


Percutaneous Management of Calcaneal Fractures: Evolution, Indications, and Surgical Pearls
This review explores the evolution of minimally invasive management, patient selection criteria, surgical pearls, and evidence supporting modern percutaneous techniques.
Key Takeaways
1. Percutaneous fixation may reduce soft tissue complications without sacrificing outcomes. Contemporary evidence suggests that minimally invasive and percutaneous approaches can provide comparable functional results to traditional extensile lateral ORIF while significantly lowering complication rates in appropriately selected patients.
2. Success depends on careful patient and fracture selection. Percutaneous techniques are best suited for select displaced intra-articular calcaneal fractures, and patient populations that may derive particular benefit from these less invasive approaches, while highly comminuted fractures often require more direct visualization.
3. Restoring overall calcaneal morphology is more important than pursuing perfect articular reduction. Modern management emphasizes correction of calcaneal height, width, length, alignment, and hindfoot biomechanics while preserving the soft tissue envelope. This relies on meticulous fluoroscopic assessment, strategic fixation, and a willingness to convert to a limited open approach when indirect reduction cannot adequately restore anatomy.
Calcaneal fractures remain among the most challenging injuries in foot and ankle surgery, often resulting in prolonged disability, chronic pain, and variable functional outcomes. Open reduction and internal fixation (ORIF), particularly via the extensile lateral approach, has historically been the standard for displaced intra-articular fractures due to its ability to achieve anatomic reduction of the posterior facet. However, this approach carries a substantial risk of soft tissue complications—including wound dehiscence, infection, and delayed healing—especially in patients with comorbidities such as diabetes, smoking history, and peripheral vascular disease.1,2
These limitations have driven a shift toward less invasive strategies that prioritize preservation of the soft tissue envelope while maintaining acceptable fracture reduction. Minimally invasive and percutaneous techniques have emerged as effective alternatives, with contemporary evidence demonstrating lower wound complication rates and comparable functional outcomes in appropriately selected patients.3–5
Evolution of Calcaneal Fracture Management
The evolution of calcaneal fracture management reflects a broader shift from purely anatomic restoration toward a balance of mechanical and biologic considerations. The extensile lateral approach, while offering excellent visualization of the posterior facet, is associated with significant soft tissue morbidity.1,3 In response, less invasive approaches such as the sinus tarsi approach were developed, allowing limited visualization with improved soft tissue preservation.
Further advances in indirect reduction techniques and intraoperative imaging have enabled the development of percutaneous fixation strategies, which minimize surgical exposure while maintaining acceptable alignment.3,6 Although arthroscopy-assisted techniques were introduced to improve visualization and reduction of the posterior facet—and have been shown to enhance reduction accuracy—current evidence has not consistently demonstrated clear superiority in functional outcomes compared to percutaneous fixation alone.
This likely reflects the greater clinical importance of restoring overall calcaneal morphology rather than achieving perfect articular congruity. Contemporary practice increasingly emphasizes restoration of global calcaneal structure, with recognition that preservation of the soft tissue envelope may be equally important in determining outcomes. As such, modern management favors a tailored approach that integrates fracture characteristics, soft tissue status, and patient-specific risk factors.2,4
Indications and Patient Selection
Successful percutaneous management of calcaneal fractures begins with appropriate patient selection. These techniques are most effective in fracture patterns where indirect reduction can reliably restore alignment without the need for extensive open visualization. Contemporary evidence supports their use in select displaced intra-articular fractures, particularly Sanders type II and certain type III patterns, where fragment geometry allows for controlled manipulation and stabilization.4,7
In clinical practice, patient-specific factors often play an equally important role. Individuals with compromised soft tissue envelopes, including those with diabetes, peripheral vascular disease, or a history of smoking, may derive particular benefit from percutaneous approaches due to the significantly reduced risk of wound complications.1,2 Additionally, tongue-type fractures represent a critical indication, as early percutaneous reduction can relieve posterior skin tension and prevent progression to soft tissue necrosis.
Equally important is recognizing when percutaneous techniques may not be appropriate. Highly comminuted fractures, particularly Sanders type IV injuries, often require direct visualization to achieve acceptable articular reduction. Similarly, fractures with significant loss of calcaneal height, marked varus deformity, or lateral wall blowout may not be amenable to indirect techniques alone. In these cases, a limited open approach may become necessary to restore anatomy. The decision-making process is therefore nuanced and requires careful assessment of both radiographic and clinical factors.
Surgical Techniques
The basis of percutaneous fixation lies within the principles of indirect reduction, ligamentotaxis, and stable fixation. Timing plays a critical role, as early intervention—typically within 7 to 10 days of injury—facilitates fragment mobility and effective use of ligamentotaxis. Delayed intervention beyond this period may result in early fracture consolidation and soft tissue contracture, limiting reduction potential.
One initiates reduction by restoring the position of the calcaneal tuberosity. Insertion of a percutaneous Schanz pin or Steinmann pin into the tuberosity and used as a joystick works to correct varus deformity, restore length, and reestablish alignment. This step is critical, as tuberosity malalignment can compromise overall hindfoot biomechanics.
Subsequent reduction of the posterior facet takes place through indirect manipulation under fluoroscopic guidance. In select cases, one may choose to utilize a limited sinus tarsi approach to assist with visualization while maintaining a minimally invasive strategy.3,6
Fluoroscopy used systematically throughout the procedure, including lateral, axial (Harris), and Broden’s views can confirm restoration of alignment, calcaneal morphology, and articular congruity. Fixation is typically with percutaneous cannulated screws placed strategically to maintain reduction and provide structural stability. Careful attention to screw trajectory is essential to avoid intra-articular penetration and ensure adequate fixation.

Outcomes and Evidence
A growing body of literature supports the use of minimally invasive and percutaneous techniques in calcaneal fracture management. Systematic reviews and meta-analyses have demonstrated significantly lower rates of wound complications compared to extensile lateral ORIF, with comparable functional outcomes in appropriately selected patients.3-5,7
Comparative studies further support these findings. For example, percutaneous screw fixation has demonstrated outcomes comparable to minimally invasive plating techniques, with reduced operative time and decreased soft tissue morbidity.8
However, these techniques are not without limitations. Because reduction is indirect, there is an inherent risk of incomplete restoration of the posterior facet, particularly in more complex fracture patterns. Importantly, this risk appears to be mitigated by careful technique, appropriate patient selection, and meticulous intraoperative imaging.6,7

Complications and Pitfalls
While percutaneous techniques reduce soft tissue complications, they introduce unique challenges. The most significant is malreduction of the posterior facet, which may predispose to subtalar arthritis and long-term functional impairment. This risk is heightened when one does not critically evaluate the fluoroscopic imaging.
Loss of fixation may occur with suboptimal screw placement or poor bone quality. Additionally, sural nerve irritation may result from percutaneous instrumentation.
A key pitfall is persistence with percutaneous techniques despite inadequate reduction. Surgeons should maintain a low threshold to convert to a limited open approach when necessary. The primary goal remains restoration of alignment and function rather than strict adherence to a minimally invasive technique.
Surgical Pearls
Successful percutaneous management requires thoughtful integration of technique and judgment. Fracture patterns with larger, well-defined fragments are most amenable to indirect reduction, while patient factors such as diabetes, smoking, and vascular disease further support a minimally invasive approach.
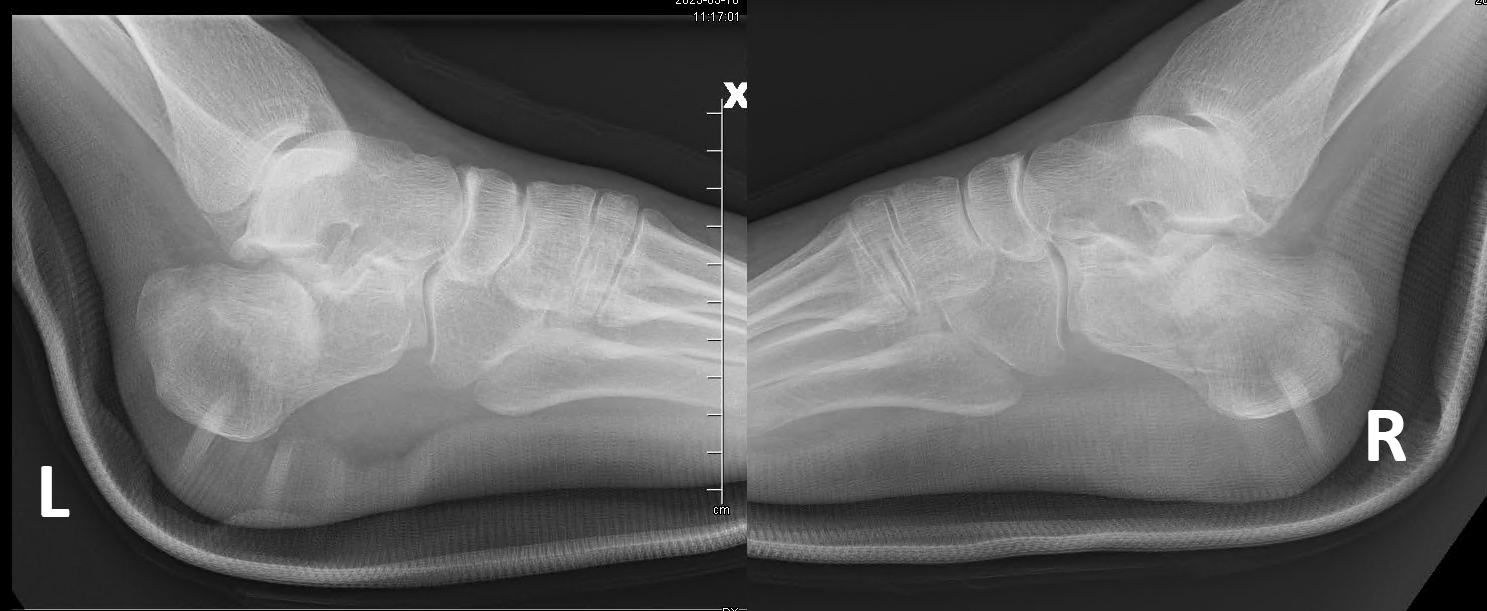
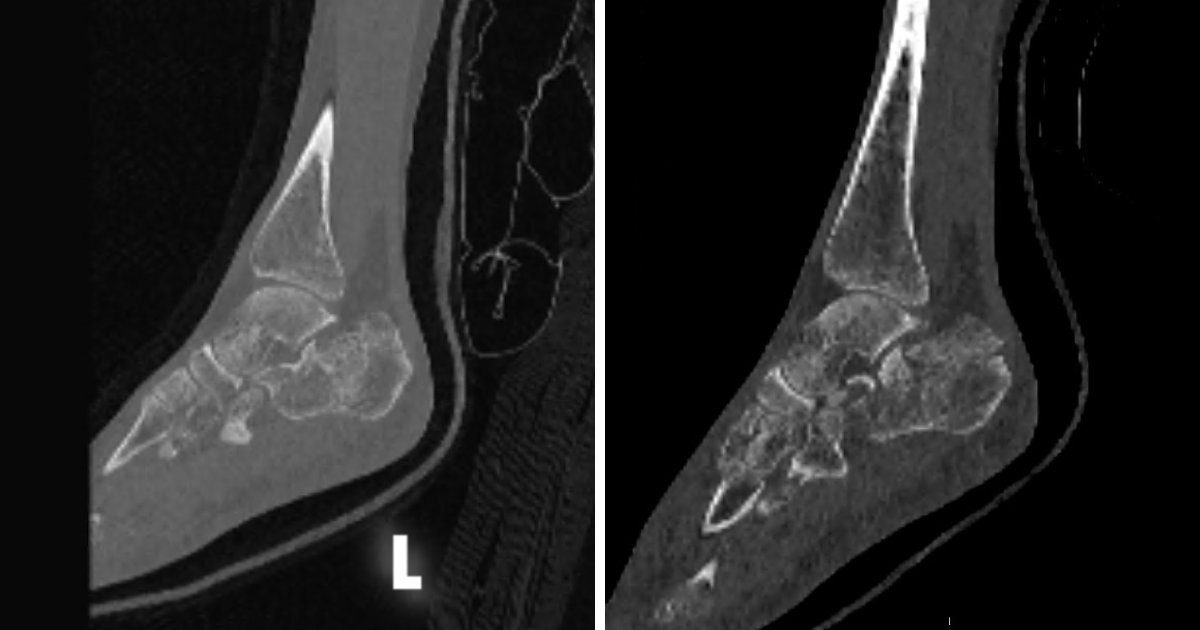
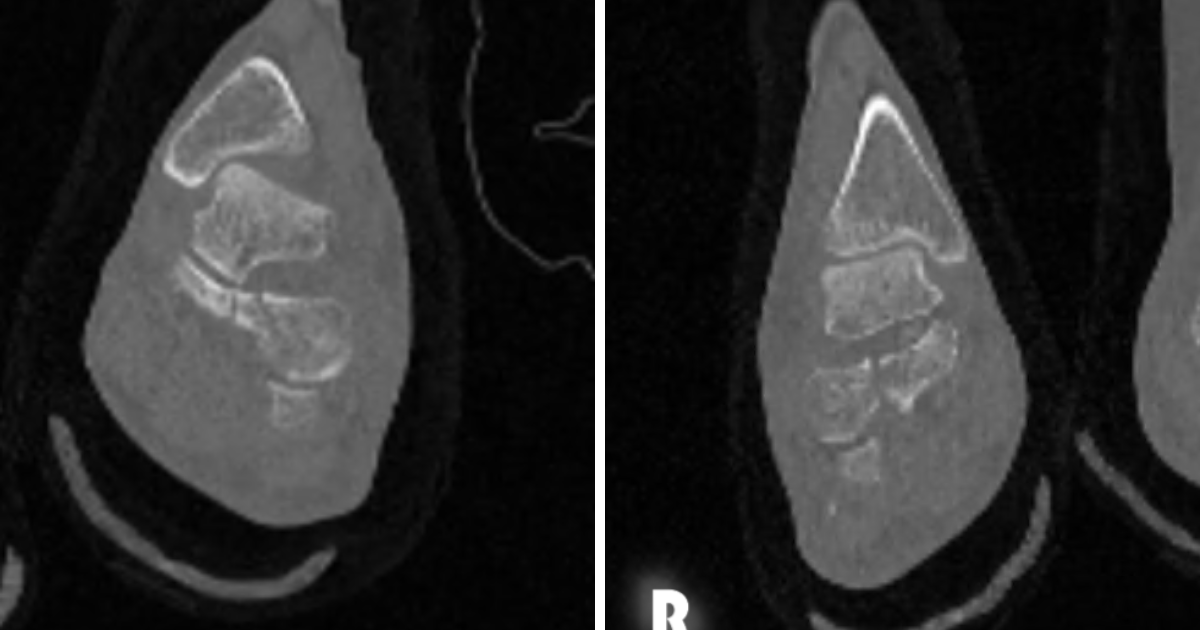
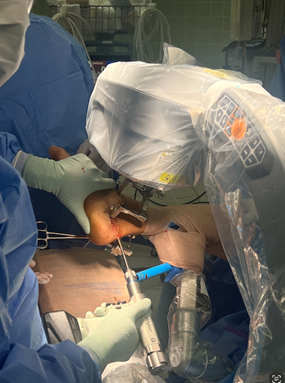
Preoperative planning should include conventional radiographs supplemented by computed tomography (CT) with 3-dimensional reconstruction to guide reduction strategy and fixation planning. Patient positioning has evolved, and while the lateral decubitus position has historically been standard, the use of modern limb positioners (eg, Trimano (Arthrex) or equivalent systems) improves intraoperative flexibility and fluoroscopic access.
Restoration of overall calcaneal morphology should remain the primary objective, as functional outcomes are closely tied to correction of deformity and restoration of hindfoot biomechanics. Surgeons should also employ systematic, multiview fluoroscopic assessment to avoid subtle malreductions and maintain a low threshold for conversion when necessary.
Conclusion
Percutaneous fixation represents a significant advancement in the management of calcaneal fractures, offering reduced soft tissue morbidity while achieving satisfactory mechanical restoration. When applied to appropriately selected patients, these techniques provide outcomes comparable to traditional open approaches.
This evolution reflects a broader shift toward individualized, biology-conscious surgical care. Ultimately, success depends on careful patient selection, technical precision, and a comprehensive understanding of fracture biomechanics.
Dr. Dei-Tumi is a second-year resident in the Department of Podiatric Surgery, Cambridge Health Alliance, Cambridge, MA.
Dr. Theodoulou is an Attending Physician and the Chief of the Department of Orthopedics, Foot and Ankle Division, Cambridge Health Alliance, Cambridge, MA. He is also an Assistant Professor of Surgery at Harvard Medical School in Cambridge, MA.
The authors have no non-financial or commercial, proprietary, or financial interest in the products or companies described in the manuscript. The author(s) did not receive grants or a consultant honorarium to conduct the study, write the manuscript or otherwise assist in the development of the above-mentioned manuscript.
The authors disclose that Artificial intelligence (AI) was used as a writing support tool to assist with language refinement, organization, and editing. All clinical content, surgical decision-making, and final manuscript preparation were performed and reviewed by the authors.
References
1. Ding L, He Z, Xiao H, Chai L, Xue F. Risk factors for postoperative wound complications of calcaneal fractures following plate fixation. Foot Ankle Int. 2013 Sep;34(9):1238-44. doi: 10.1177/1071100713484718. Epub 2013 Apr 5. PMID: 23564422.
2. Salameh M, Al-Hashki L, Al-Juboori S, Rayyan R, Hantouly A, Blankenhorn B. Management of displaced intra-articular calcaneal fractures; current concept review and treatment algorithm. Eur J Orthop Surg Traumatol. 2023 May;33(4):779-785. doi: 10.1007/s00590-022-03264-5. Epub 2022 Apr 16. PMID: 35429277.
3. Zeng Z, Yuan L, Zheng S, Sun Y, Huang F. Minimally invasive versus extensile lateral approach for sanders type II and III calcaneal fractures: A meta-analysis of randomized controlled trials. Int J Surg. 2018 Feb;50:146-153. doi: 10.1016/j.ijsu.2017.12.034. Epub 2018 Jan 11. PMID: 29337175.
4. Allegra PR, Rivera S, Desai SS, Aiyer A, Kaplan J, Gross CE. Intra-articular calcaneus fractures: current concepts review. Foot Ankle Orthop. 2020 Jul 28;5(3):2473011420927334. doi: 10.1177/2473011420927334. PMID: 35097384; PMCID: PMC8564939.
5. Lewis SR, Pritchard MW, Solomon JL, Griffin XL, Bruce J. Surgical versus non-surgical interventions for displaced intra-articular calcaneal fractures. Cochrane Database Syst Rev. 2023 Nov 7;11(11):CD008628. doi: 10.1002/14651858.CD008628.pub3. PMID: 37933733; PMCID: PMC10628987.
6. Gołos J, Kwiatkowski K, Piekarczyk P, Cieślik P, Rowicki K, Waliński T. Long-term results of operative treatment of calcaneal fractures. Ortop Traumatol Rehabil. 2015 Mar-Apr;17(2):163-74. doi: 10.5604/15093492.1157093. PMID: 26248761.
7. Zhao B, Xu X, Sun Q, et al. Comparison between screw fixation and plate fixation via sinus tarsi approach for displaced intra-articular calcaneal fractures: a systematic review and meta-analysis. Arch Orthop Trauma Surg. 2024 Jan;144(1):59-71. doi: 10.1007/s00402-023-05041-3. Epub 2023 Aug 25. PMID: 37624429.
8. Cao Y, Xu X, Guo Y, et al. Percutaneous cannulated screw fixation vs. plating with minimally invasive longitudinal approach after closed reduction for intra-articular tongue-type calcaneal fractures: a retrospective cohort study. Front Surg. 2022 Apr 4;9:854210. doi: 10.3389/fsurg.2022.854210. PMID: 35445076; PMCID: PMC9013838.
9. Rammelt S, Zwipp H. Calcaneus fractures: facts, controversies and recent developments. Injury. 2004 May;35(5):443-61. doi: 10.1016/j.injury.2003.10.006. PMID: 15081321.






