

Primary Malignant Pericardial Mesothelioma Presenting as Effusive-Constrictive Pericarditis
ABSTRACT: Effusive-constrictive pericarditis is a clinical hemodynamic syndrome characterized by constriction of the heart by the visceral pericardium in the presence of a tense pericardial effusion. The hallmark of effusive-constrictive pericarditis is the persistence of elevated right atrial pressures and ventricular interdependence after relief of the elevated intrapericardial pressures. The present report discusses the unique case of a 46-year-old white female who presented with dyspnea on exertion and chest tightness in the setting of an effusive-constrictive pericarditis. The patient was subsequently diagnosed with primary malignant pericardial mesothelioma, an extremely rare neoplasm with a very poor prognosis.
J INVASIVE CARDIOL 2011;23:E197–E199
Key words: pericarditis, effusive-constrictive pericarditis, pericardial mesothelioma
______________________________________
Case Report. This case presents a 46-year-old white female, a former smoker with a past medical history of non-insulin dependent diabetes, polycystic ovarian syndrome and depression. She is a retired insurance agent with a remote history of occupational exposure to asbestos. The patient was seen by her primary care physician and sent to the emergency room at an outside hospital with a 3-day history of dyspnea on exertion and chest tightness. The dyspnea worsened on minimal activity and was progressive in nature. Chest tightness was midsternal in location, without radiation, and worsened with deep inspiration.
On triage, the patient was hypertensive with a blood pressure of 141/107 mmHg, tachycardiac with a pulse rate of 107 bpm. Physical exam was remarkable only for distant heart sounds without any jugular venous distension. Laboratory analysis revealed a troponin T of 0.06 ng/ml, with a normal CPK and CK-MB. Electrocardiogram done in the emergency room showed sinus tachycardia with a ventricular rate of 104 bpm and low voltage complexes. Chest x-ray demonstrated cardiomegaly and pulmonary vascular congestion. A computerized tomography (CT) scan of the chest ruled out pulmonary embolism and aortic dissection, but found a large pericardial effusion. A transthoracic echocardiogram (TTE) confirmed presence of a moderate-sized pericardial effusion with right artial collapse in systole and significant respiratory variation of the mitral valve inflow pattern.
 Given the TTE findings, which were suggestive of early tamponade physiology, the patient underwent an emergent pericardial window via subxiphoid approach on day 1 of hospitalization. A follow-up postoperative TTE showed presence of constrictive physiology as suggested by paradoxical septal wall motion and respiratory variation of the mitral inflow and cardiac output. The patient underwent a simultaneous right and left heart catheterization, which demonstrated right artial pressure of 21 mmHg, right ventricular pressures of 55/22 mmHg, a pulmonary artery systolic pressure of 56 mmHg, with left ventricular end diastolic pressure of 22 mmHg and prominent X and Y descent of the right atrial pressure tracing, marked respiratory variation in pressures and equalization of chamber pressures during diastole, and the dip-plateau morphology of left intraventricular pressure (Figure 1).
Given the TTE findings, which were suggestive of early tamponade physiology, the patient underwent an emergent pericardial window via subxiphoid approach on day 1 of hospitalization. A follow-up postoperative TTE showed presence of constrictive physiology as suggested by paradoxical septal wall motion and respiratory variation of the mitral inflow and cardiac output. The patient underwent a simultaneous right and left heart catheterization, which demonstrated right artial pressure of 21 mmHg, right ventricular pressures of 55/22 mmHg, a pulmonary artery systolic pressure of 56 mmHg, with left ventricular end diastolic pressure of 22 mmHg and prominent X and Y descent of the right atrial pressure tracing, marked respiratory variation in pressures and equalization of chamber pressures during diastole, and the dip-plateau morphology of left intraventricular pressure (Figure 1).
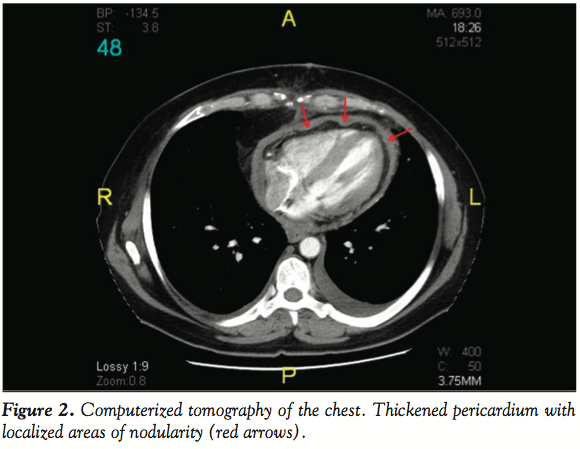 A repeat CT scan of the chest done on day 6 revealed a moderate pericardial effusion with nodularity of the pericardium (Figure 2), without evidence of any pleural lesions. The CT scan findings were suggestive of a pericardial neoplasm and the patient underwent a pericardiectomy on the beating heart without cardiopulmonary bypass. In the operating room, the patient was found to have a thickened parietal pericardium with a small-sized pericardial effusion and a thick, adherent visceral pericardium.
A repeat CT scan of the chest done on day 6 revealed a moderate pericardial effusion with nodularity of the pericardium (Figure 2), without evidence of any pleural lesions. The CT scan findings were suggestive of a pericardial neoplasm and the patient underwent a pericardiectomy on the beating heart without cardiopulmonary bypass. In the operating room, the patient was found to have a thickened parietal pericardium with a small-sized pericardial effusion and a thick, adherent visceral pericardium.
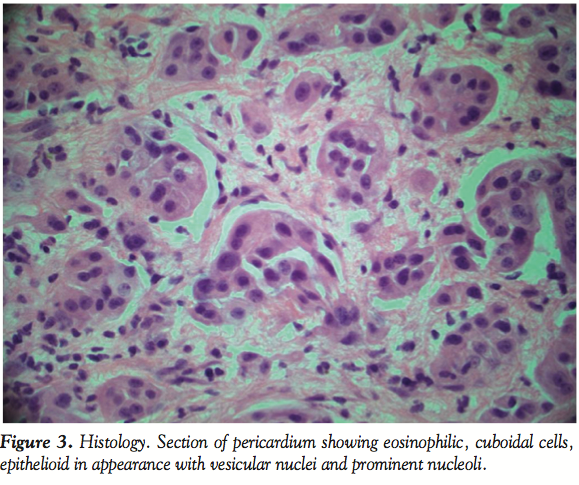 Pathology reports revealed vesicular nuclei with prominent nucleoli (Figure 3) and immunohistochemical staining confirming mesothelial origin of the tumor. The patient gradually recovered and was eventually discharged with plans for prompt initiation of outpatient chemotherapy.
Pathology reports revealed vesicular nuclei with prominent nucleoli (Figure 3) and immunohistochemical staining confirming mesothelial origin of the tumor. The patient gradually recovered and was eventually discharged with plans for prompt initiation of outpatient chemotherapy.
Discussion. Effusive-constrictive pericarditis is an uncommon pericardial syndrome that was first described in the 1960s. In a prospective study of 1,184 patients with pericarditis, Sagrista-Sauldea et al reported that 6.9% of 218 patients with tamponade had confirmed effusive-constrictive pericarditis.1 The most common cause of effusive-constrictive pericarditis is idiopathic, while cases can be secondary to irradiation, cardiac surgery, uremia, malignancy, or infections like tuberculosis.
Our patient was initially found to have a pericardial effusion with early tamponade physiology. The pressure tracings from a right and left heart catheterization done after relieving the effusion unveiled equalization of diastolic pressures in the 4 cardiac chambers, which was more prominent during inspiration (Figure 1). As noted in Figure 1, there was also evidence of discordance of pressure changes with respiration in the 2 ventricles, a phenomenon called ventricular interdependence, and the presence of a dip and plateau configuration of left ventricular tracings (square root sign) following a premature ventricular complex. All of the above hemodynamic findings are characteristic of a constrictive physiology and with the presence of the prior effusion, highly suggestive of an effusive-constrictive pericarditis in our patient. It is important to note that it is not uncommon for effusive-constrictive pericarditis to present with tamponade at initial presentation. In one series, tamponade was the initial presentation in more than half the cases.1 The etiology of this unusual form of pericarditis in our patient was identified as primary malignant pericardial mesothelioma (PMPM). This is a very unusual presentation of pericardial mesothelioma and, as per our literature review, is the first case of its kind.
PMPM is an extremely rare neoplasm with a reported incidence of < 0.0022% in a large necropsy series.2 However, it is also the most common primary pericardial tumor. There is a possible association with asbestos exposure, but this is seen only in cases with coexistent asbestos-related pleural disease.3 The onset of symptoms is insidious, with presentation usually occurring late in the course of the disease. Common presentations include constrictive pericarditis,4 cardiac tamponade,5 and heart failure. Other complications such as distant metastasis, heart block,6 and tumor embolism causing neurological deficits7 have also been reported. Upon review of the literature, effusive-constrictive pericarditis as a complication of PMPM has never been reported. CT, magnetic resonance imaging, and two-dimensional echocardiography are useful in identifying the tumor and its extent. Histology and immunohistochemistry with positive staining for calretinin, cytokeratin 5/6, and mesothelin of the biopsy sample are necessary to confirm the diagnosis.
The overall prognosis of PMPM is very poor.8 The response to radiation is poor. Cyclical combination chemotherapy with doxorubicin, vincristine, and cyclophosphamide may reduce the tumor mass.9 Surgical interventions such as pericardiectomy may help cure local tumors, or provide palliative care by decreasing disease burden and offering symptom relief.
References
- Sagristà-Sauleda J, Angel J, Sánchez A, et al. Effusive-constrictive pericarditis. N Engl J Med 2004;350:469–475.
- Gössinger HD, Siostrzonek P, Zangeneh M, et al. Magnetic resonance imaging findings in a patient with pericardial mesothelioma. Am Heart J 1988;115:1321–1322.
- Yilling FP, Schlant RC, Hertzler GL, Krzyaniak R. Pericardial mesothelioma. Chest 1982;81:520–523.
- Suman S, Schofield P, Large S. Primary pericardial mesothelioma presenting as pericardial constriction: A case report. Heart 2004;90:E4.
- Lagrotteria DD, Tsang B, Elavathil LJ, Tomlinson CW. A case of primary malignant pericardial mesothelioma. Can J Cardiol 2005;21:185–187.
- Fazekas T, Tiszlavicz L, Ungi I. Primary malignant pericardial mesothelioma [in Hungarian]. Orv Hetil 1991;132:2677–2680.
- Szczechowski L, Janiec K. Pericardial mesothelioma as a very rare cause of recurrent cerebral emboli [in Polish]. Wiad Lek 1992;45:857–861.
- Kralstein J, Frishman W. Malignant pericardial diseases: Diagnosis and treatment. Am Heart J 1987;113:785–790.
- Nambiar CA, Tareif HE, Kishore KU, et al. Primary pericardial mesothelioma: One-year event-free survival. Am Heart J 1992;124:802–803.
______________________________________
From the Englewood Hospital Medical Center, Englewood, New Jersey.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted November 12, 2010, provisional acceptance given December 21, 2010, final version accepted January 12, 2011.
Address for correspondence: Parikshit Sharma, MD, MPH, 2200 Benjamin Franklin Pkwy, Apt. W0911, Philadelphia, PA 19130. Email: psharma.doc@gmail.com













