

Placement of a Self-Expanding Transcatheter Aortic Valve Prosthesis in the Presence of Aortic Arch Angulation
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
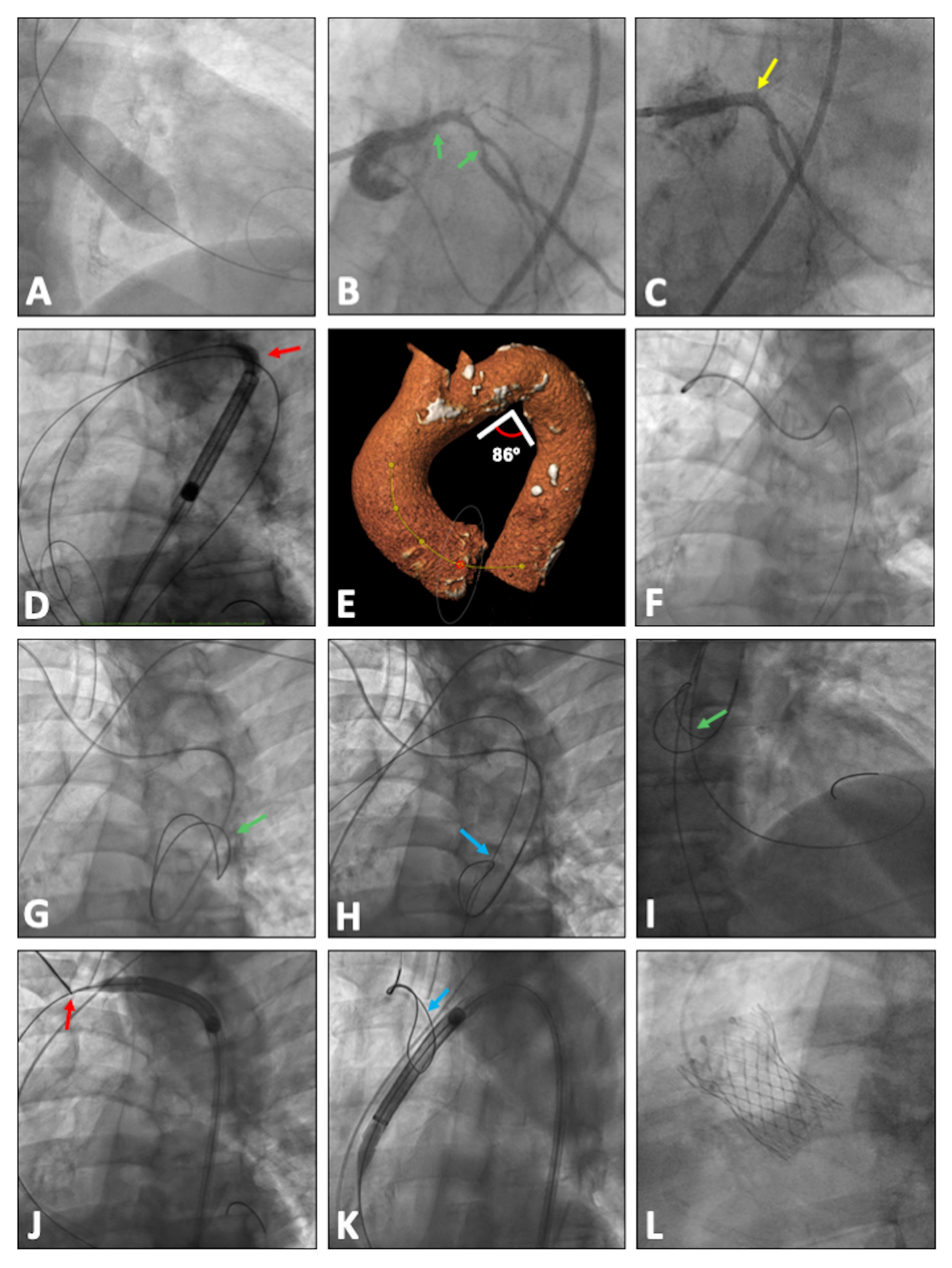
An 83-year-old man with symptomatic severe aortic valve stenosis with severe ventricular dysfunction underwent valvuloplasty with a 25-mm NuCLEUS-X balloon (B. Braun Interventional Systems) (Figure A) and percutaneous coronary intervention of the left main and circumflex arteries (left anterior descending artery presented a chronic total occlusion without viability of this territory) (Figure B and C) before being referred for transcatheter aortic valve replacement.
Through right femoral access, a high-support Lunderquist guidewire (Cook Medical) was placed into the left ventricle. An unsuccessful attempt was made to advance a 34-mm Evolut PRO+ valve (Medtronic) through the aortic arch due to a sharp angulation of the aortic arch distal to the origin of the left subclavian artery (Figure D and E). The crossing was not possible despite advancing an additional high-support guidewire (Safari2; Boston Scientific) from the left femoral artery to the aortic valvular plane with the intention of rectifying the angulation simulating the buddy-wire technique.
Through the right radial artery, a pigtail catheter was advanced over an angled Radiofocus guidewire (Terumo) to the descending thoracic aorta (Figure F). The pigtail catheter was exchanged for a Judkins Right (JR) 4, 6-French (Fr) guiding catheter. An Exeter Snare ES-35mm (AndraTec GmbH) was deployed in the descending thoracic aorta through the JR 4 catheter (Figure G; Video). A 0.032-inch guidewire was advanced from the right femoral access and passed inside the deployed snare (Figure H). With an Amplatz Left (AL) 1 catheter also passed inside the snare, the aortic valve was crossed with a straight guidewire. The high-support Lunderquist guidewire was positioned in the left ventricle crossing through the snare (Figure I). The bioprosthesis was advanced to the area of maximum angulation of the aortic arch. The snare was positioned at the level of the proximal portion of the aortic arch. Performing continuous traction with the snare on the high-support guidewire, coaxialization of the whole system was achieved, allowing it to advance through the area of maximum angulation (Figure J). Then the snare was released and withdrawn toward the distal portion of the aortic arch (Figure K). The 34-mm Evolut PRO+ valve was deployed successfully (Figure L). Once the bioprosthesis was released from the delivery system, the snare was inserted into the JR 4, 6-Fr guiding catheter and pulled out through the right radial artery.
Advancement and positioning of a self-expandable bioprosthesis through an elongated aortic arch with marked angulation is challenging with potential risk of complications. The present case shows a bailout strategy by using a 35-mm snare from the right radial artery to provide counter-traction of the high-support guidewire to coaxialize the bioprosthesis and the delivery system at the level of the aortic arch, allowing its advancement to the ascending aorta and final aortic root position.
Affiliations and Disclosures
From the 1Interventional Cardiology Unit, Department of Cardiology, Hospital del Mar. Barcelona, Spain; 2Hospital del Mar Research Institute (IMIM), Barcelona, Spain; 3Department of Medicine, Pompeu Fabra University, Barcelona, Spain; 4Centro de Investigación Biomédica en Red de Enfermedades Cardiovasculares (CIBERCV), Spain.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Hector Cubero-Gallego, MD, PhD, Hospital del Mar, Passeig Marítim 25-29, Barcelona 08003, Spain. Email: hektorkubero@hotmail.com; X: @hcuberogallego; @helenatmCARDIO; @beavaquerizo; @rutalvar3z











