMCID: PMC9643824.
6. Beskin JL, Baxter DE. Recurrent pain following interdigital neurectomy--a plantar approach. Foot Ankle. 1988;9(1):34-9. doi: 10.1177/107110078800900107. PMID: 3220333.
7. Mann RA, Reynolds JC. Interdigital neuroma--a critical clinical analysis. Foot Ankle. 1983;3(4):238-43. doi: 10.1177/107110078300300411. PMID: 6832668.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






