


Surgical Reconstruction of Chronic Plantar Fascia Rupture with Synthetic Polyurethane Urea-Based Matrix: A Case Study
Chronic plantar fascia rupture is uncommon and can leave patients with persistent pain and functional limitation despite conservative care. This case highlights surgical reconstruction with a synthetic polyurethane urea-based matrix as a potential option when nonoperative treatment fails.
Key Takeaways
- Chronic plantar fascial rupture may require more than conservative care. Persistent pain, weakness, and limited ambulation after immobilization, therapy, and orthotics may warrant surgical evaluation.
- Synthetic graft augmentation may support reconstruction. The described system provided structural reinforcement in a chronic rupture with compromised tissue quality.
- Functional improvement is a key measure of success. The patient’s AOFAS score improved from 62 to 80, with return to 4 miles of daily walking by 6 months.
The plantar fascia is a vital component of the foot’s anatomy, providing essential support to the arch and contributing to the overall stability and function of the lower extremity. It plays a significant role in supporting the arch of the foot and absorbing shock during activities like walking and running. While plantar fasciitis is a well-recognized condition characterized by inflammation of this structure, plantar fascial rupture represents a more severe and less commonly understood pathology.
Ruptures of this structure, although relatively uncommon, can cause severe pain and functional impairment. While exact statistics are difficult to pinpoint, it is estimated that complete ruptures of the plantar fascia account for only about 1-2% of all cases of plantar fasciitis or other plantar fascia-related conditions.1,2 Acute plantar fascia ruptures typically result from sudden injury or trauma, while chronic ruptures occur over a longer period, often associated with repetitive stress or strain. Chronic plantar fascia ruptures often present with persistent heel pain, swelling, and difficulty bearing weight, significantly affecting an individual's quality of life and daily activities. Treatment varies throughout the literature, with some authors favoring conservative treatment rather than surgical reconstruction.
In this article, we report a spontaneous total plantar fascia rupture reconstructed with a synthetic graft. By detailing the patient's journey from initial presentation through diagnosis, treatment, and follow-up, this case study aims to contribute to the understanding of plantar fascia ruptures and enhance approaches to similar cases.

Details of the Case Presentation
A 52-year-old male, working as a chief operating officer, presented to our clinic for evaluation of a chronic plantar fascial rupture of the right foot. The patient reported that while playing tennis with his son, he did not experience any sudden injury, but began to experience pain in his foot the following day. Magnetic resonance imaging (MRI) confirmed a complete tear of the plantar fascia near its insertion point on the calcaneus. Despite undergoing conservative treatment, including 2 months in a controlled ankle motion (CAM) walker, physical therapy, and orthotics, the patient did not experience prolonged relief. As a result, a year later, frustrated with his ongoing condition, he sought definitive surgical management.
His family history included unspecified heart disease, diabetes mellitus, coronary artery disease, and hypertension. He did not smoke or use recreational drugs and rarely consumed alcohol. His surgical history included hernia repair in 2023, shoulder repair in 2002, and neck surgery in 2010. His past medical history included hypertension, acid reflux, and back pain. The patient previously typically walked 4 miles per day but has been unable to since the injury. Current medications included acetaminophen-codeine, amlodipine, amoxicillin-potassium clavulanate, aspirin, atorvastatin, clobetasol, lisinopril, and silver sulfadiazine (SSD). At the initial visit, the patient was on a 7-day course of antibiotics by per his primary doctor, given a small area of redness/inflammation at the heel. That physician expressed concern for cellulitis. They also prescribed him silver sulfadiazine and clobetasol topically for burning and the inflammation sensation that he was feeling. However, the patient reported that he did not use the SSD and clobetasol and only took 3 days of the antibiotic.

Diagnostic Findings to Note
During the initial clinic visit, the physical examination revealed moderate tenderness upon palpation just distal to the plantar medial calcaneal tubercle on the right foot. Notably, the midsubstance of the plantar fascia was palpable on the left foot but not on the right. The patient was unable to perform a single heel rise on the right side. Examination showed forefoot valgus and an increased medial longitudinal arch with an everted rearfoot resting calcaneal stance position bilaterally. Range of motion was within normal limits for the ankle, subtalar, midtarsal, and first metatarsophalangeal joints bilaterally. Muscle strength was normal in all four quadrants bilaterally. His previously described MRI findings aligned with the clinical findings as outlined above.
Details on the Treatment Plan and Technique
Due to ongoing pain and failure of conservative treatment, we recommended the patient undergo surgical plantar fascial repair. After informed consent discussion with the patient, we proceeded with plans for plantar fascial reconstruction with a synthetic graft (Artelon FlexBand, Stryker).
After positioning the patient supine on the operating table, we conducted a time-out to confirm patient identity and the surgical site. He received general anesthesia with a laryngeal mask airway (LMA), followed by a field block using 20 mL of a 1:1 mixture of 0.5% bupivacaine plain and 1% lidocaine plain for local anesthesia. After sterile prep and drape, we made a curvilinear incision over the medial side of the right heel, extending distally and laterally over the central band of the plantar fascia (Figure 1). Sharp and blunt dissection continued, while controlling bleeding and protecting vital structures. We identified the plantar fascia rupture upon exposure of the structure, approximately 2 cm distal to the calcaneal tuberosity, along with 7 mm of degenerated fascia distal to the rupture (Figure 2).
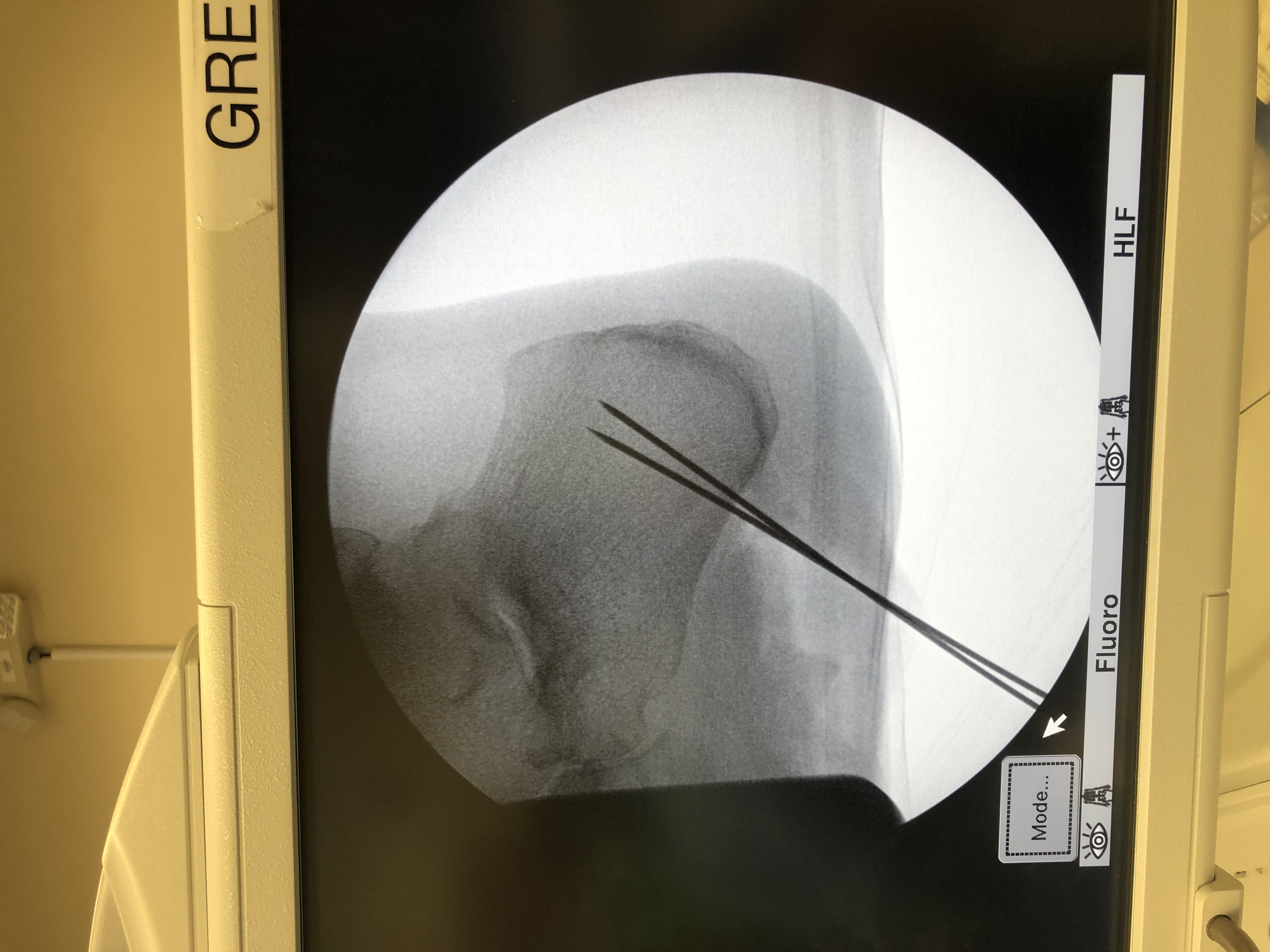
This degenerated segment was resected, and we drilled 2 holes were drilled into the calcaneus for placement of bone anchors, and confirmed via radiographic evaluation (Figures 3 and 4). We anchored the 0.5 mm graft and wove it through the plantar fascia using a Pulvertaft technique, securing it under physiological tension (Figure 5). The repair was reinforced with 2-0 Vicryl sutures and covered with amniotic tissue Clarix 1K (Biotissue) to minimize adhesions. After irrigation with saline, we approximated the edges with 2-0 polydioxanone, 3-0 polyglactin 910, and 3-0 nylon sutures. A postoperative field block consisted of 9 cc of 0.5% bupivacaine plain and 1 cc ketorolac. The foot was dressed with a microcurrent-generating antimicrobial wound dressing, transparent waterproof film, sterile 4x4s, fluffs, and a padded posterior splint in relaxed plantarflexion.
Postoperatively we advised non-weight-bearing on the affected side, with follow-up scheduled in 2 weeks. We transitioned him from splinting at 4 weeks postop, transitioning a pneumatic walking boot with a 2 cm heel lift. The patient began ankle range of motion exercises and gradually advanced to weight bearing over 2 weeks.

Examining the Outcome Measures
The patient was clinically examined for 9 months postoperatively. We used the American Orthopaedic Foot & Ankle Society (AOFAS) score modality to evaluate functional outcomes. This scoring system is a standardized tool used to evaluate pain, function, and alignment in patients with foot and ankle conditions. It consists of different scales tailored to specific regions, including the Ankle-Hindfoot, Midfoot, and Metatarsophalangeal Interphalangeal scoring systems.3
For the AOFAS Ankle-Hindfoot Score, the total score is 100 points, divided into:3
- Pain (40 points)—to assess the severity of pain
- Function (50 points)—which evaluates activities of daily living, walking distance, gait abnormality, and the need for assistive devices
- Alignment (10 points)—which measures the anatomical positioning of the foot and ankle
Higher scores indicate better function and less pain, while lower scores indicate significant impairment.3
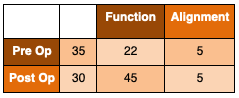
In our case, preoperatively, the patient's AOFAS Ankle-Hindfoot Score was 62 out of a total of 100 points. He scored a total of 35 points for pain, 22 points for function, and 5 points for alignment. He had an obvious gait abnormality, moderate/daily pain, and had difficulty with uneven terrains. Postoperatively, his AOFAS score increased to 80 out of 100. He scored a total of 30 points for pain, 45 points for function, and 5 points for alignment. The patient did have slight gait abnormality, mild pain, and complained of only difficulty with using stairs. Overall, our patient had a significant improvement in function outcomes measures. He no longer had any limitations with his daily activities.
This scoring system helped us assess pain levels, activity limitations, and overall foot function preoperatively and postoperatively, providing a standardized measure of patient recovery and surgical success.
Further Details on His Follow-Up Visits
Six weeks postoperatively, the patient had increased his weight-bearing; however, he noticed that there was irritation and redness to the incision site. We instructed the patient to complete a 7-day course of amoxillcin-clavulanate and to remain non-weight-bearing until the incision fully healed.
At 10 weeks, his incision was fully healed. However, he went on a 2-week vacation to Italy and returned with significant pain to his feet and calves. Pain was controlled with acetaminophen and ibuprofen at maximum dosage in a 24-hour period. There was concern for deep vein thrombosis (DVT), but the venous Doppler was unremarkable. We referred the patient was referred to physical therapy at this point.
Three weeks postop, we officially transitioned the patient into regular shoe wear, and the patient noted pain associated with exuberant scar tissue at the incision. At his 4-month follow up, he reported that he was able to walk 3 miles/day. Subsequently, at 6 months, he increased his daily activity to 4 miles/ day and was able to perform the heel rise on the operative side with no pain. Ultimately, at his 9-month follow up, the patient continued to complain of stiffness and scar tissue along the incision site. However, he transitioned to custom orthotics with a plantar fascia groove modification and expressed satisfaction with the surgery.

Discussion
Plantar fasciitis is one of the most common causes of heel pain, affecting approximately 10% of the population over their lifetime, with a higher prevalence among runners, athletes, and individuals who spend prolonged periods on their feet.1 The condition results from repetitive microtrauma and degeneration of the plantar fascia, leading to inflammation and pain, particularly at the medial calcaneal tuberosity. Conservative treatment is the mainstay of management and includes rest, activity modification, physical therapy, stretching exercises, orthotics, night splints, and nonsteroidal anti-inflammatory drugs (NSAIDs). In more refractory cases, corticosteroid injections, platelet-rich plasma (PRP) therapy, or extracorporeal shockwave therapy (ESWT) may be considered.
Surgical reconstruction of the plantar fascia is considered in cases of complete rupture, especially when conservative management fails or when there is significant loss of structural integrity, leading to persistent pain, instability, or medial arch collapse. Reconstruction techniques vary based on the extent of the rupture and tissue quality. Direct repair with non-absorbable sutures can be performed for smaller, acute tears. Larger or chronic defects may require augmentation with autografts, allografts, or synthetic grafts to restore tensile strength and maintain arch function. Tendon grafts, such as the flexor hallucis longus (FHL) or extensor hallucis longus (EHL), are commonly used for reinforcement in severe cases.
The application of synthetic grafts in Achilles tendon reconstruction has been explored in various studies. For instance, a case report detailed their use of in repairing a chronic Achilles tendon rupture, highlighting its role in providing mechanical support and facilitating tissue integration.4 Another report discussed the reconstruction of a resected Achilles tendon using the same system, emphasizing its utility in bridging significant tendon gaps and promoting functional recovery.5
Nonetheless, only a few plantar fascia rupture cases are found in the literature, and treatment strategies greatly vary. Most of the literature directly focuses on conservative management and rarely mentions repair via surgical interventions. In the study by Schaarup et al. (2020), they examined the surgical repair of complete plantar fascia ruptures in high-demand power athletes.6 The study reports that the 2 gymnasts who underwent surgical repair were able to return to their previous levels of athletic performance without recurrence of symptoms. In contrast, 3 athletes treated nonoperatively experienced prolonged recovery periods and reported persistent discomfort during high-intensity activities.6 These findings suggest that surgical repair may offer superior outcomes for athletes whose sports involve high-impact, explosive movements.
In a 2022 the case report, Chin and colleagues discuss the rare complication of iatrogenic plantar fascia rupture post-surgical release for recalcitrant plantar fasciitis.7 In this particular case, an 8-month postoperative MRI revealed a 4.2 cm gap between the distal fascia stump and the calcaneal tuberosity, indicating a complete rupture. Given the significant gap and concerns about potential retear or poor tissue healing with direct repair, the authors opted for reconstruction using an extensor hallucis longus tendon allograft. The patient experienced a gradual recovery, and after a 5-year follow-up, reported no complications. The patient's AOFAS score improved from 54 preoperatively to 85 postoperatively.7
In our case study, our patient who underwent plantar fascia reconstruction using a synthetic graft demonstrated significant improvement in functional outcomes. Preoperatively, the patient had an AOFAS score of 62, reflecting substantial pain and limited mobility despite failed conservative treatment. Following surgical intervention, the patient’s AOFAS score improved to 80, indicating enhanced function and reduced discomfort. These results suggest that this system is a viable option for reconstructing chronic plantar fascia ruptures, particularly in cases where nonsurgical management has been unsuccessful.
In Conclusion
Overall, we found that many authors highlight that while nonoperative treatments are commonly preferred for plantar fascia ruptures, surgical intervention may be beneficial for athletes involved in sports requiring significant plyometric activity. Surgical repair can facilitate a quicker return to pre-injury performance levels, particularly in cases where the demands of the sport place substantial stress on the plantar fascia.
Given the success of similar grafts in Achilles tendon repair, we feel their application in plantar fascia reconstruction presents a promising avenue. In cases of chronic or iatrogenic plantar fascia ruptures with substantial defects, where primary repair is not feasible, these grafts could serve as an effective scaffold. By providing immediate mechanical support and promoting tissue regeneration, these grafts may help restore the structural integrity and function of the plantar fascia, potentially leading to improved clinical outcomes. In our experience with this case, we conclude that allograft reconstruction can effectively restore the function and mechanical strength of the plantar fascia in cases of chronic ruptures.
Dr. Peña Felix is a resident at the Scripps Hospital San Diego Residency Program.
Dr. Cullen is the program director of the Scripps Hospital San Diego Residency Program and has a private practice in San Diego.
The authors have no non-financial or commercial, proprietary, or financial interest in the products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
References
1. Debus F, Eschbach D, Ruchholtz S, Peterlein CD. Rupture of plantar fascia: Current standard of therapy: A systematic literature review. Foot Ankle Surg. 2020 Jun;26(4):358-362.
2. Lee HS, Choi YR, Kim SW, Lee JY, Seo JH, Jeong JJ. Risk factors affecting chronic rupture of the plantar fascia. Foot Ankle Int. 2014 Mar;35(3):258-63.
3. Ibrahim T, Beiri A, Azzabi M, Best AJ, Taylor GJ, Menon DK. Reliability and validity of the subjective component of the American Orthopaedic Foot and Ankle Society clinical rating scales. J Foot Ankle Surg. 2007 Mar-Apr;46(2):65-74. doi: 10.1053/j.jfas.2006.12.002. PMID: 17331864.
4. Ahmad J, Jones K, Raikin SM. Treatment of chronic Achilles tendon ruptures with large defects. Foot Ankle Spec. 2016 Oct;9(5):400-8.
5. Shival T, M. Shahril. Department of Orthopedic, Hospital Sultan Abdul Aziz Shah, UPM, Serdang Selangor. (2022). Using Artelon As An Alternative Graft In Case Of Chronic Rupture Achilles Tendon With Huge Gap Defect. Malaysian Orthopaedic Journal, 17(Supplement A).
6. Schaarup SO, Burgaard P, Johannsen FE. Surgical repair of complete plantar fascia ruptures in high-demand power athletes: an alternative treatment option. J Foot Ankle Surg. 2020 Jan-Feb;59(1):195-200.
7. Chin CM, Tang HM, Yang KC, Chen IH, Wang CC. Surgical reconstruction with tendon allografting following iatrogenic rupture of the plantar fascia: a case report. Medicina (Kaunas). 2022 Aug 10;58(8):1075.
8. Stecco C, Corradin M, Macchi V, Morra A, Porzionato A, Biz C, De Caro R. Plantar fascia anatomy relationship with Achilles tendon and paratenon. J Anat. 2013 Dec;223(6):665-76.
© 2026 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Podiatry Today or HMP Global, their employees, and affiliates.






