

Transcatheter Management of Acquired Atresia of Aorta
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.
A 24-year-old man was referred to our tertiary care center for the management of uncontrolled hypertension secondary to severe coarctation of the aorta (CoA). On evaluation, a 2-dimensional echocardiogram showed a bicuspid aortic valve, moderate aortic regurgitation, normal left ventricular systolic function, and no antegrade flow in the descending aorta, suggestive of tight CoA. Computed tomography revealed very tight coarctation 8-mm distal to the left subclavian artery with an isthmus of size 13 mm and multiple collaterals supplying the descending aorta.
The patient was taken for cardiac catheterization; under local anesthesia, 6-French (Fr) left radial artery and 7-Fr right femoral artery (RFA) access was taken under ultrasound guidance. The proximal aorta had a blood pressure of 182/78 mm Hg, and the femoral artery had a blood pressure of 82/69 mm Hg, suggestive of a 100 mm Hg gradient across the CoA. In the initial attempt, we failed to cross the CoA segment from both the femoral and radial approaches despite using multiple catheters and guidewires, including 0.014-inch coronary wires. After a discussion with the patient and the heart team, we decided to perform perforation of the atretic segment.
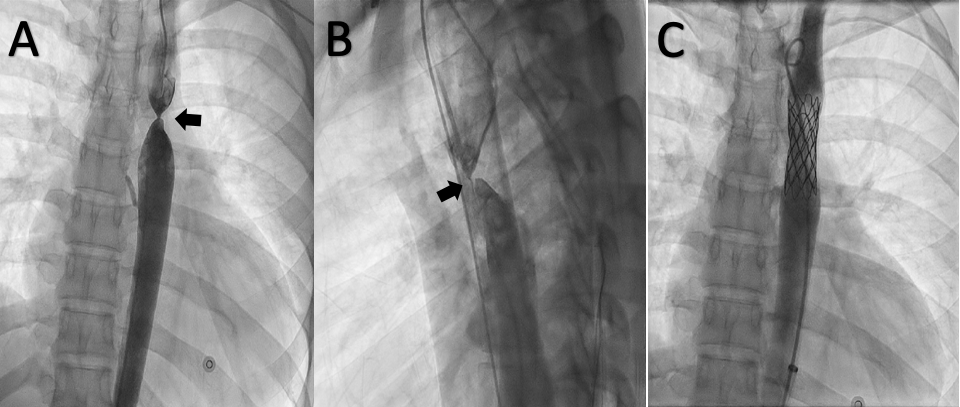
Simultaneous antegrade and retrograde aortogram showed complete occlusion with no communication between the 2 segments, suggestive of functional aortic atresia (Figure, A & B; Video 1). A Mullins dilator (Medtronic) was parked in the distal segment of the CoA. A Brockenbrough needle (Medtronic) was taken to the distal end of the Mullins dilator. The hard end of a 0.014-inch Runthrough wire (Terumo) was passed through the Brockenbrough needle and perforated the atretic segment, which was confirmed by an angiogram in the proximal segment in 2 orthogonal views (Videos 2, 3). The atretic segment was punctured with the Brockenbrough needle over the 0.014-inch wire.
Later, the Mullins dilator was pushed across the atresia and contrast was injected through it to confirm the position. The CoA segment was dilated with an 8 x 30-mm Tyshak II balloon (NuMED) and the 7-F RFA sheath was upgraded to a 14-Fr Mullins sheath after predilating with 10- and 12-Fr dilators (Video 4). A 4.5 x 8-mm zig-covered Cheatham-Platinum (CP) stent (NuMED) was crimped over a 5 cm x 15-mm Z MED II balloon (B. Braun), and the stent was deployed at 8 atm across the CoA segment (Video 5). The post-stent deployment angiogram showed no narrowing across the CoA segment and no leak (Figure, C; Video 6). The gradient across the CoA segment disappeared completely. The patient was off antihypertensives and doing well at 2-month follow-up.
Acquired aortic atresia occurs because of longstanding and severe CoA. It should not be confused with an interrupted aortic arch, as in the latter there is no continuity between the segments. Proper patient selection and planning is imperative to successfully intervene in such patients.
Affiliations and Disclosures
From the Department of Cardiology, All India Institute of Medical Sciences, New Delhi, India.
Disclosures: The authors report no financial relationships or conflicts of interest regarding the content herein.
Address for correspondence: Sivasubramanian Ramakrishnan, MD, DM, Department of Cardiology, AIIMS, New Delhi, India. Email: ramaaiims@gmail.com











