


Can We Fill in the Gaps? Authoring Custom Oncology Pathways vs Surfacing NCCN Preferred Recommendations Alone
Abstract
The use of clinical decision support (CDS) tools may help to optimize the delivery of value-based cancer care and reduce variations in treatment. Flatiron Assist (FA) is an electronic health record (EHR)-embedded CDS tool that is locally customizable and designed to aid medical oncologists in selecting and documenting National Comprehensive Cancer Network (NCCN) Guideline–concordant, NCCN Preferred, and/or customized treatment regimens. The study aimed to compare the availability of NCCN Preferred recommendations to custom preferred pathways in FA, and to assess provider concordance with the preferred suggestions. This retrospective, observational, real-world study analyzed 16,722 orders for breast, non-small cell lung, and colon cancers over 11 months, placed at 12 US-based sites of care by 522 clinicians in hospital and community-based cancer clinics. Of the 13,140 orders placed at sites where NCCN Preferred was available, an NCCN Preferred option existed for 7,680 orders, resulting in 58.5% relative coverage for the clinical scenarios in scope. Of the 3,261 orders placed where a custom preferred pathway was available, a custom preferred option existed for 2,320 orders, resulting in 71.1% relative coverage for the clinical scenarios in scope (rate ratio 1.22, 95% confidence interval 1.19-1.25; P < .001 favoring custom preferred pathways). When a preferred option was available, providers’ selection rates were similar. The study highlights the opportunity for custom preferred pathways to guide oncologists and provide clearer guidance in cases where NCCN Preferred is not available. FA’s design, with the ability to provide a local preference, and the option to highlight treatment regimens based on efficacy, safety, and affordability, makes it a valuable tool for oncologists to navigate the complex treatment landscape. The study emphasizes the need for accessible and accurate information to ensure high-quality cancer care delivery.
Background
Clinical decision support (CDS) tools can facilitate value-based cancer care delivery and enable measurement of guideline and pathway concordance to improve quality and reduce variation in care.1 Flatiron Assist (FA) is an electronic health record (EHR)-embedded and locally customizable CDS tool for medical oncologists that facilitates systemic treatment selection and documentation of National Comprehensive Cancer Network (NCCN) Guideline–concordant, NCCN Preferred, and/ or customized locally preferred treatment regimens.
There are two distinct types of guidance available for providers when making clinical decisions: treatment guidelines and treatment pathways.
Treatment guidelines, such as the NCCN Guidelines, may offer a number of clinically equivalent treatment options for a given clinical scenario. While this provides a user with flexibility and adaptability in their treatment selection, a larger number of options may lead to variation in selection, even among doctors within the same site of care. In addition to opening the door to inequities in care, this can adversely impact both the cost of care (some regimens may be significantly more expensive than others) as well as operational efficiency of the local pharmacy and infusion center.
Meanwhile, treatment pathways are more directive in nature and may identify a single preferred option for a given clinical scenario. While this can reduce variation in care, it may not account for local nuance, including situations in which different payers within a geographical area may have different preferred options for two patients with the same clinical scenario.
Previous studies have reported that NCCN Preferred is designated for 57% of clinical scenarios encountered in the real world.2 While this is important progress toward reducing unwanted variation and improving equitable delivery of high-quality cancer care, it still leaves 43% of clinical scenarios unaccounted for. This suggests an opportunity for custom preferred pathways to provide oncologists with clearer guidance in the gap.
Given the complexity of the health care and specialty drug environment, there will likely never be “one pathway to rule them all.” As a result, providers need accurate and accessible information about how to navigate an increasingly complex landscape of guidelines and pathways for each unique clinical, administrative, and financial situation.
However, cancer treatment is changing rapidly, and few sites of care are resourced to develop and maintain local preferences for every clinical scenario. FA offers NCCN Preferred designation when available, as well as the option for sites of care to designate a local preference. NCCN Categories of Preference is a designation used to highlight treatment regimens that are preferred based upon superior efficacy, safety, and when appropriate, affordability.3
The goal of this retrospective analysis was to compare availability of NCCN Preferred recommendations to custom preferred pathways to assess overall availability and provider concordance with the preferred suggestions encountered in the CDS tool.
Methods
This study is a retrospective, observational, real-world study of the treatment-selection patterns of oncologists in the US using FA, a point-of-care CDS tool. For a given clinical scenario, FA surfaces therapeutic options as NCCN Preferred; custom preferred; both NCCN and custom preferred; NCCN concordant-not preferred; or NCCN nonconcordant. A clinical scenario is defined as a unique set of clinical data elements that describe a patient’s cancer diagnosis and is how NCCN indications are categorized in FA. Clinicians must select the clinical scenario from a predefined list that describes their patient as part of the regimen-ordering process in the tool so that concordance data are known. We used the nationwide, EHR-derived deidentified Flatiron Health database to analyze treatment regimen orders placed during an 11-month observation period (February 1, 2022, through December 31, 2022) across 12 sites of care by 522 clinicians in both community and hospital-based cancer clinics. We assessed patterns of preferred and nonpreferred treatment regimen ordering to determine the percentage of clinical scenarios covered by sites that exclusively displayed NCCN Preferred vs those that displayed custom preferred pathways within the CDS tool. Sites were excluded if they displayed both NCCN and custom preferred to ensure there was no overlap within the analysis.
The study includes all treatment-selection episodes in which FA was used to assist in selection of systemic therapy for breast, non-small cell lung, and colon cancers. Each episode of treatment selection using FA is characterized as a unique event. We analyzed the frequency of orders placed that were covered by the preferred pathway and reported those as proportions (%) with 95% confidence intervals (CIs) and compared groups using chi-square tests. Mantel-Haenszel rate ratios (RRs) and 95% CIs were calculated to estimate the relative likelihood of the clinical scenario being covered by the preferred pathway comparing NCCN Preferred to custom preferred. We also analyzed the frequency with which a preferred option was selected when there was one available for the given clinical scenario.
Results
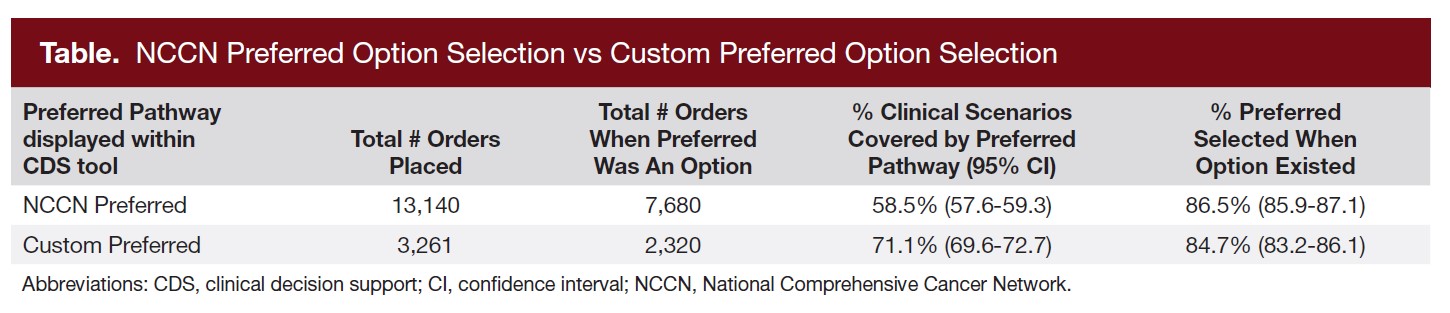
We analyzed a total of 16,401 orders during this study, of which 13,140 were placed at sites that displayed NCCN Preferred options within the CDS tool and 3,261 were placed at sites that displayed their own custom preferred pathway. Of the 13,140 orders placed at sites where NCCN Preferred was available, an NCCN Preferred option existed for 7,680 orders, resulting in 58.5% relative coverage for the clinical scenarios in scope. Of the 3,261 orders placed where a custom preferred pathway was available, a custom preferred option existed for 2,320 orders, resulting in 71.1% relative coverage for the clinical scenarios in scope. The RR was 1.22 in favor of the custom preferred pathways (95% CI, 1.19-1.25; P < .001).
The rates at which a preferred selection was made when available were similar between groups. Providers selected a preferred treatment for 86.5% of scenarios where NCCN Preferred was an option and 84.7% of scenarios where custom preferred was an option (RR, 0.96; 95% CI, 0.90-1.02; P = .060) (Table).
Discussion
This study demonstrates that custom preferred pathways have the ability to cover more clinical scenarios than NCCN Preferred alone. It also demonstrates that regardless of which preferred pathway is displayed, providers order a preferred treatment a large majority of the time when placing an order in a CDS tool that highlights preferred treatment options.
Cancer clinics that invest resources in developing their own custom pathways and use a CDS tool to display those options within the workflow at the point of care may be able to reduce unwanted variation, as illustrated by the high rate of ordering preferred treatments when the option exists. With previous research4 indicating that a physician who has recently ordered a nonrecommended or low-value treatment is more likely to continue ordering that same low-value treatment in the future, it is critical to set users on the right path at the beginning by surfacing actionable, reliable information about recommended treatment decisions.
A limitation of this study is that we do not know concordance or preference availability across the orders placed outside of the CDS tool. It is possible that clinicians choose to use the CDS tool when the treatment choice is likely to be concordant but choose not to use the tool when they are selecting treatments that are likely to be nonconcordant or nonpreferred. Another limitation is that deployment of the tool is self-selected at the clinic and physician level and that the analysis is limited to a particular point in time; thus, results may not be generalizable. Finally, this study only involved three cancer types and did not examine preference availability or concordance rates between early-stage and late-stage disease, where important variation may occur. A previous study reported that NCCN preferred treatment regimens existed in 50% of breast, 54% of non-small cell lung, and 46% of colon cancer clinical scenarios.2
The combination of both NCCN and custom preferences may offer more robust coverage of clinical scenarios encountered by oncologists; that and its impact on concordance are worthy of future study. Future studies will aim to understand why clinicians use CDS tools for treatment selection in order to measure the availability of preferences and concordance for all systemic therapy encounters.
Conclusion
Given the increasing complexity of the oncology treatment landscape, this study found that utilizing a customizable CDS tool like FA provides an opportunity for custom preferred pathways to optimize cancer treatment ordering in cases where NCCN guidelines are less clear and that regardless of the pathway in place, providers order preferred treatment options a large majority of the time.
Author Information
Authors: Rebecca Maniago, PharmD, BCOP; Marcello Ricottone; Gregory S. Calip, PharmD, MPH, PhD; Taylor Dias-Foundas; James Hamrick, MD, MPH
Affiliations: Flatiron Health, Inc, New York, NY
Address correspondence to:
Rebecca Maniago, PharmD, BCOP
Flatiron Health, Inc
233 Spring St
New York, NY 10013
Email: rebecca.maniago@flatiron.com
Funder: This study was sponsored by Flatiron Health, Inc, which is an independent member of the Roche Group.
Disclosures: All authors report employment at Flatiron Health, Inc, which is an independent member of the Roche Group, and stock ownership in Roche.
References
1. Neubauer MA, Hoverman JR, Kolodziej M, et al. Cost effectiveness of evidence-based treatment guidelines for the treatment of non–small-cell lung cancer in the community setting. J Oncol Pract. 2010;6(1):12-18. doi:10.1200/JOP.091058
2. Congelli JM, Maniago R, Jou S, Donegan J, Altomare I. BPI22-015: analysis of NCCN-preferred treatment regimen ordering via an EHR-embedded decision support tool in a community oncology practice. J Natl Compr Canc Netw. 2022;20(3.5):BPI22-015. doi:10.6004/jnccn.2021.7262
3. National Comprehensive Cancer Network. Development and Update of Guidelines. Accessed April 15, 2023. https://www.nccn.org/guidelines/guidelines-process/development-and-update-of-guidelines
4. NIHCM Foundation. Value in health care: what’s behind variation in physicians’ use of non-recommended services in oncology care? Accessed March 29, 2023. https://nihcm.org/publications/value-in-health-care-whats-behind-variation-in-physiciansuse-of-non-recommended-services-in-oncology-care



