Extreme Limb Salvage in a High-Risk Patient With Chronic Foot and Ankle Deformity
Medically complex cases pose specific challenges in limb preservation. This report demonstrates that with staged reconstruction, multidisciplinary care, and strong patient commitment, even “non-reconstructable” limbs may achieve a functional outcome.
Key Takeaways
- Amputation is not always inevitable. Carefully selected, motivated patients with severe comorbidities may still be candidates for successful limb salvage.
- Multidisciplinary optimization is critical. Vascular intervention, infection control, renal management, and advanced wound care are foundational to achieving healing.
- Staged, flexible surgical planning can support outcomes. These authors showcase how combining external fixation, latency for soft tissue recovery, and delayed internal fixation reduced complications and supported long-term function.

Limb salvage in high-risk patients with diabetes remains controversial, particularly in those with peripheral neuropathy, peripheral vascular disease, and end-stage renal disease (ESRD) requiring hemodialysis. Chronic infection, impaired wound healing, and compromised vascular supply significantly increase the risk of failure. As a result, these patients often receive recommendations for below-knee amputation as definitive management.
However, emerging evidence suggests that select patients may benefit from aggressive limb salvage efforts including multidisciplinary optimization. This report presents a case of extreme limb salvage in a patient with multiple systemic risk factors who declined amputation and successfully regained functional ambulation.

Patient Presentation
A 65-year-old male with a history of type 2 diabetes mellitus, peripheral neuropathy, peripheral vascular disease, chronic osteomyelitis, thrombocytopenia, and end-stage renal disease on hemodialysis presented to our hospital in November 2024 due to a malfunctioning dialysis catheter and dislodged central line. The patient was also on anticoagulation therapy for atrial fibrillation with apixaban.
He reported a multi-year history of progressive deformity, recurrent wounds, and infection involving the left foot and ankle. Previous treatment at an outside facility took place for left foot acute osteomyelitis and sepsis including prior surgical treatment. The patient had long-term intravenous cefepime and vancomycin without success. Despite worsening deformity and infection, the patient remained ambulatory in a controlled ankle motion (CAM) boot. Prior to presentation, he had been advised at outside institutions to undergo below-knee amputation, which he declined.

Upon hospital admission, he received evaluations by the emergency department and admitting medical teams and resumed intravenous antibiotics for known osteomyelitis. Upon our evaluation, the patient has multiple wounds to his left foot with a notable rigid and nonreducible equinovarus deformity.
Patient had palpable pedal pulses with baseline +1 pitting edema. Deformity and contracture were rigid. We noted two main wounds, both necrotic in nature. On examination the wounds were unstageable but immediately probed to bone intraoperatively. The first wound was at the plantar lateral aspect of the cuboid and fifth metatarsal base region, and the second was at the anterior lateral ankle at the site of the subluxed talar head.

A Closer Look at the Multidisciplinary Medical Optimization
Given the severity of comorbidities, we initiated a multidisciplinary approach:
- Vascular Surgery: Based on arterial studies and angiography, medical and interventional optimization successfully restored triphasic blood flow to the left lower extremity.
- Nephrology: This team managed inpatient hemodialysis and perioperative renal optimization.
- Infectious Disease: Directed long-term intravenous antibiotic therapy.
- Wound Care and Hyperbaric Medicine: Engaged for chronic wound management and soft tissue optimization, primarily with hyperbaric oxygen therapy. Continued treatments perioperatively to maximize soft tissue healing.

Details of the Surgical Management
We comprehensively reviewed the risks, benefits, and potential complications of the available treatment options with this patient, including that of below-knee amputation. The patient was highly motivated to undertake efforts towards limb preservation and after informed consent discussion, we proceeded with the following plan.
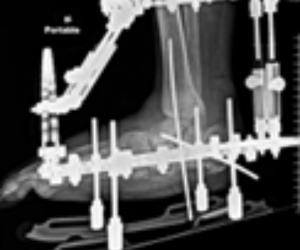
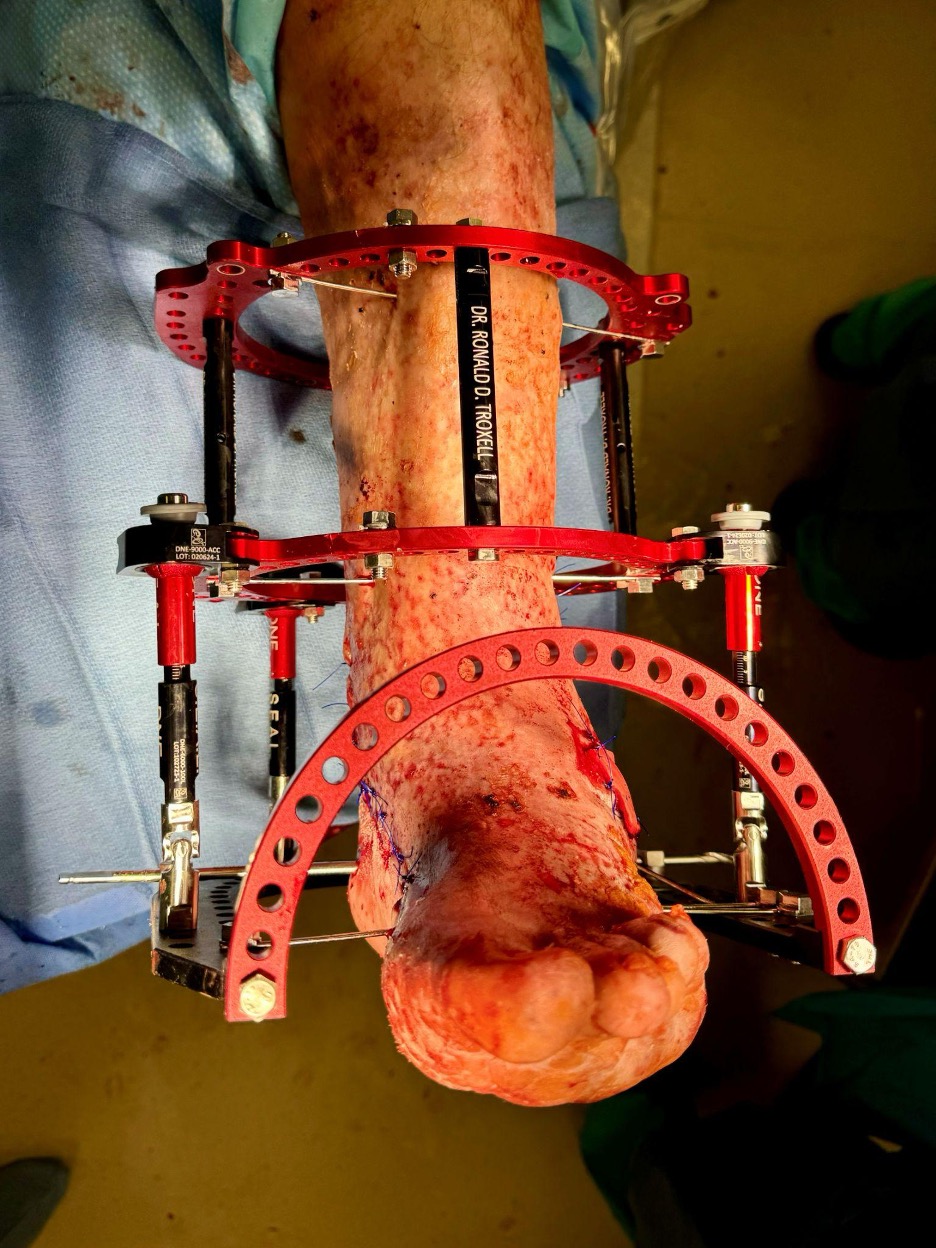
Stage 1: Deformity Correction With External Fixation
In December 2024, the patient underwent the first stage of reconstruction. This involved:
- Application of a circular external fixator
- Gradual correction of gross deformity through multiple osteotomies spanning the midfoot, hindfoot, and even fibula
- No internal fixation, given the high infection risk
This stage was complicated by multiple pin-site infections, consistent with the patient’s immunocompromised state due to diabetes and ESRD. Additionally, due to the severe medial contracture he experienced medial soft tissue necrosis in the region of the medial malleolus extending proximally 6cm.
Latency and Soft Tissue Recovery. Due to infection concerns, we ultimately removed the external fixator. The patient continued to follow protected non-weight-bearing during a prolonged latency period to allow for:
- Infection resolution
- Soft tissue recovery
- Continued wound care and hyperbaric oxygen therapy. HBOT began right away after the reconstruction (he had treatments with the external fixator on)
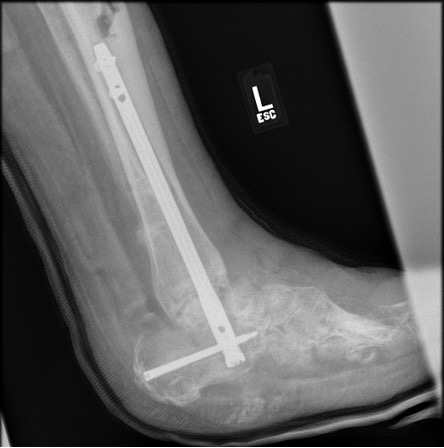
Stage 2: Definitive Arthrodesis
Once the soft tissue envelope stabilized, the patient returned to the operating room about 5 months after the first procedure for a tibiotalocalcaneal arthrodesis using a staged technique. Healing occurred slowly but without deep infection or catastrophic complication. He maintained non-weight-bearing and presented for regular follow-ups. Additional HBO treatments were required through this for successful healing.

Notes on the Patient Outcome
The entire treatment course spanned approximately 11 months. At final follow-up:
- The patient was fully ambulatory
- He utilized a custom ankle-foot orthosis (AFO) in a standard sneaker
- He had a stable, plantigrade foot and complete healing of the soft tissue envelope
- He had no evidence of recurrent ulceration or deep infection
- He continued hemodialysis, with well-controlled blood glucose levels
- The patient expressed high satisfaction and gratitude for limb preservation

Discussion and Final Thoughts
In our experience, this case underscores several key principles in extreme limb salvage:
- Patient Selection and Motivation: The patient remained ambulatory preoperatively and strongly desired limb preservation.
- Multidisciplinary Coordination: Vascular optimization, renal management, infection control, and wound care were essential to achieve this outcome.
- Staged Reconstruction: We feel that avoidance of internal fixation early reduced the risk of catastrophic infection. Additionally, being flexible to remove the external fixator and allow a latency period of casting for further soft tissue healing optimized the outcome for definitive nailing
- Acceptance of Prolonged Treatment: Limb salvage required nearly a year of careful management. Normally, for less complex and more standard deformity correction, we fin this takes at least 4 months. With the appropriately motivated patient, we have found that more complex success can be achieved.

While the risk-to-benefit ratio for this type of limb salvage effort is not appropriate for every patient, this case demonstrates that even those with multiple relative contraindications may achieve meaningful functional outcomes when treated thoughtfully.
Extreme limb salvage in patients with diabetes, ESRD, peripheral vascular disease, and chronic infection is challenging but not universally futile. With meticulous planning, multidisciplinary collaboration, and patient commitment, functional limb preservation is possible. This case supports consideration of limb salvage as a viable alternative to primary amputation in select high-risk patients.
Dr. Troxell practices in the Tampa Bay area and is the fellowship director of the Advent Health Innovative Foot and Ankle Surgery Fellowship. He discloses that he is a consultant for Enovis.
Dr. Patel is the current fellow of the Advent Health Innovative Foot and Ankle Surgery Fellowship.
References
1. Lee DJ, Schaffer J, Chen T, Oh I. Internal versus external fixation of Charcot midfoot deformity realignment. Orthopedics. 2016;39(4):e595-e601. doi:10.3928/01477447-20160526-11
2. Dayton P, Feilmeier M, Thompson M, Whitehouse P, Reimer RA. Comparison of complications for internal and external fixation for Charcot reconstruction: a systematic review. J Foot Ankle Surg. 2015;54(6):1072-5. doi: 10.1053/j.jfas.2015.06.003. Epub 2015 Jul 26. PMID: 26215548.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.